
Abstract
Background:
In recent years, bariatric surgery has proven to be a leading medical intervention to help patients meet their weight loss goals. While the surgery is an effective tool patients can use in addition to lifestyle modifications, there have been inconsistent outcomes in the effect of bariatric surgery on psychopathology and quality of life. Additionally, few studies have explored patient experience with regard to body image for patients undergoing bariatric surgery.
Methods:
To evaluate this phenomenon, we conducted semistructured focus groups with both male and female pre- and postsurgical bariatric patients focusing on body image concerns.
Results:
Concepts and themes related to body image that presented in the presurgical focus groups were grouped into five main categories: surgical motivations and expectations, negative cognition and affect, physical and daily life challenges, social behavior, and social comparisons. Elicitations from postoperative groups comprised three categories: social behavior, mind/body relationships, and health and physical changes.
Conclusions:
The differences between the ways in which pre- and postsurgical patients spoke about their experiences in their bodies speaks directly to the importance of the complex and multidimensional constructs presented, as well as to the potential need for nuanced conversations to prepare patients for surgery and ongoing support postsurgically.
Introduction
Evidence concerning the benefits of bariatric surgery continues to grow as well as the associations between bariatric surgery, weight loss, and a reduction in obesity-related physical comorbidities. 1 However, to date, the research regarding psychological outcomes following bariatric surgery has been mixed, with some studies showing dramatic improvements in quality of life and mood disorders, and some suggesting that these improvements dissipate over time.2,3 Evidence also suggests that risk of poorer psychological adjustment following bariatric surgery can be partially attributed to body image dissatisfaction, along with persistently negative perceptions and experiences of one's own body, regardless of weight loss. 4 While there is a growing interest in research addressing body image within bariatric populations, a paucity of studies directly addresses the patient experience as it relates to body image throughout the course of the pre- and postoperative periods.
Background
Body image is a construct referring to a person's perceptions, cognitions, and emotions in relation to one's own body. 5 Research regarding body image refers to the concept of embodiment, which in the phenomenological view, suggests that perceptions and identity first originate within the body. 6 Therefore, one's “lived experience” within the body can be interpreted in relation to the world through language and movement, and in relation to objects, space, and time. 7 This approach also suggests that perceptions of body image are rooted in meaningful cultural and social contexts. 8 Body image is therefore associated with self-concept and persons' convictions regarding their abilities and qualities in comparison with others. Negative appraisals of body image have been associated with lower self-esteem, depression, and binge eating, 9 as well as poorer quality of life in bariatric patients. 10 Recent neuroscience research implicates the amygdala as playing a role in the consolidation of allocentric (body as object in the physical world) sensory input to long-term memory, whereby negative cognitions and emotions associated with obesity become stored by the amygdala, resurfacing despite weight loss. 11
Lower body weight has often been associated with physical attractiveness12,13 leading obese women in particular to report greater body dissatisfaction when compared with average-weight women.14,15 Women's reasons for choosing bariatric surgery are more appearance driven when compared with men, who typically report that deteriorating health and mobility prompted their decision to undergo weight loss surgery.16,17 Nevertheless, in both women and men, the perception of one's body as less attractive, and less functional is a cognitive process. These negative somatic representations may become entrenched and slow to change, affecting cognitive processing of subsequent experiences related to the body. For example, postsurgery, patients must make the psychological transition of integrating previous roles and self-identities as “obese” persons with successful weight reduction, and the “new” smaller person in the mirror. Theorists have referred to this transition of psychological orientation as “I-obese,” versus “I-ex-obese” after rapid weight loss. Patients with longstanding identities as “I-obese” may have difficulty navigating this transition. Consequently, despite successful weight loss, female postoperative bariatric patients have endorsed an “I-obese” identity 18–30 months after surgery.11,18
Much of the existing body image research within bariatric populations approaches the construct and assessment of body image from the perspective of normal weight or eating disorder populations, using self-report measures that have not been validated for use with bariatric populations.10,19 Due to the multifaceted nature of body image, this approach may neglect or fail to identify the characteristics of body image dissatisfaction unique to bariatric surgery patients. Prior studies have highlighted the complexity of this issue as postoperative patients have reported “ambivalence” as they balance the achievement of weight loss with the resulting excess skin, persistent negative experiences of their bodies, and disappointment regarding the gap between expectations and postsurgical realities. 20
Qualitative research can provide meaningful and valuable insight into the patient experience of bariatric surgery, by exploring the depth and complexities inherent within that experience. 21 Qualitative study can also highlight the variability of the patient's lived experience over the duration of patient's participation in the preoperative and postoperative surgical/weight management programs.22,23 Nevertheless, much of the current research is limited to a narrow exploration of body image following bariatric surgery, often focusing solely on the postoperative period. 21
Given the potential impact that body image may have on patient outcome, well-being, and satisfaction after bariatric surgery, it is important to gain a more comprehensive understanding of the contextualized accounts of patient experiences of body image pre- and postsurgery. Our study presents a qualitative phenomenological approach to exploring patients' lived experience of their weight, body habitus, perceptions of functionality, weight stigma, and expectations versus realities of surgical weight loss.
