
Abstract
Background:
This article has two aims: review current literature addressing sexual and gender minority (SGM) bariatric patients and describe a pilot study identifying sexual minority (SM) bariatric patients at an academic medical center.
Methods:
The literature review was conducted using keywords: lesbian, gay, bisexual, transgender, and bariatric. Our bariatric program's database from January 1, 2005 to September 10, 2015 was reviewed retrospectively. Chart review of partnered patients identified individuals with same-sex partners. Descriptive demographics and weight loss outcomes were obtained.
Results:
The literature review identified two articles about transgender bariatric patients and zero articles about SM bariatric patients. The database review yielded 5576 patients; 145 patients self-identified as partnered, including 16 (0.29%) with same-sex partners (11 women, 5 men). Mean age and preoperative weight were 40 years and 305 lbs (body mass index, BMI 48.5). Bariatric operations included 12 gastric bypass, 2 duodenal switch, 1 sleeve gastrectomy, and 1 gastric band. Twelve-month mean weight was 200 lbs (BMI 30, 50% excess weight loss) with 5 (31%) patients lost to follow-up.
Conclusions:
The published literature discussing SGM bariatric patients is limited. Within our case series, the SM bariatric patient population identified was 0.29%. Documentation of sexual orientation and gender identity within the bariatric screening process could better identify this population.
Introduction
Obesity is a complex metabolic disease and ongoing epidemic, as well as a risk factor for diabetes, cardiovascular disease, and reduced life expectancy, that currently affects 42% of adults in the United States. 1 The Sexual and Gender Minority (SGM) community continues to be an underserved health care group with regard to obesity care and bariatric surgery. This article reviews the literature involving SGM bariatric patients, as well as describes a case series designed to identify sexual minority (SM) bariatric patients at a large academic medical center.
The acronym “SGM” has begun to replace the familiar acronym “LGBT,” which stands for “lesbian, gay, bisexual, and transgender,” as the former better describes this diverse community and more clearly divides it into distinct groups: SM individuals (lesbian, gay, or bisexual individuals) and gender minority individuals (transgender or gender nonconforming individuals). In the past decade, several national health organizations have published recommendations for further research in SGM health to advance knowledge of this population.2,3
Historically, the SGM population has faced barriers to health care access, and discrimination in the health care setting. Some of the challenges SGM patients experience when interacting with the health care system include not disclosing identity owing to fear of discrimination and not being included on demographic data forms.3,4
The SGM community also experiences minority stress, defined as unique pressures such as stigma and prejudice faced by SGM individuals leading to an uncomfortable social environment and mental health problems. The model describes external stressors such as the “coming out” process and discrimination, as well as internal stressors such as identity-related self-esteem and internalized homophobia. 5 Collectively, minority stress can lead to heath concerns and impede access to care. In addition to the above psychosocial factors, SGM individuals also have higher rates of alcohol, tobacco, and drug use compared with their cisgender, heterosexual counterparts. 6
To increase awareness of this population, the two aims of this study include the following: to review current literature addressing SGM bariatric patients and to describe a pilot study identifying SM bariatric patients at an academic medical center.
Materials and Methods
Literature review
The literature review sought to identify all published studies addressing the topic of SGM bariatric patients. The following electronic databases were searched: PubMed, Web of Science, ScienceDirect, and Google Scholar; no language or date restriction was used while conducting this search. The search process included using the term bariatric with the following terms related to sexual and gender identity: lesbian, gay, bisexual, transgender, sexual minority, gender minority, LGBT, and SGM. All the included articles were subjected to analysis of their full text, and the eligible articles were identified.
Case series
Institutional review board approval was obtained (No: Pro00066540). A retrospective review of the Duke Center for Metabolic and Weight Loss Surgery database was performed from January 1, 2005 to September 10, 2015. Inclusion criteria consisted of adult patients with morbid obesity who completed bariatric surgery at our institution during this period. All patients underwent a standardized preoperative bariatric pathway including evaluation by a bariatric psychologist, cardiac and pulmonary risk stratification, an upper endoscopy, and monthly medically supervised weight loss sessions with nutritional goals focused on dietary habits needed to be successful postoperatively. Postoperative care consisted of scheduled bariatric clinic visits at 2 weeks, 3 months, 6 months, and 12 months.
