
Abstract
Introduction:
Laparoscopic one-anastomosis gastric bypass (OAGB) is a bariatric surgery that can be used to treat obesity. It is considered a new procedure in the Gulf Region. The purpose of this study is to assess the initial experience with OAGB and its safety and efficacy as a primary bariatric surgery.
Methods:
We performed a retrospective before and after study on a consecutive group of patients who underwent bariatric surgery in the period between January 2015 and December 2018 in two hospitals. Data on weight loss, resolution of comorbidities, as well as postoperative morbidity and mortality were recorded from patient's files.
Results:
A total of 40 patients underwent OAGB as a primary surgery. The mean follow-up time was 31 ± 12.3 months. The average weight and body mass index before OAGB was 116.1 ± 25.3 kg and 43.7 ± 7.7 kg/m2, respectively. The minimum weight they have reached is 74.6 ± 19.7 kg. Percent total weight loss (%TWL) at 1, 3, 6, and 12 months postoperatively was found to be 10.6, 17.9, 27.9, and 34.1%, respectively. %TWL on the last day of follow-up was 34.3%. Patients with comorbid conditions such as hypertension, diabetes, asthma, obstructive sleep apnea, or menstrual irregularities reported either complete resolution or improvement of their condition. No marginal ulcers, anastomotic stenosis, or leaks occurred; however, one patient had bile reflux.
Conclusion:
OAGB is safe and efficacious in decreasing the excess body weight and eliminating most of obesity-related comorbidities when performed as a primary surgery.
Introduction
The epidemic of obesity presents a major challenge to chronic disease prevention around the world. 1 Obesity is associated with an increased risk of type 2 diabetes mellitus, hypertension, coronary heart disease, stroke, osteoarthritis, sleep apnea, and certain cancers. 2 Conservative measures to treat obesity might be ineffective in some patients, necessitating bariatric surgery. Indications for bariatric surgery were identified by the National Institutes of Health (NIH) Consensus Development Panel in 1991 3 and were later revised by the American Bariatric Society in 2004. 4 These indications include having a body mass index (BMI) of ≥40 kg/m2 with no comorbidities or BMI 35.0 to 39.9 kg/m2 with at least one serious comorbidity such as type 2 diabetes, hypertension, dyslipidemia, and obstructive sleep apnea, among others or a BMI of 30.0 to 34.9 kg/m2 with uncontrollable type 2 diabetes or metabolic syndrome. Laparoscopic one-anastomosis gastric bypass (OAGB) can be performed as a primary or revision bariatric surgery to treat such patients. It consists of a long narrow gastric pouch created by dividing the stomach, and a loop gastrojejunostomy at the lower end of the pouch reducing body weight by both restrictive and malabsorptive factors.5–8 OAGB is a simple and safe procedure and can be easily revised, converted, or reversed.7,9,10 The purpose of this study is to assess our initial experience with the safety and efficacy of OAGB as a primary surgery to decrease the excess body weight and eliminating obesity-related comorbidities.
Methods
Study design
A retrospective before and after study was carried out in a public and a private hospital in Kuwait on consecutive patients who underwent OAGB as a primary bariatric surgery between January 2015 and January 2018. The inclusion criteria for this study were patients aged 18–60 years, with no previous bariatric surgery. Exclusion criteria included patients who had a previous bariatric surgery or had undergone any intervention after the OAGB. Patients were not directly involved in this study, but as their information was included, ethical approval was granted from the ministry of health (ethical approval number 2018/726) for access to patient information data base system. This study is registered in research registry (researchregistry5298), and the work has been reported in line with the STROCSS criteria. 11
Preoperative preparation and operative technique
All patients were seen preoperatively by a dietician specialized in postbariatric surgery diet follow-up with knowledge in eating disorders assessment and management. All patients underwent a radiological barium swallow, gastric endoscopy, and routine laboratory tests, including nutritional, vitamins, liver, endocrine, and coagulation profile. All surgeries were done by two experienced surgeons under the same way to reduce variation. All patients had OAGB laparoscopically with four ports and surgeon standing on the right side of the patient with the assistant on the left. Surgery started by creating a long gastric pouch using an EndoGIA 45 mm stapler ∼1.5 cm to the left of the lesser curvature to transect the gastric sleeve transversely to create the gastric pouch. An antecolic end to side gastrojejunal anastomosis is then performed with a 30 mm EndoGIA stapler to a jejunal loop 150 cm distal to the ligament of Trietz. The gastroenterostomy is then closed with continuous suture. A 36 French bougie (Ethicon) is then advanced to the efferent jejunal loop to inject blue dye to check for anastomotic leak. The omentum was not divided.