Methods and Materials
Patients were actively recruited from the Surgical Weight Loss Clinic of one academic medical center from January 2019 to December 2019. Patients were required to be 18 years of age or older with a preoperative body mass index (BMI) of 40 or greater to be recruited for participation. Patients with a preoperative BMI of 35 or greater were considered if they were also diagnosed with comorbid conditions, such as sleep apnea or type 2 diabetes mellitus. Postoperative BMI varied. Both men and women were included in the study. Those who were actively completing presurgical assessments and attending presurgical educational sessions as well as postoperative patients (2 months to 12 years postsurgery) were invited to participate. Before participation, patients were presented with a summary explanation of research and given the option to participate or opt out. Consent to participate in the focus group was considered implied if the patient took part in research activities.
Focus groups were stratified based on surgical status. Multiple 60-min focus groups were conducted at the Surgical Weight Loss Clinic. Groups were led by trained study team members (E.S. and A.W.) utilizing a phenomenological approach that explored both pre- and postoperative patients' perceptions of body image. Group interviews were semistructured with prompting questions to encourage discussion among participants. Goals of the presurgical group included the elicitation of responses from participants regarding topics such as weight bias, body image concerns, functional impairment, and the perception of social support. Participants were encouraged to share their narratives and identify barriers faced as a result of their weight. Participants were also encouraged to disclose current or previous expectations for postsurgical change. Postsurgical participants were asked an additional final question aimed toward encouragement of deeper additional reflection on participants' surgical journeys. A copy of the interview guide is provided in Supplementary Methods.
Each focus group was digitally audiorecorded and then transcribed verbatim by a study team member for analysis. Transcripts were independently and manually coded by two different study team members utilizing both inductive and deductive coding. Codes from these two independent coders were then merged to create a code book and reviewed for agreement. A separate codebook was created for the presurgical groups and postsurgical groups. Codes were then reviewed until consensus was established. Dissenting opinions were discussed until consensus was reached between all study team members and the study Principal Investigator. Initial coding was conducted through the use of margin notes. Final coding was performed using NVivo 12 Plus. NVivo 12 plus was used to build concept maps based on content analysis of the focus groups. This study was reviewed and approved by the Institutional Review Board (IRB).
Results
Patient characteristics
A total of 14 patients participated in the presurgical focus groups. One of these patients was undergoing a revision surgery and was excluded from analysis. Of these 13, 2 were male and 11 were female. The postsurgical group consisted of 11 patients with 2 males and 9 females. Overall, 24 patients were included in the analysis. Patient characteristics are detailed in Table 1. Relevant thematic quotations are provided in Supplementary Table S1.
Participant Characteristics
BMI, body mass index; SD, standard deviation.
Preoperative content analysis
The presurgical focus groups focused primarily on body image concerns, internalized weight bias, and use of social media as a form of support. Concepts and themes related to body image that presented in these interviews were grouped into five main categories: surgical motivations and expectations, negative cognition and affect, physical and daily life challenges, social behavior, and social comparisons. Each of these primary categories were assigned secondary codes along with some tertiary codes (Fig. 1). A concept map of the preoperative focus group themes is presented in Supplementary Figure S1.
