
Abstract
Background:
Single-incision trans-umbilical laparoscopic sleeve gastrectomy (SITU-LSG) is associated with better aesthetic outcomes. However, no studies have evaluated clinical outcomes associated with SITU-LSG in Chinese adolescents.
Methods:
We evaluated adolescents who had undergone SITU-LSG from May 2016 to June 2019. Clinical outcomes were assessed at postoperative 1, 6, and 12 months.
Results:
This study enrolled 13 patients (7 females, 6 males) with respective age, weight, height, and body mass index (BMI) values of 16.46 ± 1.98 years, 123.35 ± 22.64 kg, 171 ± 9.06 cm, and 41.73 ± 5.03 kg/m2. Operative duration, intraoperative blood loss, duration of postoperative hospitalization, and hospitalization costs were, respectively, 90 (range: 70–130) min, 20 (range: 5–50) mL, 3 (range: 2–5) days, and 58161.62 ± 6595.56 yuan. There were no postoperative mortalities or major complications. At 12 months, BMI for these patients had decreased to 28.20 ± 2.27 kg/m2 (p < 0.01), whereas the percentage of excess weight loss was 67.97% (range: 56.00–110.70%), and height had risen to 172.62 ± 8.66 cm (p < 0.05). SF-36 scores were significantly improved in all eight indices (p < 0.01).
Conclusion:
These data confirm that SITU-LSG is safe and effective for obese Chinese adolescents, significantly improving postoperative quality of life and aesthetic appearance.
Introduction
Laparoscopic sleeve gastrectomy (LSG) currently represents the most commonly performed bariatric surgery, 1 and advances in the fields of precision medicine and accelerated rehabilitation have been applied to expedite and improve bariatric surgery patient outcomes.2–5 Single-incision trans-umbilical LSG (SITU-LSG) was first conducted in 2008 by Saber, who found this protocol to be associated with satisfactory aesthetic outcomes. 6 Since that initial report, many studies have proven SITU-LSG to be a feasible approach to the treatment of adult patients, with safety and efficacy comparable with that of traditional multiport LSG.7–12
However, reports regarding SITU-LSG procedures performed in adolescents are still lacking. Although LSG has been reported to improve the quality of life of treated adolescents,13–15 no studies to date have assessed the dynamic changes in quality of life for these patients after SITU-LSG. In addition, few studies have assessed clinical outcomes of LSG in Chinese adolescents. To overcome these knowledge limitations, this study was designed to specifically assess SITU-LSG clinical outcomes in Chinese adolescents.
Materials and Methods
Herein we retrospectively assessed 13 adolescent patients (7 female, 6 male) who had undergone SITU-LSG at Beijing Shijitan Hospital between May 2016 and June 2019. These patients were defined as adolescents based upon World Health Organization criteria, as all were 10–19 years old. 16 In addition, all patients eligible for inclusion in this study met the surgical indications in the Chinese guidelines for bariatric surgery. 17 Additional study inclusion criteria were as follows: (1) body mass index (BMI) <50 kg/m2, (2) no history of abdominal surgery, (3) no history of mental illness, (4) no diseases affecting the skin in the abdominal region, and (5) patients were willing to consent to undergo this procedure after being made aware of the risks of reduced port LSG.
Before SITU-LSG treatment, all patients had failed to achieve satisfactory outcomes through conservative treatments including Chinese medicine, exercise, and decreasing food intake for at least 6 months. A multidisciplinary team composed of a gastroenterologist, an endocrinologist, a psychiatrist, a nutritionist, and a bariatric surgeon assessed SITU-LSG surgical indications for each patient. Patient demographics, comorbidities, preoperative status, operative status, and postoperative status were retrospectively analyzed for this study. All 13 enrolled patients underwent treatment at a single center, with operations being performed by three experienced surgeons who had conducted ≥800 laparoscopic bariatric procedures.
All patients underwent abdominal and gynecological ultrasound scans and polysomnography preoperatively and at each follow-up time point. Fatty liver and polycystic ovarian syndrome (PCOS) were diagnosed by abdominal and gynecological ultrasound scans, respectively, and were considered to be cured if subsequent examinations for these comorbidities were negative after a positive diagnosis. Obstructive sleep apnea syndrome (OSARS) was diagnosed through polysomnography, and subsequent negative polysomnographic findings were considered to indicate that OSARS had been cured.