Medical records of patients who self-identified as “partnered” during their presurgical psychology evaluation were reviewed to identify individuals with same-sex partners. This variable was used because direct inquiry about sexual orientation was not performed in the bariatric preoperative process. To determine the sex of patient's partners, two search methods were used. First, the psychology documentation was further reviewed to determine if the sex of the patient's partner was recorded in the psychology visit, if this was not documented, the patient's medical record was further reviewed to determine if partner sex was documented in it.
Additional variables, including patient age, sex, preoperative weight in pounds, preoperative body mass index (BMI), operation performed, 1-year postoperative weight in pounds, 1 year BMI, and 1 year percent excess weight loss, were recorded. Descriptive statistics were used to summarize patient characteristics.
Results
Literature review
The literature review identified two articles on the topic of gender minority bariatric patients and zero articles about SM bariatric patients. The two articles about gender minority bariatric patients included one case report and one review article, as summarized in Table 1.
Summary of Literature Review: Articles About Gender Minority Bariatric Patients
The 2018 case report by authors Clapp & Wynn, discussed a 41-year-old transgender woman whose successful bariatric surgery led to resolution of her body dissatisfaction and facilitated her successful transition process. 7 To our knowledge, this is the first published academic article documenting bariatric surgery for a transgender patient.
The 2019 article by authors Hecht et al. was a review article discussing psychosocial risk factors that may affect transgender patients within the following realms of bariatric care: presurgical assessment, surgical clearance, and postoperative period. 8 The authors highlight several ways in which the psychosocial needs of transgender bariatric surgery candidates are unique from cisgender individuals. Some of the unique issues facing transgender bariatric patients include the following: a higher prevalence of mood and anxiety disorders, increased rates of suicidal ideation, suicide attempts, and nonsuicidal self-injury (NSSI), increased amount of substance abuse, as well as higher levels of emotional and physical abuse, including physical and sexual assault. In addition, owing to distress caused by the discrepancy between physical gender characteristics and gender self-identification, transgender individuals may experience gender dysphoria, which can have a negative impact on their global mental health.
The article also discusses medical factors related to hormonal treatments used by transgender individuals. Although hormonal treatment in this population has been associated with a higher quality of life, use of hormonal medications can affect factors related to bariatric surgery. Feminizing hormones, such as estrogen, can lead to increased risks of venous thromboembolic disease, elevated liver enzymes, hypertriglyceridemia, gallstones, weight gain, and increased risk of cardiovascular disease in older patients. Masculinizing hormones, such as testosterone, carry risks of weight gain, sleep apnea, acne, balding, and polycythemia. Furthermore, the malabsorptive nature of certain bariatric procedures may impact postsurgical absorption of hormone medications.
In conclusion, the article encourages bariatric programs to be cognizant of the above differences between transgender and cisgender bariatric patients, and to augment their presurgical psychological assessment and postoperative process accordingly when caring for this population.
Case series
A total of 5576 bariatric patients (women 81%, men 19%), were identified within our program's bariatric database and 145 patients self-identified as partnered in their psychology preoperative evaluation, within this group there were 16 patients (0.29%) identified with same-sex partners, 42 patients with opposite-sex partners, and 87 patients who had no documentation of their partner's sex in their medical record (Fig. 1). Within the same-sex partnered cohort were 11 women and 5 men with mean age of 40 years and mean preoperative weight of 305 lbs (BMI 48.5). The operations performed included 12 laparoscopic gastric bypass, 2 robotic duodenal switch, 1 laparoscopic sleeve gastrectomy, and 1 laparoscopic gastric band. One-year postoperative mean weight was 200 lbs (BMI 30) and excess weight loss at 12 months was 50%. Five patients (31%) patients lost to follow-up at 1 year.

Flow chart of patients with same-sex partners identified in bariatric database.
Discussion
The two aims of this project were to review the literature discussing SGM bariatric patients and conduct a pilot study identifying SM bariatric patients at an academic medical center.
Within surgical literature, there is little published material surrounding SGM health. Kamen et al. have studied the SGM community within the context of cancer care and found that oncologic SGM populations are generally invisible, as national cancer registries do not collect these demographic data. Regarding comfort with disclosure of sexual identity, although surgeons are most likely to give patients their oncologic diagnosis, SGM patients are least likely to disclose their sexual identity to their surgeon. Other findings include that SGM cancer patients have significantly different support systems compared with heterosexual patients. SGM patients' support system consists largely of friends instead of immediate family members and involving the appropriate SGM support system positively impacted SGM health outcomes and satisfaction with health care providers. 9 Kamen et al. demonstrated that psychological disparities exist when comparing SGM cancer survivors with heterosexual cancer survivors. Relative to their heterosexual counterparts, gay men, bisexual men, and transgender cancer survivors experienced more depression and social concerns. 10 At present there is no standard screening for SGM bariatric patients, thus it is unknown if bariatric patients have similar challenges with disclosing their sexual identity to their surgeon and bariatric team, or if these patients also have nontraditional support systems.