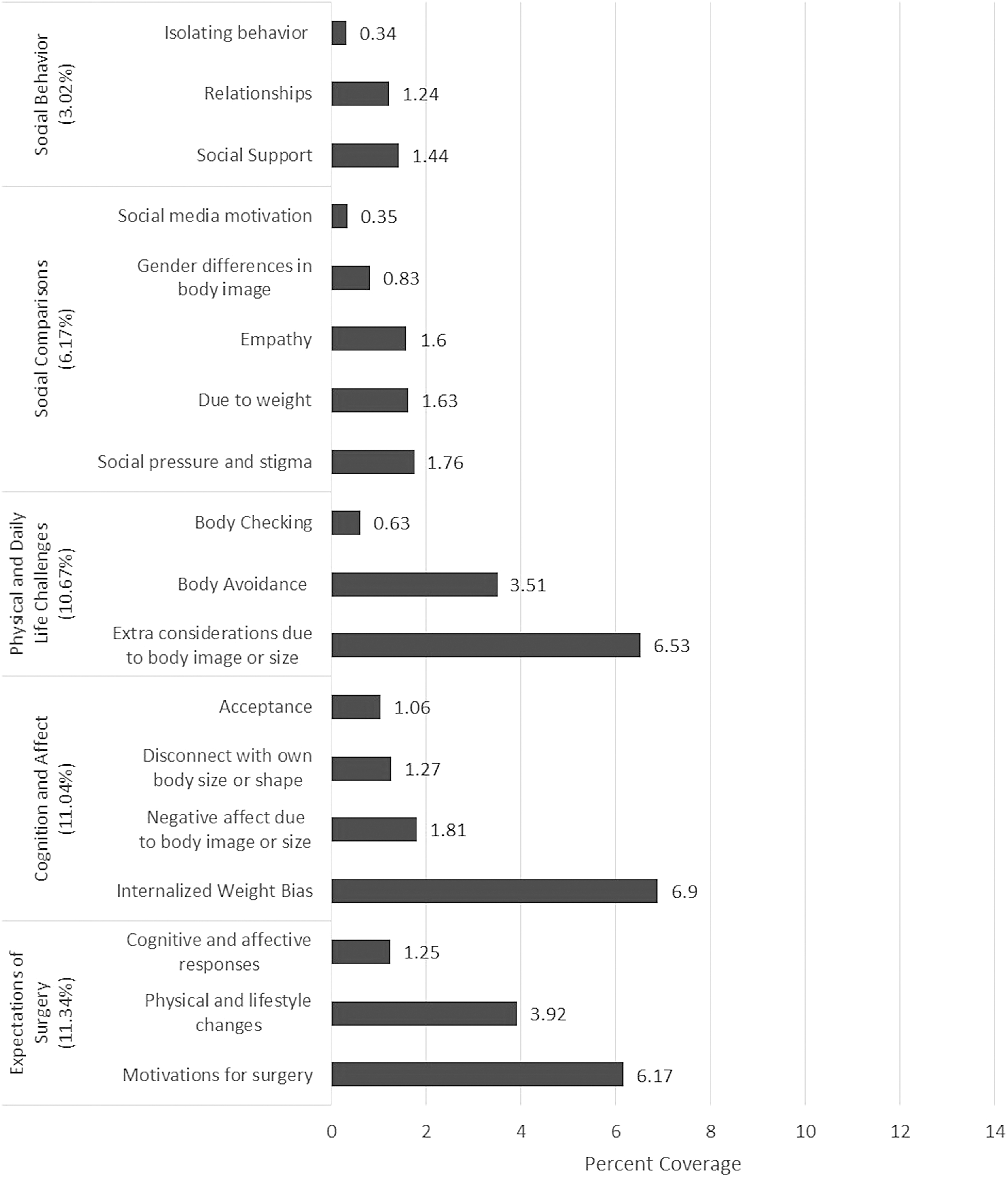
Presurgical concept elicitations. Figure depicts the total percentage coverage of qualitative coding within the presurgical focus group transcripts.