All operations were performed as per CONSORT 2010 guidelines, and the institutional review board (IRB) of Beijing Shijitan Hospital had approved this study. All patients and their parents provided informed consent after being made aware of the potential risks associated with the SITU-LSG procedure.
Operative techniques
Three surgeons performed standardized SITU-LSG procedures for all 13 patients in this study. In brief, pneumoperitoneum (15 mmHg) was first created by inserting a Veress needle into the navel. Patients then adopted a reverse Trendelenburg and left-side up position with their legs separated to form an “A” shape. The surgeon then stood between the patients' legs, while the first assistant who was responsible for holding the laparoscope stood to the right of this surgeon. The second assistant was positioned on the patient's right side.
A 2 cm arc-shaped incision was made at the plica medially to the belly button. A disposable incision protective sleeve was placed through this incision, and the disposable incision retainer was connected with the incision protective sleeve (single-port device; Fig. 1). Hole “A” was used for visualization, whereas ultrasound knife and 60-mm endoscopic staplers (Endo-GIA Tri-Staplers) were inserted through hole “B,” and rotatable pliers (Fig. 2) and other pliers were inserted through holes “B” and “C.” The first Kirschner needle (K-needle, length: 26 cm, diameter: 1.5 mm, Fig. 3) was used to puncture the abdominal cavity under the tip of the xiphoid process and was subsequently used to retract the left outer lobe of the liver.18,19

Single-port device. Color images are available online.

Rotatable plier. Color images are available online.

Kirschner needle. Color images are available online.
The K-needle was then inserted into the right diaphragmatic crus through the visceral surface of the liver to a depth of 5–10 mm. To minimize the risk of accidental liver or chest cavity puncture and consequent hemorrhage or pneumothorax, this procedure was conducted under laparoscopic visualization. When effective visualization was not achieved using the first K-needle, a second needle was inserted into the left or right diaphragmatic crus. The left outer lobe of the liver was then raised to fully expose the gastric fundus and cardia (Fig. 4).
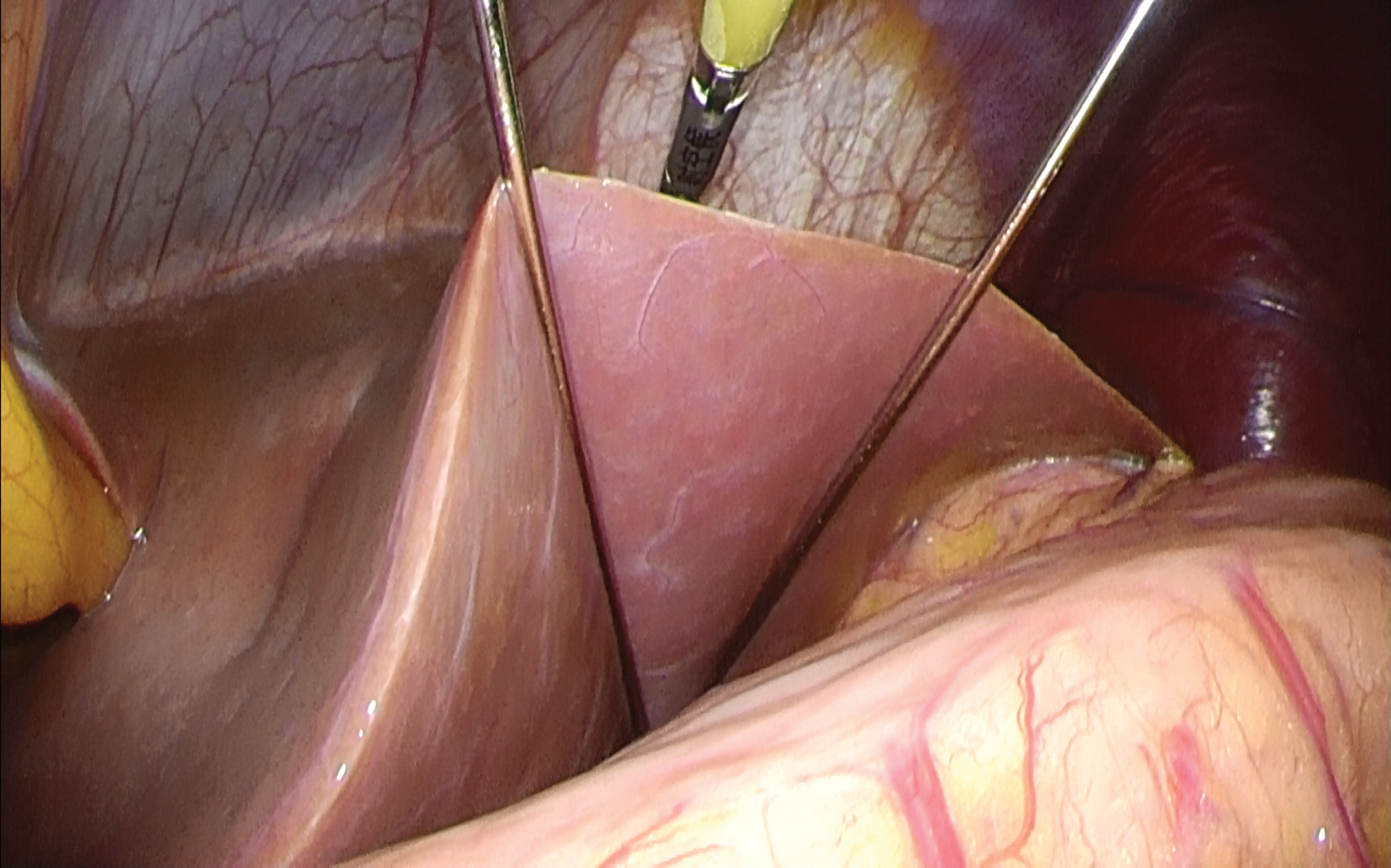
Upon the use of two K-needles, the left outer lobe of the liver was raised to fully expose the gastric fundus and cardia. Color images are available online.
