
Abstract
Background:
Internal herniation (IH) after gastric bypass surgery is a well-known complication. However, an IH through the foramen of Winslow has never been reported previously. Such herniations, most likely due to pre-existing conditions, combined with gastric bypass surgery and rapid weight loss demand adequate assessment. Although the incidence of “traditional” IHs has decreased since primary closure of these defects during initial bariatric surgery, rare types of IHs can still arise.
Methods and Results:
We report a case in whom a cecum volvulus due to malrotation herniated through the foramen of Winslow 14 months after gastric bypass surgery. In our case, radiological computed tomography examination indicated the possibility of a colic IH.
Conclusions:
We hypothesize that rapid weight loss and pre-existing conditions, such as a dolichocolon or malrotation, could predispose patients to these “unusual” types of IH. Although there is no other literature describing this phenomenon, we believe that “unusual” types of IH due to rapid weight loss are theoretically more common than previously thought and awareness is advised.
Introduction
The lifetime incidence for internal herniation (IH) after gastric bypass surgery is ∼2.5–4.5%.1,2 In the nonbariatric population, 1–8% of IHs is due to herniation through the foramen of Winslow (omental foramen) and 33% of these herniations involve the cecum or ascending colon.3,4 The combination of a herniating cecum through the foramen of Winslow and a Roux-en-Y gastric bypass could be considered an “unusual” herniation. This refers to the type of herniations not usually associated with bariatric surgery, such as those of the transverse mesocolon, Petersen's space, or mesenteric defect at the enteroenterostomy. These “unusual” types are a rare occurrence with no other cases reported in the literature.
Case Report
A 64-year-old female patient presented at our emergency department due to the acute onset of sharp abdominal pain in the right upper quadrant that radiated toward her back. She did not complain of nausea or vomiting and had recently passed stool. The patient's surgical history reported an uncomplicated antecolic laparoscopic Roux-en-Y gastric bypass 14 months earlier with an alimentary limb length of 75 cm and a biliopancreatic limb length of 150 cm. Before gastric bypass, the patient's weight was 98 kg with a body mass index of 40.1 kg/m2. In the 14 months after surgery, the patient had lost 34 kg (34.6% total weight loss).
At physical examination, the abdomen was extremely painful in the right upper quadrant. Blood results revealed a leukocytosis of 13.9 × 109/L, a C-reactive protein of <0.6 mg/L, and a lactate of 2.0 mM. The differential diagnosis consisted of IH, cholelithiasis, cholangitis, pancreatitis, (marginal) stomach ulcer, and perforation. IH of the small intestine was the most likely diagnosis and, therefore, a computed tomography (CT) scan with intravenous contrast fluid was performed to differentiate (Fig. 1). The CT scan, in which the report was not structured according to Ederveen et al., 5 showed signs of a suspected IH of the colon with distention of the cecum and collapsed transverse colon. The patient was then transferred to the operating room.
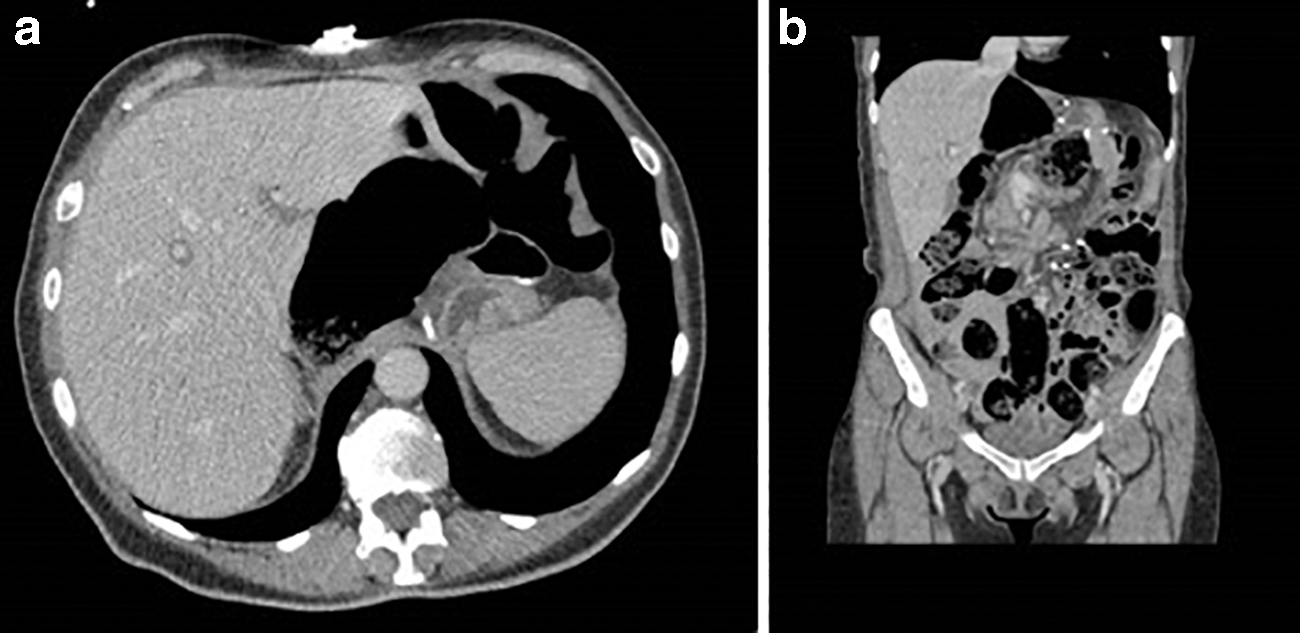
Abdominal computed tomography scan showing a distended large intestine and a suspected internal herniation through the foramen of Winslow.