Surgical motivations and expectations
Patients were asked to reflect on how they anticipated surgery would change their perceptions regarding body image. In all focus groups patients endorsed hopeful expectations relating to physical changes in their bodies, which was expected to impact lifestyles and behaviors postsurgery. In additional to physical changes, patients anticipated cognitive and affective changes to a lesser degree and expressed fears and apprehension toward the upcoming procedure. Patients also heavily endorsed that health and physical concerns were a primary motivating factor in seeking bariatric surgery. Other motivating factors included the desire to improve self-perceptions (both negative and positive) and fears for the future should no change occur. Barriers to change, while occasionally cited, typically related to logistical concerns (e.g., finances, transportation, familial obligations, and work obligations) as well as motivational barriers.
Negative cognition and affect
With regard to concerns relating to body image, patients heavily endorsed negative affect in relation to their body image or size as well as instances of internalized weight bias. Patients also expressed difficulty mentally accepting their physical bodies, including denial and disbelief regarding current weight suggesting disconnect between the individual and his or her shape or size. Instances of “mind-reading” also manifested in all focus groups. “Mind-reading” often reflected the individual's personal fears regarding perceptions by others. Patients were also very aware of stereotypes regarding obesity and overweight that fuels social stigmas related to weight. Despite these conflicted and negative feelings, notions of acceptance (e.g., self-confidence, normalizing cognition, self-care, and self-compassion) surfaced during the discussions as well.
Physical and daily life challenges
Instances of body avoidance presented in nearly all focus groups while conversely, participants acknowledged body checking (e.g., use of mirrors and scales) to a lesser degree. All participants strongly reflected upon the extra consideration and challenges they faced as a result of their body shape or size, such as accommodations for travel, eating in public due to fear of scrutiny and subsequent shame, along with physical size, and participating in activities with peers and families.
Social behavior
Phenomenon relating to relationships was less prevalent theme; however, patients did endorse challenges regarding relationships especially with regard to engaging in socially isolating behaviors and the negative impact of weight on sexual performance as well as desire for intimate relationships. The use of social support and positive personal relationships for coping was endorsed within a number of focus groups. Self-acceptance fell into this category as well with a number of patients emphasizing accepting and normalizing cognitions and engaging in self-care.
Social comparisons
The notion of social comparisons presented both in relation to the use of social media as well as everyday social environments. Comparisons often resulted due to weight differences and social pressures. To a lesser degree, patients identified sources of positive social influences that served as motivation for change as well as empathy for others struggling with weight. The notion of gendered differences in body image presented in some of the conversations and suggested that women were more affected by weight stigma and societal pressures when compared to men.
Postoperative content analysis
Postoperatively, patients exhibited similar concerns as well as additional challenges. Improvements in health and physical functioning were addressed along with patients' prior expectations for change preoperatively, versus postoperative reality. Changes in cognitive and affective processes from pre- to postsurgery were explored. Elicitations from these postoperative groups comprised three categories: social relationships, body image, and health and physical changes. Themes within these primary categories were further transformed into secondary codes along with some tertiary and quaternary codes (Fig. 2). A concept map of the postoperative focus group themes is presented in Supplementary Figure S2.
