
Abstract
Introduction:
Determinants of weight gain after bariatric surgery have not been sufficiently studied from the patients' perspective.
Objective:
The present qualitative study aims to identify these determinants and needs of patients to counteract them.
Methods:
Well after their surgery, in 2018 we interviewed 13 patients in France, with two focus groups: the success group (“SG”) comprising patients who reached the desired weight, and the weight recidivism group (“WRG”) comprising patients who had regained weight 2–12 years after surgery.
Results:
While SG patients were relatively satisfied but remained vigilant, WRG patients were lacking in confidence. Determinants of weight gain declared by patients were environmental, physiological, psychosocial, and lifestyle related; they were also impacted by the patient–physician relationship. We noted that WRG patients cited more external factors than did SG patients. Means to avoid weight gain were more psychological than physiological or environmental; when expressed, they were primarily associated with internal factors.
Conclusion:
This study highlights weight gain factors as seen from the patients' perspective. Educational sessions are predicated on identification of their means of avoiding weight gain. In this work, “locus of control” emerges as a key predictive factor of bariatric surgery success.
Introduction
For obese persons, compliance with prescriptions in dietary regimens is quite important but not easy to maintain. 1 In cases of failure to lose weight, bariatric surgery is viewed as a form of metabolic and mechanical assistance enabling a patient to reduce the amount of food consumed (principle of restriction) and/or to reduce food assimilation (principle of malabsorption). 2 In France, bariatric surgery has been experiencing a major boom. The number of surgical interventions has tripled since 2006 with a major increase of Sleeve Gastrectomy.
Clinical success of bariatric surgery is defined as an excess weight reduction (EWR) of a minimum of 50% 3 and clinical failure as weight regain of more than 5% of EWR within 12 months after surgery. In fact, 10–40% of patients regain weight in the long term or do not lose weight, 4 and 50% of patients regain more than 5% of EWR in 48 months.
The failure rate depends on several factors: anatomical/surgical elements, metabolic/hormonal imbalance, and behavioral aspects. 5 In some cases, surgery itself can cause weight regain, 6 and the failure rate can reach 76% within 6 years. 7 In addition, physiological factors can explain failure: habituation of the intestines to the “new digestive circuit” with optimization of their capacities of nutrient absorption, 8 appetite increase due to a neural-endocrine metabolic response, and increase of energy conservation in response to long-term deprivation. Furthermore, eating behavior disorders 9 and lack of integration of lifestyle and dietary measures due to the maintenance of poor nutrition and exercise habits4,10 are the main failure determinants identified in the literature. Some authors have gone so far as to criticize the trend suggesting that surgery cures obesity and contend that surgery can only be envisioned concurrently with the behavioral change required in chronic disease management. 7 Other determinants have been mentioned, without full consensus having been achieved, 11 such as age, 12 geographical origin or ethnicity, 13 socioeconomic level, 14 and comorbidities. Finally, nonmanagement of negative emotions like boredom, stress, anxiety, lack of self-esteem, depression, and emotional shock contributes to weight regain. 15
While several studies have tried to identify these determinants, in most cases retrospectively, few of them have directly questioned patients about their vision of the causes and prevention of weight regain, even though this type of interrogation is essential to high-quality and adapted care. 16 The purpose of this study was to identify the determinants of weight regain after bariatric surgery and to identify the needs of patients who failed to reach expected targets of the surgery, as viewed from their own perspective.
Methods
Personal characteristics of research team
The interviewer was a female dietician practicing in the clinic for 4 years, with a Master's degree in health promotion. The observer was a psychologist who has been working in the same clinic for 12 years.
Relationship with participants
Patients with bariatric surgery were divided into two groups: Success Group (SG) for those whose EWR exceeded 50% and Weight Recidivism Group (WRG) when it failed to do so 2–12 years after the most recent surgery. Using medical records, the dietician phoned 16 SG patients and 22 WRG patients. She was known by patients for having organized educational sessions, for which two patients had served as cofacilitators.