Postoperative care
All the patients received care under a standard pathway. Patients were encouraged to ambulate right after surgery and oral feeding was allowed to start on postoperative day one after the performance of a gastrografin swallow leak test. Patients were discharged home on the third postoperative day. Patients were followed up by a surgeon and a dietician, once a month for the first 2 postoperative months and every 3 months thereafter. Patients were advised to take a daily multivitamin tablet as a supplement; iron supplement, vitamin B12, calcium, and vitamin D supplement. For the first 6 months only, patients were prescribed a proton pump inhibitor and a bile salt in the form of ursodiaxicolic acid. Routine laboratory tests, including nutritional, vitamins, liver, endocrine, and coagulation profile, were performed once every 3 months in the first year, once every 6 months in the second year, and once yearly thereafter.
Ethical considerations, data collection, and statistical analysis
Ethical approval for the conduction of this study was granted. A list of all the patients who underwent OAGB since January of 2015 onward was taken from the operation theater surgical cases database. Patients were screened back in time and those who have had OAGB as a primary bariatric procedure were selected for this study. This gave a total of 40 patients. Comorbidity status was measured as: hypertension is blood pressure >120/80 requiring medication for control, and diabetes is fasting blood sugar of more than 6.9, hemoglobin A1c (HBA1C) of more than 6.5, or 2 h oral glucose tolerance test plasma glucose of more than 11 requiring oral hypoglycemic agents or insulin for control. Asthma as a reversible obstructive pulmonary disease requires prophylactic therapy. Gastroesophageal reflux disease (GERD) is an endoscopic diagnosis of esophagitis, and patient is symptomatic on regular proton pump inhibitor (PPI). Obstructive sleep apnea (OSA) was diagnosed using polysomnographic evidence requiring the patient to use continuous positive airway pressure (CPAP) at night. Remission was measured as follows: for hypertension and diabetes, regulation of blood pressure or blood sugar level to normal while stopping all medications; for asthma, dropping the need of taking daily preventative therapy and having no exacerbations in the last 6 months; for GERD, dropping the need of taking PPIs and asymptomatic; for OSA, dropping the need of using night CPAP. Improvement was measured as follows: for hypertension and diabetes, decreasing the amount of oral hypertensive or hypoglycemic drugs by at least 1 drug AND having control of the disease; for Asthma, a drop in at least one severity class; for GERD, a drop in the requirement of PPI for symptomatic relief. All information was derived from patients' medical file records.
Statistical analysis was conducted using IBM SPSS Version 25. The difference in means test was used for comparison of mean weight and BMI before and after OAGB and for normally distributed laboratory investigations. Man–Whitney U test was used for testing laboratory investigation results that had a skewed distribution. p < 0.05 was considered significant.
Results
Our sample size was 40 consisting of 80% females, and the mean age was 40 ± 10.4 (20–60). The mean follow-up time was 31 ± 12.3 months. Four of our patients had previous insertion of intragastric balloon for weight loss, but none had a bariatric procedure. The weight loss profile of our patients is presented in Table 1 and Figures 1–3. The mean weight and BMI before OAGB were 116.1 ± 25.3 kg (82–180 kg) and 43.7 ± 7.7 kg/m2 (32.9–70.3 kg/m2), respectively. The minimum mean weight and BMI they have reached after OAGB is 77.6 ± 19.7 kg (50–134 kg) and 28.3 ± 7.7 kg/m2 (18.9–52.3 kg/m2), respectively. Percent total weight loss (%TWL) at 1, 3, 6, and 12 months postoperatively was found to be 10.6, 17.9, 27.9, and 34.1%, respectively. %TWL on the last day of follow-up was 34.3%. Percent excess weight loss (%EWL) at 1, 3, 6, and 12 months postoperatively was found to be 28.0, 47.6, 73.2, and 88.9%, respectively. %EWL on the last day of follow-up was 84.3%. At the last day of follow-up, post-OAGB, only one patient had an %EWL of less than 25 (2.5%), while 5 (12.5%) had an %EWL between 25–50%, and 34 (85%) had an %EWL of more than 50.