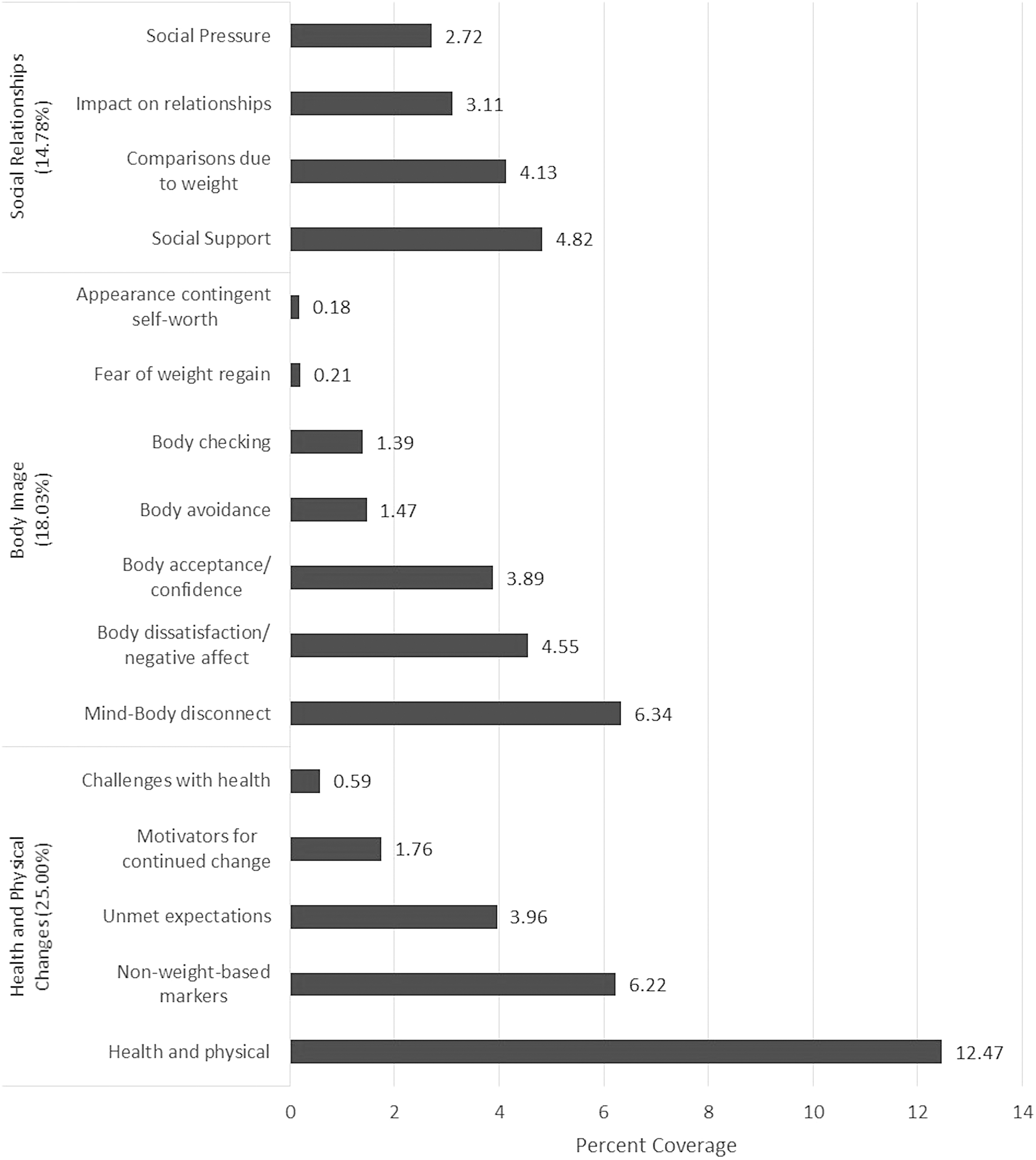
Postsurgical concept elicitations. Figure depicts the total percentage coverage of qualitative coding within the postsurgical focus group transcripts.
Social relationships
Patients endorsed substantive changes in their social interactions as well as their awareness of disparities between pre- and postsurgical social regard by others. Similar to presurgical patients, postsurgical patients acknowledged comparisons to others due to weight or weight loss, increase in social pressure as a result of weight loss and decreased weight stigma, and change within close relationships. Specifically, patients identified both improvement in personal relationships and lack of support from their close friends and family, particularly with regard to eating, exercise, and appreciation of the patient's postsurgical adjustment trajectory. As a result, some close relationships were severed due to the perception of negative influences on the behavioral, social, and attitudinal changes individuals were attempting. Postoperative patients expressed ambivalence, anger, and sadness as they compared noticeable increases in positive social attention with preoperative experiences of weight bias and social isolation.
