
Abstract

What Is SADI?
There is quite a bit of discussion around the single anastomosis duodeno-ileostomy (SADI), sometimes known as SADI-S to clarify that a sleeve gastrectomy (SG) is part of the operation. There have been other descriptive names attributed to this operation, but all seem to have finally converged to this final name, SADI.
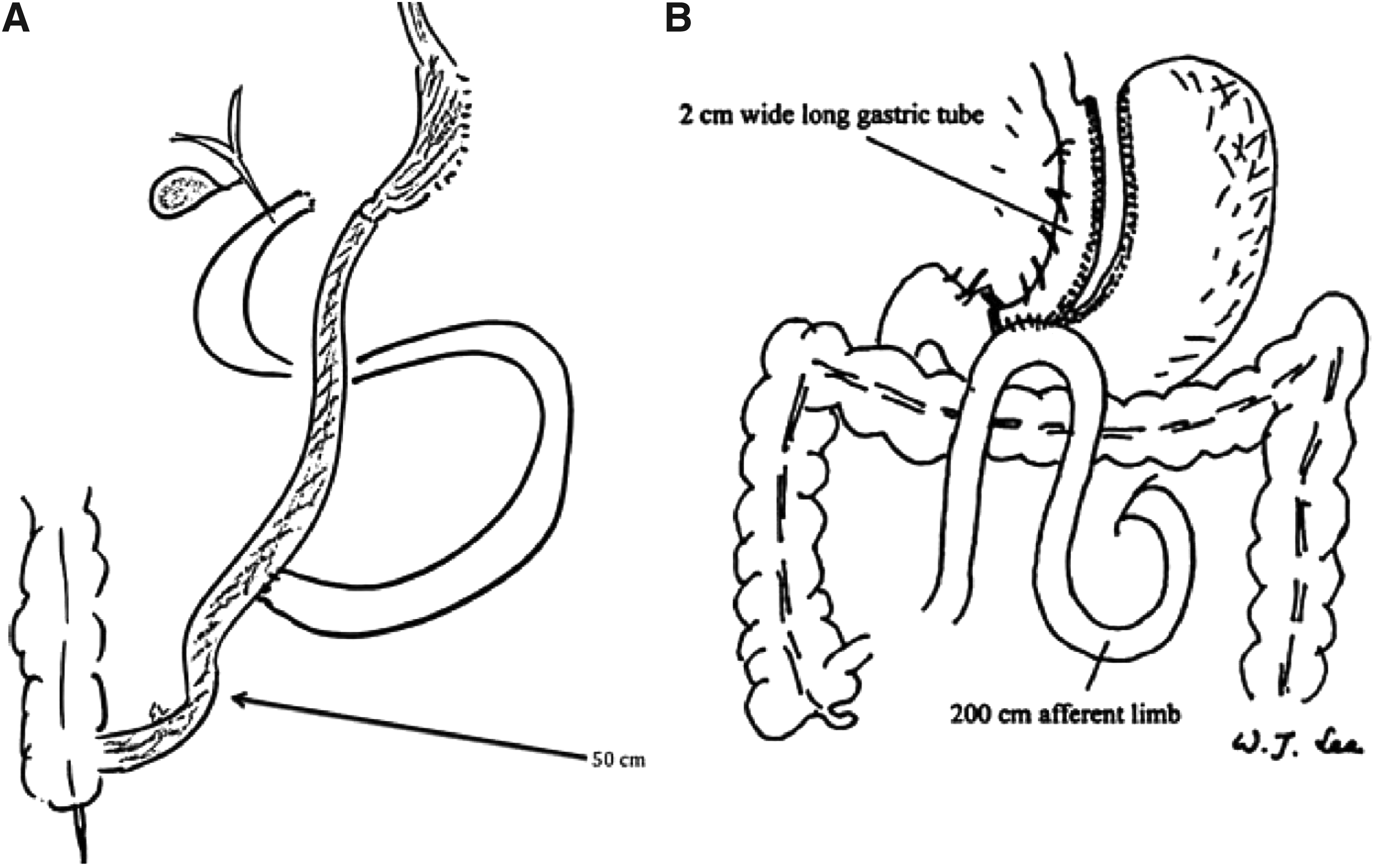
In brief, the SADI (Fig. 1) is a derivative of the biliopancreatic diversion-duodenal switch (BPD-DS) 1 that ameliorates the significant micronutrient deficiencies that can be associated with BPD-DS, with one less distal small-bowel anastomosis (Fig. 2).