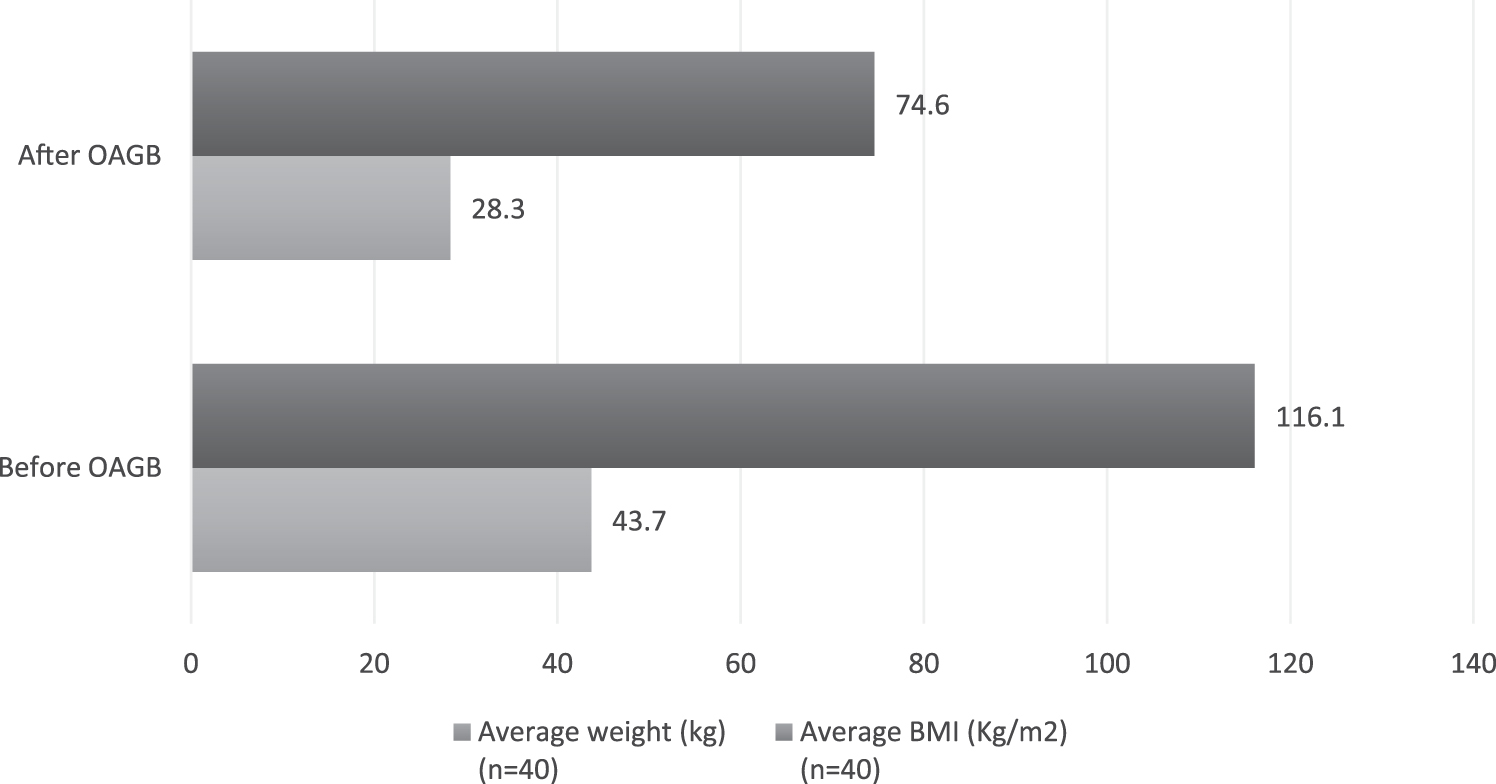
Weight & BMI comparison before and after OAGB. BMI, body mass index; OAGB, one-anastomosis gastric bypass.