Participant selection
Purposive participant selection was carried out. Messages on mobile phones asking the patients to call back the focus group were sent out. One reminder phone message was sent to both groups. Among the 14 contacted SG patients, 7 agreed to participate, except for one who was absent during the focus group, while 3 others refused and 3 did not answer. Finally, among the 16 contacted WRG patients, 6 accepted, 4 refused, and 6 failed to answer. Current mean body mass index (BMI) was 25.01 kg/m2 in SG and 38.96 in WRG.
Setting
The focus groups took place on June 11, 2018, from 10:00 to 12:00 for WRG and from 14:00 to 16:00 for SG in the clinic meeting room.
Participant characteristics
There were four (31%) male and nine (69%) female patients, and they were 49 ± 11 years old (28–68): 52 ± 10 (43–68) years old in WRG and 45 ± 12 (28–61) years old in SG. Characteristics of the two groups were homogeneous for sex (1/6 male in WRG and 3/7 in SG); presurgery maximum BMI (51.29 vs. 48.36 kg/m2); postsurgery minimum BMI (32.75 vs. 23.32 kg/m2); family situation (3/6 with children and 3/6 in couple in WRG and 3/7 with children and 5/7 in couple in SG); professional situation (3/6 inactive vs. 1/7 inactive); and localization (5/6 urban vs. 4/7 urban). We noted a difference in levels of precarity with two people in WRG and number of previous bariatric surgeries (4/6 in WRG and 1/7 in SG) (Table 1).
Characteristics of Study Participants (n = 13)
BMI, body mass index; SG, success group; WRG, weight recidivism group.
Data collection
A sociodemographic questionnaire was filled out before the focus groups came into being. A focus group guide was created and tested by the research team. Patients were welcomed to the meeting room with coffee and tea. The rules were explained (mutual respect, no phone), and the same general question was put forward on the participants' feelings about their current situations. The discussions were recorded as an audio file with the agreement of both groups. The focus groups took place in a confidential area and lasted about an hour and a half. The animator allowed each participant to speak with a pleasant climate and underlined different remarks that called for further reflection. The observer jotted down notes during both focus groups.
Data analysis
All data were processed anonymously. The verbatims were not shared with the participants. Idea saturation was sought out and achieved. Content analysis was the methodological orientation chosen to underpin this study. Analysis was processed by examination of the verbatims, in three phases: (i) extraction of all information, (ii) detection of the relevant data, and (iii) organization in logic trees. The themes were not identified in advance. The analytical “triangulation” method was applied, which meant that in case of discrepancies in coding between two coders, the third coder decided.
Consent and approval
Oral consent was requested from all patients after their having received an information note. As this study was in the field of human and social science, it did not depend on the French law (decree 2017-884 of May 9, 2017) because its aim was not to develop knowledge in biology or medicine but rather in psychosocial science. Approval by the local institutional review board was consequently not needed.
Results
On the one hand, WRG patients declared that their current situation was “difficult,” “unfair,” “painful,” like an “obsession,” a “punishment.” They reported feeling guilty, sad, powerless, worried, and desperate. They had lost confidence in themselves. On the other hand, SG patients reported feeling “well,” “serene,” “without hungry feeling” but characterized their situation as an “obsession” because they were “afraid of weight recidivism” and had to remain “vigilant.” Some of them did not recognize themselves and thought that they were “too thin” (Supplementary Table S1). Determinants of weight recidivism are illustrated in Figure 1. Some of them were common to both groups. They can be divided into three themes:

Tree of determinants of weight regain. SG, success group; WRG, weight recidivism group.
Physiological determinants: water retention, body memory, hungry, absence of satiety, excess weight loss;
Lifestyle determinants: little physical activity, inactivity, snacking, irregular meals;
Psychosocial determinants: stress, anxiety.
Three determinants were specific to SG: boredom, annoyance, lack of vigilance.
The determinants declared by WRG patients were more numerous and can be classified as
Physiological: genetics, change of metabolism, aging, menopause, sugary appetence, gluttony, drinking during meals;
Environmental: family environment, social and professional life, lack of physician empathy, life trauma;
Psychological: being unable to regularly monitor, unable to say no, addiction problems, long-term diet, embarrassment, tiredness, problems unsolved before surgery (Supplementary Table S2).