A portion of the stomach wall was raised using rotatable grip pliers, and the ultrasonic knife was used to incise the gastrocolic ligament in the hemal arch. The greater curvature was then fully dissociated from 4 to 6 cm above the pylorus to the angle of His, after which a 32F. Bougie tube was inserted by mouth into the patient's stomach. When the tube tip had passed through the pylorus, the stomach was resected along this Bougie tube from 4 to 6 cm proximal to the gastric pylorus to 1 cm left of the angle of His with an initial two purple and following several blue 60-mm Endo-GIA Tri-Staplers. The seromuscular layer along the entire staple line was then continuously sutured using 3-0 sized absorbable barbed threads. After adequate hemostasis, K-needles and the single-port device were removed and the excised tissue was collected from the 2 cm arc-shaped incision.
No blue methylene tests or drainage tubes was employed during SITU-LSG, and 2-0 absorbable sutures were used to close all fascial defects.
Postoperative management and follow-up
On days 1–3 postoperatively, upper gastrointestinal contrast was conducted. If no abnormalities were observed, patients were allowed to freely drink water and were placed on a liquid diet. Patients were discharged when they were able to drink and consume a liquid diet without significant vomiting or discomfort. Patients were administered daily esomeprazole (40 mg) for 1 month, and all were given preventative vitamin and microelement supplements. Follow-up visits were conducted at 1, 6, and 12 months after surgery. During follow-up visits, patient weight, height, abdominal circumference, blood pressure, routine blood work, routine urine analyses, feces, liver and kidney function, blood nutrition indicators, lipid/sugar metabolism indicators, abdominal ultrasound scans, gynecological ultrasound scans, and polysomnographic findings were assessed.
In addition, patients completed the generic Medical Outcomes Study Short Form-36 (SF-36) questionnaire at each follow-up time point. This questionnaire is widely used to assess quality of life after bariatric surgery based on eight indices: physical functioning (PF), role-physical functioning (RP), role-emotional functioning (RE), social functioning (SF), bodily pain (BP), mental health (MH), vitality (VT), and general health (GH).20–24 These indices can in turn be used to calculate physical component summary (PCS) and mental component summary (MCS) index values. The scale additionally includes an item assessing changes in health over the past year referred to as health transition (HT). SF-36 scores ranged from 0 to 100, with 100 corresponding to the best health-related quality of life.