Body image
Cognitive and affective phenomenon were highly prevalent in the postoperative patients. Patients cited barriers to change, instances of body avoidance, body checking and dissatisfaction, along with improved body confidence when compared with the preoperative patients. Patients endorsed increased awareness of positive and negative cognitive and affective changes along with desire for additional mental health support for navigating these changes. Patients continued to report disconnect between their physical shape and internal perceptions of themselves indicating a struggle with accepting their new bodies. A subset of patients related an increase in the practice of self-compassion as a method for integrating previous expectations with actual outcomes, including weight loss, regain, and plateaus; body functioning, and excess skin.
Health and physical changes
Awareness of health and physical changes varied dependent upon presurgical expectations and aspirations, and the actuality of weight loss and postsurgical life. When prompted, many participants expressed that their expectations for surgery did not completely align with the reality after, and many expressed frustrations as a result of not meeting personal goals. Changes specifically due to weight loss presented as concerns for excess or loose skin that developed as patients continued to lose weight, and with length of time postsurgery. Some patients experienced periodic health challenges both as a result of surgery and due to comorbidities. Patients also heavily endorsed behavioral changes that occurred both in relation to their lifestyles (e.g., exercise) and their relationships with food and substances, particularly alcohol. References to nonweight-based markers of weight loss (e.g., looser clothes) were also common in the conversations and were cited as motivators for continuing weight loss, particularly as patients experienced weight loss plateaus.
Discussion
The current research adds to the growing body of literature examining body image in patients presenting for bariatric surgery. The totality of the research thus far clearly marks this as a complex and multidimensional construct for which it is crucial to understand variations among populations. 24 The differences between the ways in which pre- and postsurgical patients spoke about their experiences in their bodies speak directly to the importance of this, as well as to the potential need for nuanced conversations to prepare patients for surgery and ongoing support postsurgically.
The most-often cited theme for the presurgical group related to physical and daily life challenges, which underscores the fact that motivations for pursuing weight loss surgery are multifaceted, including a combination of desire for improved health, role function, and appearance. They strongly endorsed high expectations for the ways in which the surgery would change their lives, including improved overall appearance and confidence, better health, and enhanced functioning. Striking were the consistent and often unprompted discussions of the negative stereotypes attached to those who are medically classified as obese, as well as the seamless transition between speaking of others' weight bias and the internalization of this bias. Furthermore, a prominent theme included the ways in which either potential weight stigmatization experiences or internalized bias prevented them from engaging in desired ways in their lives.
The postsurgical groups typically spoke of surgery as an overall positive experience, with nuanced complexities that speak to the differences between patient expectations and their lived reality. They described improvements in health, role function, and reduced barriers to daily life activities, such as seeing a grandchild's sporting games, with health and physical changes as the most frequent theme discussed. These nonweight-based markers of improved health and role functioning appeared to further bolster body acceptance and confidence. Despite this, there was also acknowledgement that, often, not all goals had been met, and there was typically ongoing dissatisfaction regarding loose skin. This was described both as an esthetic dissatisfaction and as a functional and health limitation given the pain that the skin can cause. Participants discussed generally increased social engagement, with noteworthy negative affect resulting from the realization that strangers and others in their lives often treated them more positively following weight loss. This invalidation of their prior bodies and reinforcement of societal weight bias appeared to add complexity to acceptance of their current bodies. Furthermore, they spoke of a mind/body disconnect, such that they often failed to reconcile cognitions, affect, and behavior with their weight loss until substantial periods of time had lapsed. The ways in which this interacts with behaviors typically thought of as maladaptive, such as body avoidance and body checking, raise compelling questions for continued study of body image in this population.