Means to avoid weight recidivism are illustrated in Figure 2. Some of them are common to both groups. They can be divided into four themes:
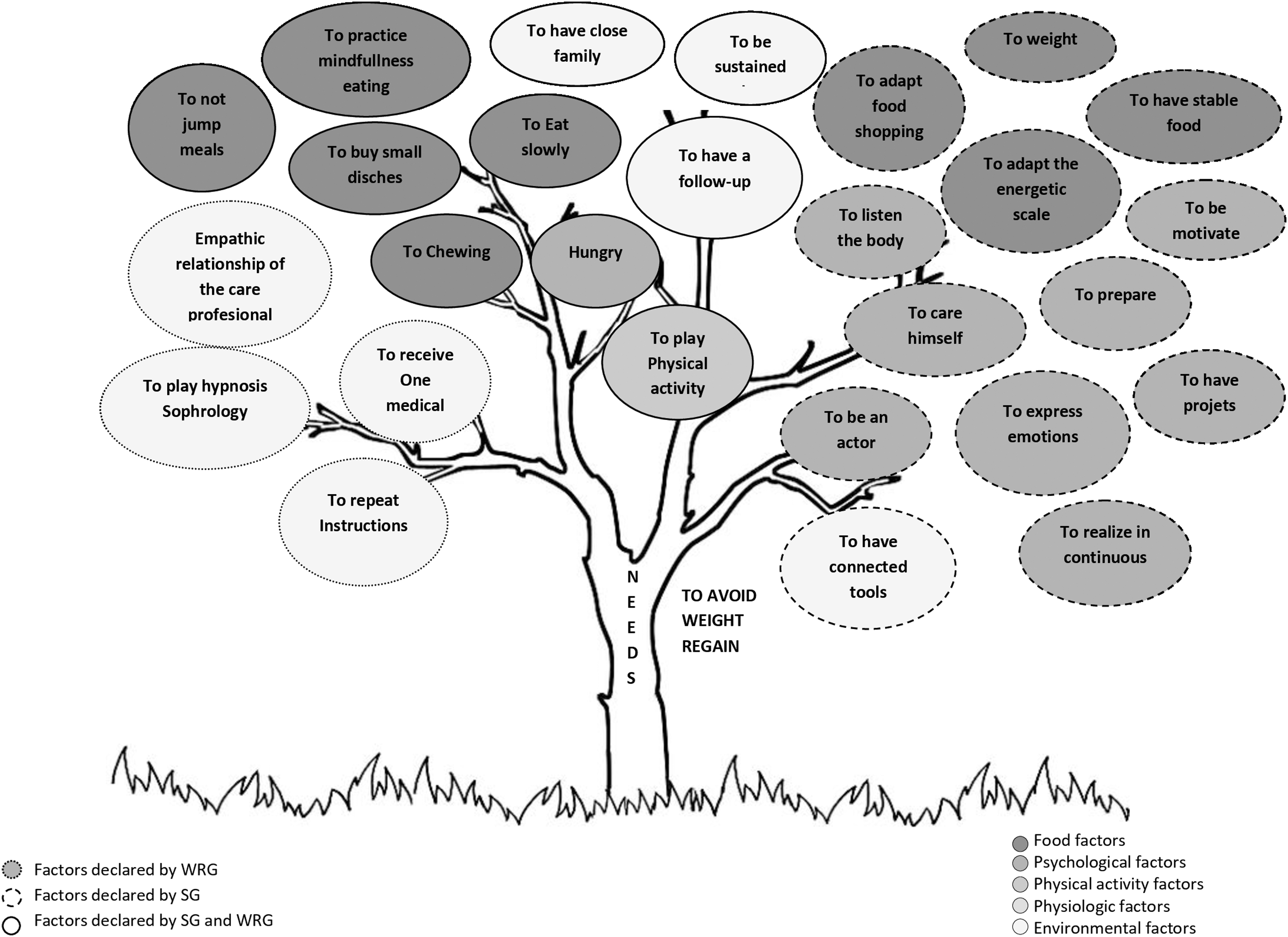
Tree of needs to avoid weight regain.