SADI. An SG is performed. The first portion of the duodenum is transected. An omega-loop small bowel loop ∼250 cm from the ileocecal valve is brought up to the duodenum to form an end-to-side anastomosis. SADI, single anastomosis duodeno-ileostomy; SG, sleeve gastrectomy.
According to the 2018 IFSO position statement, average total body weight loss was as high as 38.9% at 12 months, with excess body weight loss ranging from 61.6% to 95% in the same time period. 2 The data are still being gathered with respect to amelioration of comorbidities, but there is no reason to believe that the SADI would be any less beneficial than other combined restrictive–malabsorptive procedures. The insulin sensitivity and glycemic benefits appear to be similar between the BPD-DS and the SADI, with both being better than Roux-en-Y gastric bypass (RYGBP) and the SG alone. 3
In one recent series of 82 patients, the two most common complications were nausea (6.1%) and dehydration (6.1%). 4 There are sporadic reports of early postoperative leaks at the duodeno-ileostomy.
A significant number of reports used the SADI as a remedy for failed SG or failed adjustable gastric banding with modest success. In fact, patients who had SADI after a failed index SG had less total body weight loss than those who had SADI as the index procedure, which is not an uncommon observation in patients who undergo SG conversion to RYGBP. 5
So in summary, what we know about the SADI are the following:
Largest reported individual series are <100 cases. Safely performed, virtually all laparoscopically. Amelioration of comorbidities is similar to those of BPD-DS, particularly for insulin and glucose homeostasis. An omega-loop duodeno-ileostomy that obviates a distal enteroenteral anastomosis. Duodeno-ileostomy requires ability to sew with laparoscopic or robotic instruments after duodenal transection at the junction of the first and second portions, similar to BPD-DS. SADI can be used as a revisional procedure for other failed weight-loss operations, in particular, failed SG. Barrier for transitioning from performing SADI to BPD-DS is minimal.
Issues to Consider Regarding SADI
The operation looks quite similar to the one-anastomosis gastric bypass (OAGB) or mini-gastric bypass (Fig. 2B). The difference is that the OAGB forms the anastomosis between the distal stomach (prepyloric) to the ileum, whereas the SADI forms the anastomosis postpyloric between the duodenum and the jejunum. 6 Which leak would the surgeon rather contend with should it ever to occur? Proponents of the SADI believes that it has less bile reflux than the OAGB, which is not much of an argument if the reported bile reflux in 925 patients is indeed 0.3%. 7
Micronutrient malabsorption is believed to be less drastic with the SADI when compared with BPD-DS, but this is merely an assumption because most nutritional deficiencies can take several years to fully manifest.
Reflux is not lessened with the SADI procedure. In fact, the OAGB may have less reflux given the potential reduction in intraluminal pressure from the gastrojejunostomy. 8
In the United States, most insurance payers currently do not consider the OAGB or the SADI a covered benefit. Even if patients pay from their own savings, it can create insurmountable economic and medical hardships should subsequent complications ever occur.
The SADI is a different operation than the BPD-DS. The BPD-DS has a long defunctionalized biliopancreatic limb that re-establishes continuity in the final 50 cm of ileum. In contrast, the SADI has ∼250 cm of distal small bowel for nutrient absorption; in this respect, the SADI is more similar to the OAGB. Both the SADI and BPD-DS do have the same high-stakes anastomosis at the duodeno-ileostomy that requires facile sewing skills to perform.
The SADI is not the “perfect” operation. Patients with SADI have been reversed or converted to RYGBP.
How Does SADI Compare with Other Procedures?
A comparison of weight-loss operations based on aggregate benefits (remission of comorbidities and weight loss) and risks (technical difficulty, complications, and adverse effects) will likely place SADI between RYGBP and BPD-DS (Fig. 3).