Statistical analysis
Patient demographic and clinical characteristics including gender, complications, and comorbidities are reported as proportions. Data normality was assessed through the Kolmogorov–Smirnov test. Continuous variables that were normally distributed are given as means ± standard deviation, whereas they were otherwise given as medians and ranges. Continuous data were compared through paired t-tests or paired Wilcoxon signed-rank tests using SAS Enterprise Guide 6.1 (SAS Institute, NC, USA), with p < 0.05 as the significance threshold for these analyses.
Results
Patient demographic characteristics
All 13 adolescent patients completed 1-, 6-, and 12-month postoperative follow-up visits. The preoperative age, weight, height, and BMI of these patients were 16.46 ± 1.98 years, 123.35 ± 22.64 kg, 171.31 ± 9.06 cm, and 41.73 ± 5.03 kg/m2, respectively. In total, 2, 2, 11, 1, 1, and 1 patients had been preoperatively diagnosed with type 2 diabetes mellitus (T2DM), hypertension, fatty liver, OSARS, hyperuricemia, hyperlipidemia, and PCOS, respectively. Patient demographic characteristics are summarized in Table 1.
Demographic Characteristics of the Sample (n = 13)
Mean ± SD.
No. (%).
BMI, body mass index; OSARS, obstructive sleep apnea syndrome; PCOS, polycystic ovary syndrome; SD, standard deviation; T2DM, type 2 diabetes mellitus.
Surgical outcomes
SITU-LSG was successfully performed in all patients without the need for any additional incisions or conversion to open surgery. Operative duration, intraoperative blood loss, duration of postoperative hospitalization, and hospitalization expenses for these patients were 90 (70–130) min, 20 (5–50) mL, 3 (2–5) days, and 58161.62 ± 6595.56 yuan, respectively.
No patients experienced postoperative mortality, leakage, stenosis, bleeding, gastroesophageal reflux disease, malnutrition, incisional infections, or hernias. Two patients developed severe nausea and vomiting that were not alleviated after 1 month of conservative treatment, but that improved after dietary changes, esomeprazole, and ondansetron hydrochloride tablet administration. In addition, two female patients suffered from alopecia that lasted 4–7 months after surgery, but that resolved spontaneously. Surgical outcomes for all patients are summarized in Table 2.
Operative Data of the Sample (n = 13)
Median (range).
Mean ± SD.
No. (%).
SITU-LSG efficacy
At 12 months post-SITU-LSG, the weight of these patients declined from 123.35 ± 22.64 to 84.31 ± 10.91 kg, whereas BMI values fell from 41.73 ± 5.03 to 28.20 ± 2.27 kg/m2 (p < 0.001). In addition, the percentage of excess weight loss (%EWL) for these patients was 67.97% (56.00–110.70%), whereas their height rose from 171.31 ± 9.06 cm preoperatively to 172.62 ± 8.66 cm postoperatively (p < 0.05).
Within this 1-year postoperative period, two cases (100%) of T2DM, two cases (100%) of hypertension, eight cases (72.73%) of fatty liver disease, nine cases (81.82%) of OSARS, one case (100%) of hyperuricemia, and one case (100%) of hyperlipidemia were cured in these patients. Although the patient with PCOS was not cured of this condition during the study period, her androgen levels had returned to normal and her menstrual cycles had normalized (30–45 days) after surgery. The overall efficacy of this SITU-LSG procedure in this Chinese population is outlined in Table 3. In addition, gross appearance and postoperative abdominal status are shown in Figures 5 and 6. 19

SITU-LSG specimen. SITU-LSG, single-incision trans-umbilical laparoscopic sleeve gastrectomy. Color images are available online.

Abdominal status after SITU-LSG. Color images are available online.
Clinical Efficacy of Single-Incision Trans-Umbilical Laparoscopic Sleeve Gastrectomy (n = 13)
p Value for preoperative values compared with 12 months postoperative values. Significant p values are in italics.
Mean ± SD.
Median (range).