Physiological: chewing;
Lifestyle: eating slowly, having regular meals (no skipping meals), engaging in physical exercise, taking small portions;
Psychosocial: mindful eating;
Environmental: being supported, joining associations and patient education programs, being regularly monitored by a surgeon.
Two means were specific to SG patients:
Environmental: Empathetic physician and nursing staff, with a coherent, repeatedly transmitted set of instructions; Psychological: Stress management strategies such as hypnosis and sophrology.
The means evocated by WRG patients were more numerous:
Lifestyle: weight, balanced meals, mindful food shopping;
Psychosocial: motivation, expression of emotions, having life plans, listening to one's body, taking proper care of oneself;
Environmental: being well-prepared, having connected tools (Supplementary Table S3).
Discussion
The present study is one of the first to highlight patients' views about weight regain determinants after bariatric surgery and their means of avoiding it, with the active participation of two groups: those who regained weight and those who did not.
One of the strengths of the study is the focus group method, with specific attention given to the free participation of each person and closure when the ideas had reached saturation. It facilitated interaction between participants. Another strength is to have collected point of views of two different groups (with and without weight regain).
One of the limitations of the study is the low number of participants, as results about patients' points of view could not be representative of targeted study's population. However, in qualitative studies, the number of participants is allowed to be low if idea saturation is reached. Indeed, according to focus group methodology, idea saturation is reached when no new information is brought forth. Then, the focus group session can end. Nevertheless, these results need to be confirmed by a quantitative study, which could assess frequency of each weight regain factor on a representative patient sample. Another limit could be the neutrality of the animator who conducted the focus groups because she was a medical team member. So, patients were able to identify her as a health professional, and this may have led to information bias because of reluctance to candidly express their thoughts and fear of being judged. However, she was not known by the included patients, and she achieved idea saturation which underscores the quality of qualitative studies. Another limit consists in the differences between the groups in terms of number of previous bariatric surgeries and levels of precarity. However, other characteristics were similar. Moreover, according to the Prochaska model, change depends on number of failures, and possibly in this context on number of surgeries.
Patients' views about weight regain determinants were totally different in the two groups. While SG patients were pleased but vigilant, WRG patients had lost self-confidence, as was to be expected. Daily life after bariatric surgery has been characterized in the literature as constraining because body attention is permanent. Weight gain is associated with stress, shame, feeling of failure, and self-disdain, 17 and it can lead to social isolation. 18
From the patients' discourse, we can classify weight regain determinants and means of avoidance according to the Dahlgren and Whitehead model of health determinants. 19 We found these determinants to be, from micro to macro: physiological, lifestyle, psychosocial (including social network), and environmental determinants such as the health care system, particularly professional caregivers' attitudes. We did not find “polluted environment” determinants.
The first weight regain determinants declared by WRG patients were physiological, with increased food intake during meals due to lessened feeling of fullness. This determinant is often the central factor that a physician takes into account.
The lifestyle determinants had to do with sedentariness and lack of physical activity. Another study showed that 41 of the 100 patients who had undergone bariatric surgery 1 year before were no longer respecting physical activity guidelines. 20 More precisely, if the patient had been active before surgery, his/her physical activity would be easier to maintain, 21 but if he/she hadn't exercised for a long time, his/her motivation would be harder to (re)create in view of finding the activity best adapted to him/her. 22
An oft-mentioned psychosocial determinant was difficulty in controlling one's emotions in situations where food becomes an outlet, a way to cope with uneasiness. These correspond to the concept of emotion-induced changes of eating. 23 Eating so as to feel better or to avoid negative feelings is a more and more frequently cited cause in obesity pathology. 24 As a result, food behavior troubles have got to be screened before and after surgery.