During diagnostic laparoscopy, a midgut volvulus was seen and the cecum herniated through the foramen of Winslow (Fig. 2a–d). The gastric pouch and the surgical anastomoses from the previous surgery were all normal. Though attempted, laparoscopic relocation of the cecum was not possible and we converted to an upper midline laparotomy to successfully reposition the cecum. Although vital, the cecum was highly flexible throughout the abdominal region due to a malrotation and, therefore, an ileocecal resection was performed. The foramen of Winslow was approximated using nonabsorbable sutures. All bariatric mesenteric defects, which had been closed using staples during the original bariatric surgery, were still closed. The patient recovered well after surgery and was able to leave the hospital after 4 days without complications. Follow-up after 7 months showed a good recovery without any postoperative complaints or midterm complications.

Discussion
A cecal volvulus (the torsion of the cecum around its own mesentery, often resulting in obstruction and sometimes perforation and necrosis 6 ) that then herniates through the foramen of Winslow (omental foramen) is very rare. Predisposing factors include a common intestinal mesentery, failure of the right colon to retroperitonealize, a long small bowel mesentery, or a large foramen of Winslow. 4 This case is unique due to the combination of a cecal volvulus herniating through the foramen of Winslow after Roux-en-Y gastric bypass surgery, which caused rapid weight loss. Usual assessment and treatment would involve a CT scan with intravenous contrast fluid and if necessary an upper GI contrast study; this last diagnostic tool is less reliable in bariatric patients considering their altered anatomy. The rapid weight loss after bariatric surgery may have been the predisposing factor for such a herniation, leading to a sudden increase in space internally and potentially predisposing to the displacement of the highly flexible cecum. There is, however, no research to support this hypothesis.
Sanmugalingam et al. 7 reviewed three studies regarding IHs, either Petersen's space or enteroenteromesenteric defect, including one retrospective and two nonrandomized studies with a total of 6540 patients. In all patients an antecolic approach was used. Results showed significant reduction in IH when defects were closed, 14.4% versus 1.1%, (p = 0.0001)). The study of Aghajani et al., 8 which was not included in the previously mentioned review, prospectively evaluated 4013 patients who underwent laparoscopic Roux-en-Y gastric bypass for a 10-year period with a follow-up of 5.5 years. They found that primary closure of the mesenteric defects significantly reduced the incidence of IHs (primary closure: 60/2444 [2.5%] vs. mesenterial openings intact: 185/1570 [11.7%], relative risk 4.086 [confidence interval 95% 2.97–5.62]). In fact, there are numerous articles proving that the combination of an antecolic approach and the standard closure of the remaining mesenteric defects significantly reduces the incidence of postoperative IH.9–11
However, IHs still occur even when mesenteric defects are primarily closed due to rapid and massive weight loss. 12 The mesenteric defects in this patient were also primarily closed during the primary operation. We hypothesize that while primary standard closure of mesenteric defects decreases the chances of “traditional” IHs (between the Roux limb, the transverse mesocolon and the retroperitoneum [Petersen's space] or at the jejunojejunal anastomotic mesenteric defect), significant weight loss may increase susceptibility for the herniation through the foramen of Winslow or other potential “spaces” in the abdomen, such as paraduodenal or small bowel mesentery herniations. This susceptibility may be greater in patients with pre-existent, but at that point unknown, conditions such as a malrotation. There is, however, no literature to support this hypothesis.
We suggest that any type of IHs, “traditional” or those herniating through spaces less common after bariatric surgery (“unusual”), should be suspected in gastric bypass patients presenting with acute abdominal pain. Furthermore, if patients are known or suspected to have an underlying predisposing condition, such as a dolichocolon or malrotation, the treating surgeon may consider closing other herniation points prophylactically, such as the foramen of Winslow.
Conclusion
This case report describes a previously unpublished phenomenon in which a patient (14 months after gastric bypass surgery) presented with symptoms suggestive of an IH. During diagnostic laparoscopy, a cecum volvulus herniating through the foramen of Winslow was found and successfully treated; all usual mesenteric defects that primarily closed during previous surgery were still closed. Owing to a highly flexible cecum and malrotation, an ileocecal resection was performed. We hypothesize that this type of IH was due to underlying conditions, a malrotation, and was triggered by significant weight loss after Roux-en-Y surgery. Imaging by means of a CT scan plays a key role in the diagnosis of such a patient and is more difficult to interpret considering the patients altered anatomy. Combined awareness of the radiologist and bariatric surgeon is warranted here and structured radiology reporting in bariatric patients could improve accuracy of diagnostics. Similarly, IHs should be suspected in patients presenting with significant weight loss after bariatric surgery and acute abdominal pain, and surgeons could consider closing the foramen of Winslow in patients with predisposing conditions for IHs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.