No. (%).
EWL, excess weight loss.
Changes in quality of life
We assessed patient quality of life based on postoperative SF-36 scores (Table 4). At 12 months postsurgery, these scores had significantly improved relative to preoperative levels with respect to PF, RP, RE, SF, BP, MH, VT, GH, HT, PCS, and MCS (p < 0.01).
SF-36 Scores (n = 13)
p Value for preoperative values compared with 12 months postoperative values.
Significant p Values are in italics.
Median (range).
BP, bodily pain; GH, general health; HT, health transition; MCS, mental component summary; MH, mental health; PCS, physical component summary; PF, physical functioning; RE, role-emotional functioning; RP, role-physical functioning; SF, social functioning; VT, Vitality.
Discussion
Patients typically seek bariatric surgery as an approach to improving their overall health and appearance. Standard LSG operations typically utilize multiple ports, potentially leading to unsightly scarring. To decrease the length of the umbilical incision in these procedures and to eliminate other surgical scarring, we conducted a SITU-LSG procedure using a small (2 cm) umbilical incision. By placing a single-port device into the umbilical fossa, we were thus able to mask surgery-associated scarring, thereby significantly improving aesthetic outcomes for these patients.
Although the aesthetic gains associated with this procedure are promising, SITU-LSG is also more challenging than traditional LSG and prolongs the overall operative duration and associated risk of surgery-related damage,25–28 thus raising the question of whether or not it is worthwhile to conduct SITU-LSG in obese adolescent patients. Herein, we found that the average operative duration, intraoperative blood loss, duration of postoperative hospitalization, and hospitalization-associated expenses for Chinese adolescent patients who underwent SITU-LSG were 101.54 min, 25.38 mL, 3 days, and 58161.62 yuan, respectively. In addition, these patients did not experience any incidence of mortality, leakage, stenosis, bleeding, gastroesophageal reflux disease, malnutrition, incisional infection, or hernia during follow-up.
Two patients suffered from severe nausea and vomiting, whereas two patients experienced alopecia after treatment. In both cases, symptomatic therapy was sufficient to alleviate these complications without decreasing patient quality of life. Our results are consistent with those of prior studies.26–29 As such, we can conclude that SITU-LSG represents a safe and effective approach to treating obese Chinese adolescents.
However, it is essential to note that our follow-up duration was limited, and as such we cannot preclude the possibility that SITU-LSG may be associated with long-term complications such as trocar site hernias, which often only manifest several years after single-incision laparoscopic surgery.30–32 Studies with a longer follow-up period will thus be required to definitively establish the safety and feasibility of SITU-LSG.
At 12 months postsurgery, the BMI of these patients had declined significantly from 41.73 ± 5.03 to 28.20 ± 2.27 kg/m2, with an average %EWL of 72.01%. Overall, these patients exhibited rapid weight loss and an increase in height over the follow-up period. At 1 year postoperatively, the height of these patients had risen from 171.31 ± 9.06 to 172.62 ± 8.66 cm (p < 0.05), which may suggest that these patients were able to maintain adequate nutrition after SITU-LSG, thereby supporting normal growth and development. Rates of comorbidities in these adolescents had also fallen at this follow-up time point, with respective T2DM, hypertension, fatty liver, OSARS, hyperuricemia, and hyperlipidemia remission rates of 100%, 100%, 72.73%, 81.82%, 100%, and 100%. As such, SITU-LSG was an effective approach to achieving weight loss goals and reducing comorbidity rates in Chinese adolescents.
Bariatric surgery has been shown to markedly improve the quality of life of obese adolescents,33–36 but to date, studies have not evaluated dynamic changes in obese adolescent quality of life after SITU-LSG.
Herein, we found that PF, RP, RE, SF, BP, MH, VT, GH, HT, PCS, and MCS were all significantly improved at 12 months post-SITU-LSG relative to preoperative values. The majority of these values had improved within 1 month after surgery, with the exception of BP, which improved within 6 months postsurgery. We hypothesize that this delay may have been due to a failure to alter eating habits, resulting in instances of nausea and vomiting when patients ate too quickly. In this sense, our results were consistent with those of a study of traditional multiport LSG, 15 demonstrating the ability of SITU-LSG to improve overall quality of life for obese Chinese adolescents. At 1-year postoperatively, PF, RP, BP, GH, VT, SF, RE, and MH were 94.62, 100, 100, 88.23, 93.85, 97.43, 100, and 90.46, respectively, in this patient cohort, thus confirming the ability of SITU-LSG to improve patient quality of life.