Finally, environmental determinants are among the weight regain determinants admitted by patients, whose capacity to adapt themselves to their environment is a predictor of success. On that subject, we noted a lack of awareness of the effects of pollution on obesity, even though chemicals are now known to be obesogenic through metabolic disruption and adipose tissue inflammation. 25 As regards capacity of adaptation, it would seem that care professionals have an influence on diligence; in contrast, it has been shown that patients experiencing weight regain are often frustrated by their doctors' lack of understanding. 22
All patients justify their behavior with determinants concerning the locus of control, which can be internal or external. If the patient thinks that behavioral consequences depend on his own choices, his locus of control will be internal. On the contrary, if that person thinks that behavioral consequences depend on random factors (luck, destiny, God, others), his locus of control will be external. 26 In our study, different declared weight regain determinants could be considered as external, especially for WRG patients. It has been shown that “external” patients have more food behavior troubles before surgery than resilient patients. 27 It has also been shown that some patients react to initial weight loss as passive spectators and are unprepared for subsequent weight regain. 28 In our study, SG patients defined themselves as actors in their care pathway and success. They intervened in the decision-making process by coping with situations and mobilizing their resources or psychosocial skills (capacity to control their lives, self-efficacy, problem solving, decision-making). 29 As patients with an internal locus of control are more compliant to health guidelines, 30 it would be interesting to compare locus of control between the two groups using a validated scale 31 so as to determine whether locus of control could be a predictor of weight regain. As regards means of avoiding weight regain, while physiological determinants have often been declared as key, psychosocial determinants are even more frequently cited. Lifestyle needs are important more in terms of food modalities (eating slowly, having regular and balanced meals, not skipping meals, taking small portions, weighing oneself, engaging in vigilant food shopping…) than in terms of physical exercise. These needs are the same as those mentioned in professional guidelines. 32 The psychosocial skills declared by patients correspond to the five basic areas of life defined by the World Health Organization: decision-making and problem solving; creative critical thinking; communication and interpersonal skills; self-awareness and empathy; coping with emotions; and coping with stress. 33
Among environmental health determinants, while means of weight regain avoidance associated with work or home conditions were scarcely mentioned, determinants associated with the health care system were emphasized, such as being adequately prepared for surgery, as recommended by professionals. 34 Moreover, patients tend to desire long-term follow-up after surgery, 35 with competent professionals who listen attentively. Patients need to be understood and supported. The two groups think that individual consultations should be completed by discussion groups, as has been found in other studies. 36 Indeed, additional support and help with emotional eating are desired, especially by patients experiencing weight regain significantly associated with life events. 37
In this way, while weight regain factors are mostly external, we found that the means of avoiding weight regain are primarily internal. In the study by Anastasiou et al., 38 obese patients with high internal locus think that their health depends on their behavior and lose weight more often than “external locus” patients, who think that their health problems depend on others, such as health professionals. 39 An internal locus of control positively influences treatment compliance, improves coping, and empowers patients. 40 Healthy behavior and weight loss are thereby developed. On the contrary, external locus of control will have unfavorable effects on health, as has been demonstrated by Sonntag et al. 39 Undergoing weight loss surgery is anything but a quick fix. 37 It requires patient empowerment with appropriate educative methods. 41 When they are properly applied, bariatric surgery complemented by medically supervised weight management program is beneficial for treatment of weight regain and may help the patient to achieve long-term weight loss success. 42 Educational sessions about physical activity, food, environmental health, emotion management, everyday life management, and support groups can develop the psychosocial skills needed to better understand and adhere to health care rules complementarily to physical treatment. For example, a patient should be prepared to work through whatever emotions are associated with weight fluctuations. 43 Education and counseling should be proposed for individuals, couples, and families and occur during all phases of bariatric surgery. Moreover, these sessions should use communication techniques that empower patients to deflect negative comments and influences in a constructive manner and render their positive approach meaningful.29,44
Conclusion
The weight gain determinants declared by both concerned and nonconcerned patients showed that preparation to bariatric surgery is essential and should include educational sessions about health determinants: not only physiological but also psychological, social, and environmental. Educational sessions with support groups are likewise to be recommended.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.