The diversity of topics raised by participants suggests that revised quantitative measures of body image may be needed to characterize this construct in patients undergoing bariatric surgery, and that multiple measures capturing different components of body image should be included in future research. Participants in the current study spoke of topics that represent self-perceptions and attitudes about one's body, as well as subjective evaluations of their bodies and the ways in which this is influenced by larger social structures and more immediate interactions with the proximal environment, thereby mapping onto multiple dimensions of the body image construct. 25 To understand the role of body image for these patients, focused research findings should be balanced by those that capture the full scope of the construct. Our results suggest that this will need to include research capturing body functionality, health, the impact of bodies on relationships, weight stigmatization experiences, and internalized weight bias, as well as the change process for each of these postsurgically. Limitations of generalizability mean that clinicians and researchers should not take conceptualizations of body image founded on college student samples or samples of patients with eating disorders to hold true for patients with bariatric surgery; it may be that distinct facets of body image are more impactful toward quality of life and overall well-being for patients undergoing this surgery. Understanding which components of body image are most meaningful for this population will have implications for both presurgical preparation and postsurgical support and intervention.
Consistent with previous literature, our postsurgical participants spoke of a mind/body lag, such that their cognitive, behavioral, and affective experiences in their body were based on the aforementioned “I-obese” rather than the “I-ex-obese” that might be expected based on weight loss alone.11,18,20 Additionally, striking was the consistent and marked difficulty participants described in receiving and interpreting comments from others. These two themes appeared to intersect in multiple participants' descriptions, such that another person would make a seemingly positive statement about the participant's weight loss and their immediate internal reaction was to note that they have not yet achieved their goals and consequently do not want or deserve praise or positive commentary. Perhaps such reactions are grounded in the “I-obese” identity without integration of the “I-ex-obese” perspective.
Relatedly, both pre- and postsurgical participants further discussed frequent appearance-related social comparison, body avoidance, and body checking. For example, frequent mirror checking, or conversely, mirror avoidance was described. The extent to which this behavior, which is viewed both in theoretical and research findings as maladaptive in the eating disorder literature,26,27 reinforces the “I-obese” or “I-ex-obese” mindset at varying points pre- and postsurgically is not yet understood. It seems theoretically plausible that these behaviors could reduce the mind/body lag through reminding oneself of actual body size, and in some instances appear to be similar to mirror exposure that is hypothesized in the eating disorder literature to reduce body image distress.
28
For instance, in one postoperative group, a participant described previous mirror avoidance and her current efforts to change that behavior:
Now I'm working on looking at myself more, not to be judgmental, but just in the moment looking at myself.. . yeah, it's hard, before you're like picking apart every single thing. It's like learning to chip away at that behavior. (Postoperative patient)
Yet, it could also function to increase negative affect and preoccupation with body dissatisfaction, as it appeared to do for one participant who tracked his weight loss to the decimal point “religiously” (Postoperative patient). Lyons et al. similarly note that the impact these behaviors have could be both positive and negative. 20 A more fine-grained analysis that examines frequency, prompting events, function, and consequences of these behaviors at different time points along the surgical process would be valuable. Overall, the description from the current participants suggests that the mind/body lag could result in an integration of both an “I-ex-obese” identity with an “I-obese” identity, rather than the loss of the latter in favor of the former. Given patients often strong sentiment that surgical weight loss would fully transform their lives, understanding the integration of these identities could enhance clinicians' ability to prepare patients for the realities of postsurgical life.
As previous research has suggested, weight stigmatization experiences and internalized weight bias factored prominently in current participants' experiences in their bodies both pre- and postsurgically.13,18,20 Frequent stigmatization experiences and avoidance of environments in which such an experience might occur significantly impacted presurgical participants' views of their own bodies and engagement in social situations. Postsurgically, decreased stigmatization was not uniformly positive and presurgical stigmatizing experiences appeared to continue to factor into self-perceptions and relationships. As one participant described:
It's amazing, when I was fat, people wouldn't talk to me. But now I'm losing weight, the people who wouldn't talk to me, now they're talking to me. Now wait a second I'm the same person, only I'm not fat. (Postoperative patient)
Losing weight appeared to solidify their understanding of the ways in which the world previously treated them differently, and most often cruelly, due to their weight, causing a range of negative affect and behavior. In some instances, this appeared to prompt continued social isolation, as participants did not want to invite those into their lives who previously did not notice them due to their weight. The fact that these experiences and weight bias continued to impact daily living and body image postsurgically marks it for continued research and attempts to mitigate its ill effects. Furthermore, body size is one of the few types of stigmatized identities that is subject to change over the course of a lifetime, thereby potentially providing valuable insight into the role of such stigma on a host of meaningful outcomes, such as well-being, emotional experiences, relationships, and identity.