Our results demonstrate that SITU-LSG can be safely and effectively performed as a means of improving cosmetic outcomes and quality of life for Chinese adolescents.
However, it is important to note that this procedure is not appropriate for all adolescents. For example, Maluenda et al. 8 suggested that SITU-LSG can only be successfully performed for select obese individuals with a BMI <40 kg/m2 using a unique access device together with conventional laparoscopic instruments, whereas Sucher et al. 11 suggested that without liver retraction, SITU-LSG can only be conducted in patients with a BMI <45 kg/m2. Based on our experience, performing SITU-LSG in patients with a BMI >50 kg/m2 may be very challenging, greatly elevating the risk of intraoperative bleeding and prolonging the overall operative duration. We found that the SITU-LSG procedure was still safe and feasible for patients with BMI values between 45 and 50 kg/m2 owing to our use of a K-needle and rotatable pliers.
The operative duration, intraoperative blood loss, postoperative hospitalization duration, and hospitalization expenses of the patient with the largest BMI in this study (48.67 kg/m2) were 120 min, 20 mL, 2 days, and 52195.00 yuan, respectively, with all of these values being within acceptable ranges. As such, we believe that SITU-LSG can be safely conducted in obese adolescents with a BMI <50 kg/m2 when K-needles and rotatable pliers are used. Owing to the associated advantages, we utilized K-needles for all reduced port LSG procedures. A single K-needle offers as much utility as a grip plier, and it can fully expose the cardia and gastric fundus.
However, it is important that the K-needle depth be carefully controlled when puncturing the right diaphragm crus to avoid damaging the proximal large blood vessels. In our experience, this depth must remain <10 mm. In addition, the abdominal wall was punctured with the sharp tip of the K-needle, whereas the blunt end was used to insert into the right diaphragm crus to prevent liver hemorrhage or pneumothorax. When the blunt end of this needle contacts the liver or diaphragm, bleeding or pneumothorax will only occur when a significant external force is applied.
In addition, the K-needle used for this procedure had a diameter of just 1.5 mm, such that any bleeding that may occur upon liver puncture would be minimal and could be readily stopped using an ultrasonic knife. Similarly, if this needle were to puncture the diaphragm, this muscle would contract, thereby closing the resultant wound and preventing the occurrence of severe pneumothorax. The sharp end of the K-needle has the potential to injure the hands of the operating surgeon, and as such, we utilized an injector cap to mitigate this risk (Fig. 7). We did not detect any instances of pneumothorax or large blood vessel puncture in this study, whereas one patient experienced liver hemorrhage caused by K-needle puncture, and this hemorrhage was rapidly stopped using an ultrasonic knife.

After using an injector cap, no further damage to the operating surgeon's hands occurred. Color images are available online.
In addition, one surgeon experienced a hand injury induced by the sharp end of the K-needle. However, after the use of an injector cap, no further injuries occurred. As such, we believe that K-needles can be safely and effectively used to conduct reduced port LSG procedures.18,19 The primary technical difficulties associated with reduced port LSG include the challenges of instrument navigation within a limited area of movement and the loss of the classic laparoscopic triangle. However, by using rotatable pliers, it is possible to enlarge the operative field and to thereby make it easier to conduct laparoscopic dissection and suturing when performing reduced port LSG. As such, we utilized rotatable pliers for all reduced port LSG procedures.
Conclusions
These data demonstrate that SITU-LSG is an effective and safe approach to treating Chinese adolescent patients, improving overall quality of life while achieving satisfactory aesthetic outcomes. However, the sample size of this study was limited, and we did not directly compare outcomes associated with SITU-LSG and traditional multiport LSG procedures. As such, future large-scale prospective randomized controlled trials will be necessary to validate and expand upon our results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This article was supported by Beijing Municipal Science & Technology Commission, No. Z191100006619043.