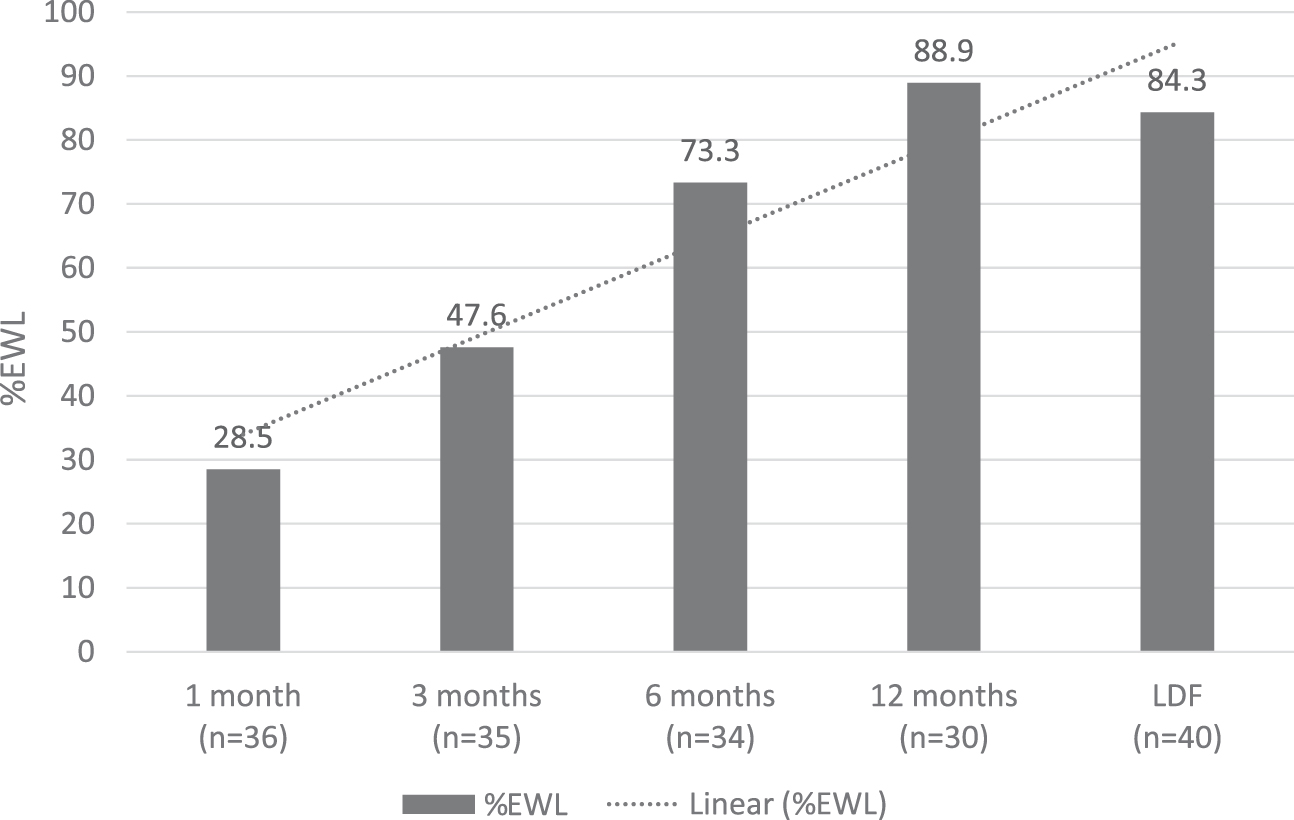
%EWL in relationship to time after OAGB. %EWL, percent excess weight loss.
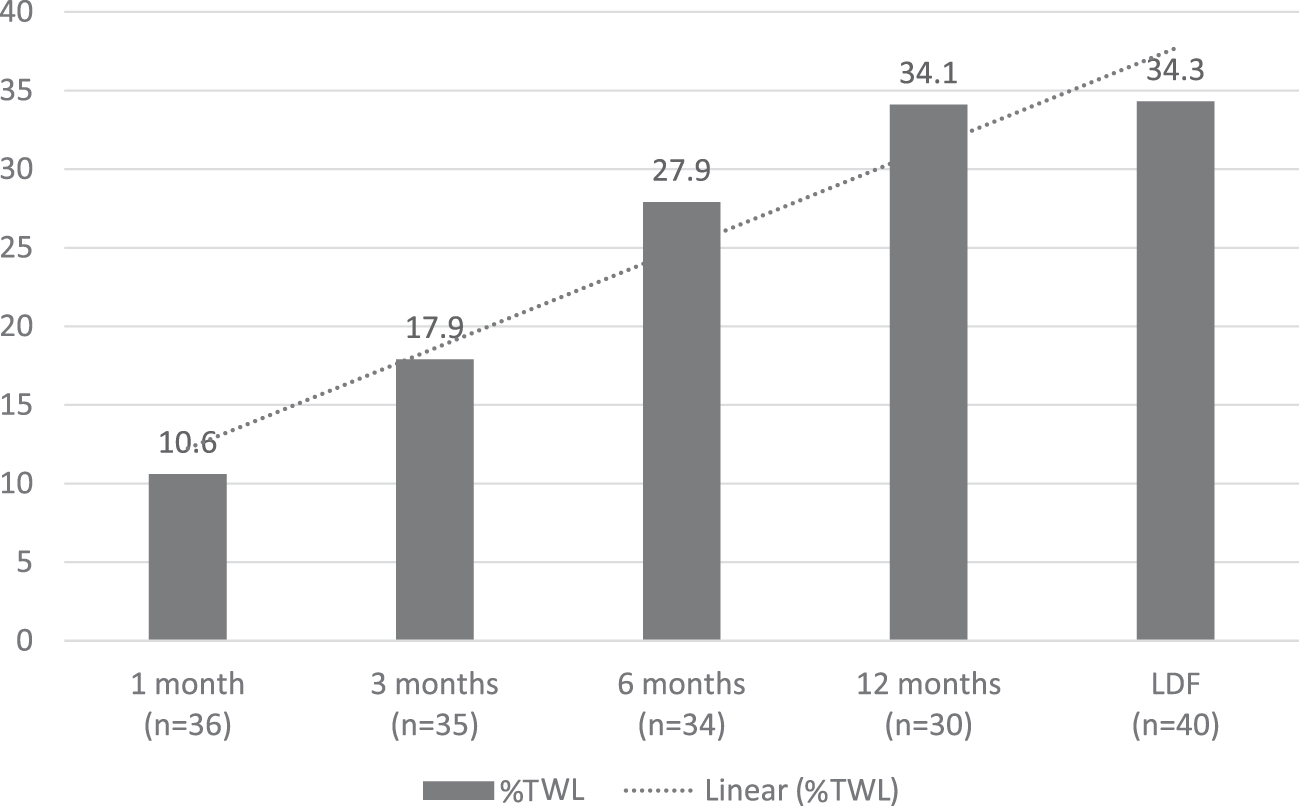
%TWL in relationship to time after OAGB. %TWL, percent total weight loss.
Weight Loss Profile
p-Value tested for difference in means of weight and BMI before and after OAGB. It was significant at p < 0.000.
BMI, body mass index; %EWL, percent excess weight loss; LDF, last day of follow-up; OAGB, one-anastomosis gastric bypass; SD, standard deviation; %TWL, percent total weight loss.
We have investigated blood laboratory results of 23 of our patients before and after OAGB. This included hemoglobin, mean corpuscular volume, iron, albumin, total cholesterol, triglycerides (TG), high-density lipoproteins, low-density lipoproteins, lactate dehydrogenase, calcium, glucose, vitamin D, and vitamin B12. Among these tests, only TG showed a significant difference before and after the OAGB dropping from 1.33 to 0.88 (p = 0.007) as seen in Table 2.
Laboratory Investigation Results of 23 Patients Before and After 1 Year of One-Anastomosis Gastric Bypass
Normally distributed variables mean < 1/3SD—difference in means t-test.
Skewed variable mean > 1/3SD—difference in medians Man–Whitney U test.
HDL, high-density lipoproteins; LDH, lactate dehydrogenase; MCV, mean corpuscular volume; TG, triglycerides.
All hypertensive and/or diabetic patients reported either complete resolution or improvement of their condition as presented in Table 2. All seven patients who had OSA in our study completely had full control on their condition after OAGB and have dropped the need of using CPAP at night. Seven patients were suffering from menstrual irregularities of >35 days interval, all of them successfully had their menstrual cycle normalized by the last day of follow-up (Table 3).
Comorbid Condition Status After One-Anastomosis Gastric Bypass
Remission was measured as follows: for hypertension and diabetes, regulation of blood pressure or blood sugar level to normal while stopping all medications; for asthma, dropping the need of taking daily preventative therapy and having no exacerbations in the last 6 months; for OSA, dropping the need of using night CPAP.
Improved measurement as follows: for hypertension and diabetes, decreasing the amount of oral hypertensive or hypoglycemic drugs by at least one drug AND having control of the disease; for Asthma, a drop in at least one severity class.
Seven patients had PCO diagnosed and had irregular periods of >35 interval, all of which reported regulation of their period at LDF.
CPAP, continuous positive airway pressure; OSA, obstructive sleep apnea.