To the best of our knowledge, this is the first study to qualitatively describe the subjective experience of participants' relationships with food postsurgically. Participants spoke both about the physical relationship with food, such as learning which foods would now cause them to feel ill, as well as the emotional relationship with food. In some cases, they appeared to view these shifts as positive, such as decreased emotional eating. In others, they spoke about it with a visceral sense of loss, particularly when combined with unmet weight goals:
I was not prepared to give up a lot of things I liked to eat. That was very hard, on top of you can't eat this and you're not a size two. I feel like I'm losing over here. (Postoperative patient)
Statements such as these call for future research and program development initiatives for how best to prepare patients for this change.
As noted, the number and depth of the themes established in the current research underscores the need for future research to examine body image as a multidimensional construct in bariatric patients. 24 To ask the question “does body image improve postsurgically?” would be to miss the nuance and depth of these patients' experiences in their bodies, as well as the fluctuations that appear to occur postsurgically. Future clinical care would benefit from longitudinal research that captures the full spectrum of how body image changes before and after surgery, as time frame for capturing data appears to impact the picture seen.13,20,29,30 In our own postsurgical sample, a participant less than 1 year out from surgery noted quite different experiences from those several years postsurgery. For example, in one postsurgical group, several members were less than 2 years out from surgery and one member was 8 years postsurgery. While those with less time elapsed since surgery discussed difficulty with unmet expectations, the ebbs and flows of weight loss, and continued body dissatisfaction, the participant who was 9 years postsurgery described a “journey” perspective and more apparent integration between the “I-obese” and “I-ex-obese” perspective. Here again, focused research questions must be balanced with data that can inform the full picture of the ways in which different components of body image change over the course of living life postsurgically.
Limitations
This study presents with some limitations. Given the qualitative nature of the study, focus groups were subject to a number of variable factors, including the number of patients in each group, the type of surgical procedure, the amount of weight lost, the personalities of those in the groups, and the strategies of the interviewer. The focus groups' questions were scripted; however, the two lead interviewers' reflection statements, while intentionally brief, may have varied. Additionally, groups differed in terms of personal experiences as well as their individual desire and ability to express their feelings. Postoperative patients were recruited at various stages in their postoperative care. As a result, patients were at different postsurgical adjustment time frames with variability in the development and practice of different coping methods in response to body image concerns.
Additional variability between the coders could factor into results as well. Each focus group was coded by two coders. All groups were coded by two team members, (M.B.) as well as a second study team member (E.S. or A.W.). Kappa statistics were not calculated as the ultimate goal of coding was to reach consensus on the concepts that manifested in the focus groups.
Conclusions
Overall, this research highlights the importance that body image concerns play in the psychosocial health changes that occur in patients undergoing bariatric surgery. The close intersection of these phenomena with internalized weight bias results in the manifestation of a number of other behaviors and psychosocial thought processes that have the potential to impact surgical outcomes if left unaddressed. Future studies are needed to identify the long-term health outcomes that are impacted by pervasive body image concerns as well as interventions that can mitigate these feelings and improve such outcomes.
Ethics Statement
This study was reviewed and approved by Penn State IRB. As this study included only minimal risk, participants were presented with a summary explanation of research and consent was deemed implied if the patient took part in the research activities.
Footnotes
Acknowledgments
The authors would like to thank Emily Stefano, PhD and Betsy Aumiller, DEd for their work and contributions to this project.
Author Disclosure Statement
The authors have no relevant conflicts of interest.
Funding Information
Data collection for this research was supported by the Brad Hollinger Eating Disorders Research Endowment at Penn State Health/Penn State College of Medicine Research Grant 2019–2020.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.