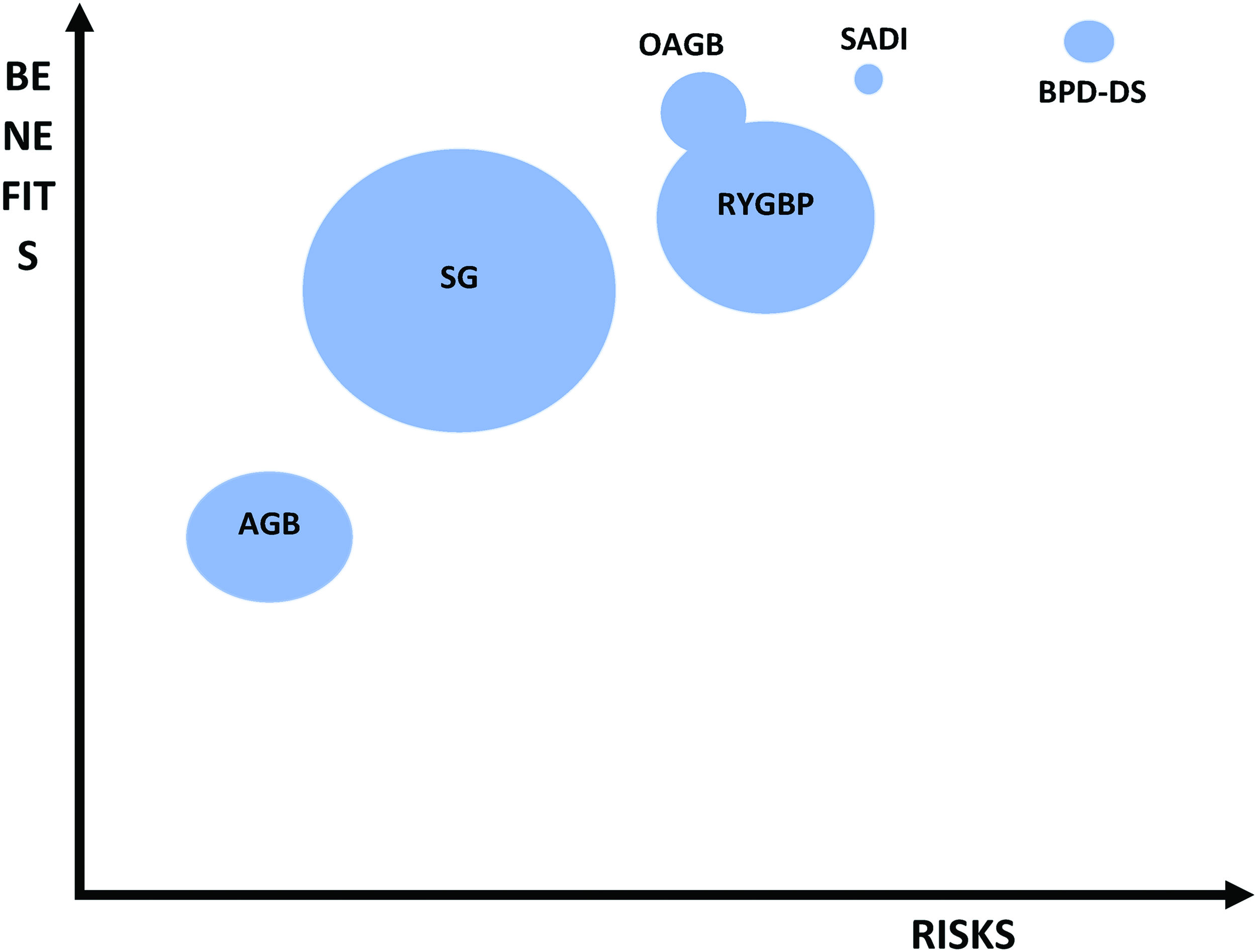
Framework for comparing different index weight-loss procedures based on benefits and risks. Balloon size is proportional to estimated frequency performed. AGB, adjustable gastric band. Color images are available online.