When it comes to complications, our study reports no incidence of marginal ulcers, leaks, and anastomosis stenosis; however, bile reflux occurred with one patient (2.5%) as presented in Table 4.
Complications After One-Anastomosis Gastric Bypass
Discussion
In this study, we report our initial experience with OAGB as a primary procedure in Kuwait, which is part of the Gulf Region. We report excellent results in terms of weight loss and resolution of comorbidities with no mortality and only one patient with bile reflux. OAGB is a promising bariatric procedure given its technical simplicity and ease of revision. However, when compared to Roux-en-Y gastric bypass (RYGB) or other bariatric procedures, OAGB is less preferred to date although studies continue to show its safety and efficacy. For example, Rheinwalt et al. have reported comparable %TWL (36% vs. 34%) and resolution of comorbidities at 3 years of follow-up between OAGB and RYGB with the former having significantly shorter operation time (80 vs. 103 minutes), dumping syndrome (3.6% vs. 6.6%), and anastomotic stenosis (1.9% vs. 14.7%) when compared to RYGB. GERD incidence, however, was higher with OAGB when compared to RYGB (3.6% vs. 0.7%). 12 If GERD develops after primary OAGB, Olmi et al. have reported their experience of complete resolution of signs and symptoms after performing a Braun anastomosis to treat this condition. 13
Lee et al. experience with OAGB reports that it is more effective than RYGB in terms of weight loss with a lower BMI (27.7 vs. 29.2) at 5 years and higher %EWL (72.9 vs. 60.1) when compared to RYGB. Not only that, but also they have seen less major complications with OAGB (1.8% vs. 3.2%). Both procedures had a similar revision rate and resolution of comorbidities.
Surgeons continue to fear OAGB due to complications such as bile reflux, marginal ulcers, and malnutrition, however, the incidence of such complications are repeatedly reported in the literature to be quiet low.14,15 Hussain et al., for example, have reported that complications arising after OAGB are uncommon affecting 2.3% of patients, and if they occur, they can be successfully managed by revision of RYGB or Braun anastomosis. Those complications included severe diarrhea (0.4%), bile reflux (0.3%), bleeding (0.3%), liver decompensation (0.2%), gastrojejunal stenosis (0.2%), perforated ulcer, excess weight loss, and protein malnutrition affecting 0.1% each. 16 These numbers are very low and occur in the minority of patients undergoing OAGB. In this report, we had one patient who developed bile reflux postoperative. This patient was complaining of heart burn and gastroscopy revealed pouchitis with bile present, he was managed conservatively with Carafate 1 gram, quater in die and PPI.
A comprehensive review by Mahawar et al. concluded that although biliary reflux might complicate OAGB resulting in histologic gastritis, it does not necessarily become symptomatic. The review found no increased risk of gastric or esophageal cancer after OAGB. It is worth noting that Helicobacter pylori plays a critical role in the development of gastritis and gastric cancer and its presence is a prerequisite, so eradication is essential in all patients before OAGB. The review commented on marginal ulcer as a complication to be uncommon and the high occurrence reported by some studies is due to inaccuracy, bias, or poor follow-up. 14 The reported marginal ulcer rate by three big well-conducted studies ranged from 0.6% to 4.0%, which is similar to that seen with RYGB.10,17,18
From our experience, OAGB was very effective in reducing weight with a %TWL of 34.3% at 12 months that have persisted to the last day of follow-up (31 months). The average patient's weight and BMI dropped significantly more than 40 kg and 15 BMI grades, respectively. We also report it to be very effective in eliminating and improving comorbidities such as hypertension, diabetes, asthma, OSA, and menstrual irregularities. When it comes to complications, our study found no major morbidity or mortality following OAGB as a primary surgery, however, one case of bile reflux occurred.
Limitations of this study include the small sample size of 40 patients, it is worth mentioning, however, that this is the first report from a Gulf Cooperation Council (GCC) country of its experience with primary OAGB.
Conclusions
This study significantly reports on the safety and efficacy of the OAGB to decrease the excess body weight. Our results also indicate that OAGB is a successful surgical procedure to eliminate most of the obesity-related comorbidities.
Footnotes
Authors' Contributions
R.E. designed the study, analyzed the data, and writing, R.A. and A.A. collected data, H.A. collected the data and proof reading. M.H.J. conceptualized, designed the study, writing, and proof reading. All authors have provided approval of the final version to be published.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.