As the obesity epidemic continues, identifying health care disparities that limit patient access to obesity care has become a pertinent issue. 11 Although obesity impacts many Americans regardless of age, race/ethnicity, socioeconomic status, and urban vs rural location, there is little published regarding the SGM bariatric population. Lesbian, gay, bisexual, and transgender individuals are all unique groups with different risks for obesity. Compared with their age-matched heterosexual peers, lesbian and bisexual women have higher rates of obesity.12–15 Although gay men have lower rates of obesity than heterosexual men, they have increased risks for eating disorders and body image issues. 16 The transgender community currently has the highest rates of obesity within the SGM population, with recent studies indicating that 30% of transgender Americans have obesity, with the highest prevalence occurring in transgender men (46%).8,13,17 Other food-related health issues occurring within this community include disordered eating and body image issues.18–20
The overlap of various social identities, termed intersectionality, can contribute to discrimination and exponentially increase minority stress for an individual. It is known that weight stigma has a different effect across racial groups. 21 Another element that may impact SGM patients with obesity is intersectionality between their SGM identity and their experience of obesity. At present, the relationship between weight stigma and SGM status is unknown.
Bariatric surgery is the most effective intervention for morbid obesity and outcomes are intricately intertwined with behavioral and psychological factors: successful bariatric surgery outcomes depend on lifelong changes in eating patterns and social support. Strong social support is associated with greater postoperative weight loss.22,23 Increasing knowledge about the unique needs of the SGM population may lead to greater SGM access to bariatric services, and improve the ability of bariatric programs to care for this group before, during, and after surgery. Most bariatric programs and the American Society for Metabolic and Bariatric Surgery's Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP) database do not collect sexual orientation or gender identity information; thus determining the degree of SGM access to bariatric surgery remains a challenge.
An additional limiting factor for SGM patient access to bariatric surgery is insurance status. Although some patients pay out of pocket for bariatric costs, the majority who undergo bariatric operations do so through a bariatric benefit in their insurance policy. Today in the United States 30% of lesbian, gay, and bisexual individuals and 20% of transgender individuals are uninsured, suggesting that SGM populations may have decreased access to bariatric surgery benefits. Furthermore, of the individuals that do seek health care services, 56% of lesbian, gay, bisexual, and 70% of transgender individuals have experienced discrimination in a health care setting, another system-based factor that may impede patient access to quality bariatric care. 24
The literature review yielded two published studies regarding transgender bariatric patients and zero studies about SM bariatric patients. The dearth of literature discussing SGM bariatric patients suggests that this population is under-identified and understudied, resulting in a gap in knowledge about how to provide the best obesity and bariatric care for this community. In addition, each SGM subgroup (lesbian, gay, bisexual, transgender, and nonbinary gendered individuals) has specific needs and risk factors that may benefit from individualized investigation and intervention. 24
Some of the unique issues surrounding transgender bariatric patients include a higher prevalence of mood and anxiety disorders, with lifetime rates approaching 46% and 38%, respectively, and elevated rates of suicidal ideation and self-harm behaviors. A study of transgender adults in California reported 34% of transgender adults experienced suicidal thoughts, and several studies cite 25–43% lifetime suicide rates for transgender adults.25,26 Transgender individuals also have a higher rate of NSSI with prevalence of 19–36.8%. Of note, transgender youth have even higher rates of self-harm behaviors that occur in 34% of transgender female youth and 56% of transgender male youth. Because of the high rates of the above mental health issues, the importance of adequate screening for these during the bariatric psychology evaluation cannot be underemphasized.
For transgender bariatric patients presurgical assessment should include screening for population-specific risk factors including minority stress, gender dysphoria, depression, anxiety, suicidal ideation and self-harm behaviors, substance abuse, emotional and physical abuse, and address the patient's use of hormonal therapy. Intersectionality with obesity and weight stigma should also be investigated. Surgical clearance, similar to all bariatric patients, should ensure that patients have adequate treatment for any of the above conditions, and adequate long-term support to ensure success after bariatric surgery. An important postoperative issue to consider within the transgender population is that the use of hormonal medications carries increased risk of venous thromboembolism, thus adequate education about the additional risks and appropriate postoperative prophylaxis is necessary.
The results of our case series, identifying only 16 (0.29%) SM bariatric patients of a group of 5576 patients, suggests that this population is significantly under-identified within our bariatric program, as the prevalence of SGM individuals in the United States is estimated to be ∼5.6% of the population, with a higher prevalence (7.2%) in adults younger than 30 years. 27 We believe this group was under-identified because of insufficient screening questions within our bariatric intake forms, thus patients were not given adequate opportunity to self-disclose their SGM status. After this study, our intake forms were modified to identify members of the SGM patients.
Multiple reports emphasize the importance of allowing patients to self-identify on intake forms to prevent invisibility. With regard to collecting information about patient sexual orientation and gender identity (SOGI), earlier studies indicate that 80% physicians were concerned that asking SOGI questions would offend patients; however, 97% of SGM patients were not offended by such questions and felt them to be a relevant part of their health care visit. 28 This demonstrates the need for further education to help health care providers feel comfortable and competent providing care to SGM patients. For bariatric practices to begin identifying SGM patients, the following items should be included in all intake forms: sexual orientation, gender identity, preferred pronoun, and preferred name. An example of SOGI intake questions is given in Figure 2.
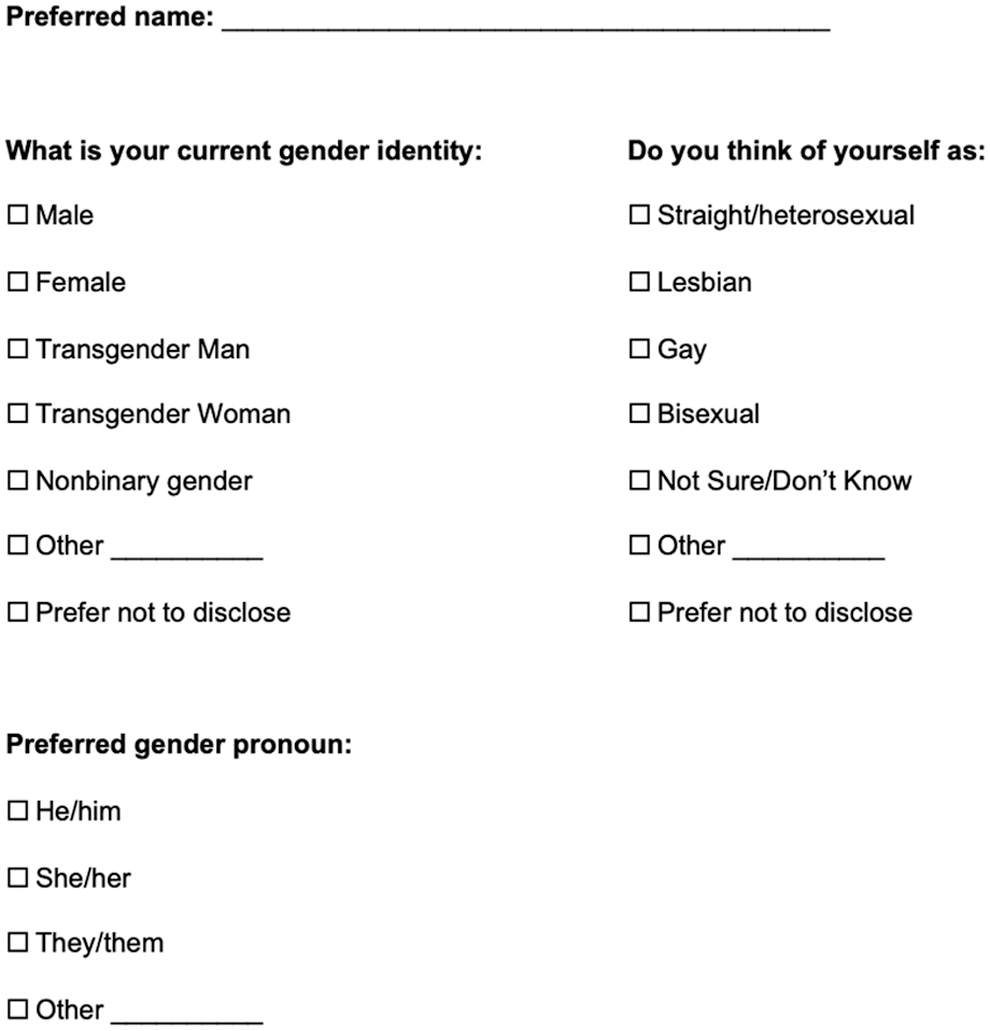
Example intake form for gathering SOGI information. SOGI, sexual orientation and gender identity.
Despite our sample being underpowered, there was an increase of male SM patients (31%) in the cohort, compared with the composite group (19%). Further investigation is warranted to determine if SM men seek bariatric surgery more frequently than cisgender, heterosexual men. In addition, patients in the SM cohort included 69% of patients with documented follow-up at 12 months, and 31% being lost to follow-up. The literature reports 12-month follow-up rates of 76%, after bariatric surgery range; although our SM group had a lower rate of follow-up, it is unclear if this was owing to their SM status versus other factors.29,30 However, the rate of lost to follow-up patients may be related, at least in part, to lack of positive rapport with the bariatric team because of absence of team knowledge/understanding of the patient's SM status. With regard to weight loss at 12 months, the SM group had 50% EWL, reflecting a good initial weight loss outcome.
Today SM patients are likely to be part of most bariatric practices in the United States. Areas that make this population unique include experience of minority stress, intersectionality with obesity-related issues, and the need for additional screening for mood disorders, anxiety, substance use, and maladaptive eating. Furthermore, SM patients differ from heterosexual patients in that they may have different support systems with friends serving as primary support rather than significant others or family members. It is important that the bariatric health care team be aware of these psychosocial differences to provide SM patients appropriate care. 19
With regard to minority stress, one factor that should be addressed during the bariatric psychological evaluation for SGM patients is the patient's degree of “outness” regarding their SOGI, as lack of disclosure can affect patient mood and well-being. Patients who have not fully disclosed their sexual orientation or gender identity may harbor more minority stress and have issues with their support system if their immediate family is not aware of their SOGI. For bariatric patients, social support is a key element for long-term success after weight loss surgery. 22 To foster strong bonds between bariatric team and patient, it is important for SGM patients to feel comfortable and safe disclosing SOGI to their bariatric team.
There are several limitations to this study. As a retrospective investigation, it relied on data that were not specifically designed to screen for SGM patients. Although chart review was performed to identify partnered patients with same sex partners, there was no way to identify nonpartnered SM patients or gender minorities because our program intake forms did not include collection of SOGI information. Another shortcoming pertains to the small sample size of SM patients identified; this number was underpowered to perform any substantial statistical analysis. An additional challenge with describing the SGM community is that it consists of multiple smaller groups, each with individual psychosocial and health care needs. Each of the SGM subgroups: lesbian, gay, bisexual, and transgender have different issues with regard to physical health, mental health, and health care access. Thus, the most effective research involving this population should identify each group in significant numbers to better understand the unique health care needs of each subpopulation.
Conclusions
The SGM population is a growing minority demographic that faces numerous health care disparities and is currently under-identified within bariatric programs despite lesbian, bisexual, and transgender subgroups carrying increased risk of obesity, and all subgroups carrying increased risks of maladaptive eating habits. We encourage bariatric programs to give patients an opportunity to self-identify their SOGI during the intake process, with hopes that this will lead to improved relationships between SGM patients and their bariatric health care team. Further studies are needed to examine the individual SGM subgroups to better understand the unique needs each population may have regarding obesity care and bariatric surgery, as well as to better inform prevention efforts.
Footnotes
Author Disclosure Statement
D.P. is a consultant for Novo Nordisk, a speaker for Medtronic and recipient of a Medtronic research grant, a speaker for Gore and recipient of a Gore education grant, a speaker for Teleflex and recipient of a Teleflex research grant, a speaker for Intuitive Surgical and recipient of an Intuitive Surgical research grant, an advisory board member of Levita Magnetics, and an owner of Changzhou Panda Medical Co. Ltd.
N.S. is a consultant for C-SATS and CMR Surgical, recipient of a Digbi Health research grant, and founder of Endolumik, Inc.,
S.S.: No competing financial interests exist.
K.F.: No competing financial interests exist.
Funding Information
No funding was received for this study.