
Abstract
Background:
The most effective treatment for permanent weight loss is bariatric surgery. The present study aimed to evaluate the early period effects of laparoscopic Roux-en-Y gastric bypass (LRYGB) and laparoscopic one-anastomosis gastric bypass (LOAGB) surgeries on the clinical and metabolic results.
Materials and Methods:
A total of 80 patients underwent bariatric surgery. The patients in Group I (n = 42) underwent LRYGB, and patients in Group II (n = 38) underwent LOAGB.
Results:
Clinical and laboratory improvements were detected in all diabetic patients in both groups starting from the third month after surgery. Third month and sixth month after surgery, more rapid diabetes regulation was detected in Group II (p = 0.0019 and p = 0.0016). There was an improvement in arterial blood pressure, total cholesterol, triglyceride, and low density lipoprotein in both groups. The decrease in body mass index was statistically higher in third- and sixth-month controls in Group II (p = 0.004, and p = 0.003). The ratios of excess weight loss % (EWL%) in the third- and sixth-month controls were higher in Group II, which was statistically significant (p = 0.007, and p = 0.008).
Conclusions:
One-anastomosis gastric bypass is associated with more rapid EWL% and type 2 diabetes remission; also, not inferior to RYGB in terms of other metabolic parameters.
Introduction
Obesity is one of the most important health problems in the world. According to the World Health Organization (WHO), more than 650 million adults were obese in the world in 2016, and by 2030, if recent secular trends continue unabated, the absolute numbers were projected to total 2.16 billion overweight and 1.12 billion obese individuals. 1 Bariatric surgery is the most effective treatment for severe obesity and is successful in the treatment of obesity-related comorbidities, particularly type 2 diabetes mellitus (T2DM). 2 In a systematic review and meta-analysis study, Cheng et al., compared bariatric surgery and medical treatment in obesity treatment. Weight loss and diabetes remission, the primary end point of the study, were statistically more significant in patients undergoing bariatric surgery (p < 0.05). 3
Various procedures have been described for the treatment of obesity since 1954. According to The International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) 2016 data, the most common bariatric surgery is sleeve gastrectomy (SG), followed by Roux-en-Y gastric bypass (RYGB) and one-anastomosis gastric bypass (OAGB), respectively. 4 Which surgical technique is superior in terms of weight loss and control of comorbidities in the treatment of obesity? The answer to this question continues to be discussed.
Laparoscopic RYGB (LRYGB) has become one of the gold standard operations in morbidly obese patients, especially with metabolic disorders, after being described by Wittgrove in 1992.5,6 The OAGB, also known as “mini-gastric bypass” technique, first described by Robert Rutledge in 1997, aims to reduce the operative time, simplify the procedure, and reduce complications. The most important difference of this technique from RYGB is that the single anastomosis does not disturb the intestinal integrity and reduces the operative time and reduces surgical complications. 7 The clinical results varied in morbidly obese patients in accordance with the preferred surgery technique. The main objective in the obesity surgery is the treatment of comorbid disease and to improve the quality of life with weight loss.
The primary outcome parameter was to evaluate the early period effects of LRYGB and laparoscopic OAGB (LOAGB) surgeries on the clinical and metabolic results. Secondary outcome was excess weight loss % (EWL%).
Materials and Methods
A retrospective analysis was conducted on obese patients who underwent bariatric surgery in Istanbul University Istanbul Medical Faculty General Surgery Department between November 2016 and July 2018. A specialist in endocrinology and metabolism examined all patients before surgery after they were admitted to the hospital. The informed consent form was obtained from all patients. All patients underwent preoperative gastroscopy. The inclusion criteria were as follows: patients between the ages of 18 and 65 years with body mass index (BMI) of 40 or 35 kg/m2 with comorbidity and failure to achieve permanent weight loss by nonsurgical methods. Exclusion criteria were previous obesity surgery or gastrointestinal system surgery, pregnancy, and uncontrolled psychiatric illness. The surgeon and the patient decided together which surgical technique to perform.
The patient data, including age, height, weight before the surgery and weights in the controls, arterial blood pressure (BP), BMI, glycosylated hemoglobin A1c (HbA1c), fasting blood glucose (FBG), blood fasting insulin level, insulin resistance index (homeostasis model of assessment insulin resistance [HOMA-IR]), cholesterol, triglyceride, low density lipoprotein (LDL), high density lipoprotein (HDL), iron, total iron binding capacity (TIBC), folate, vitamin B12, total protein, albumin, and EWL% in the controls, were retrospectively evaluated. T2DM was defined as an HbA1c above 7.0% in the last 6 months before surgery and/or use of antidiabetic drugs. Remission was defined as HbA1c below 6.5% (42 mmol/mol) without using antidiabetic medication. Patients with HbA1c = 5.7–6.4% were defined as “patients at risk of diabetes.”
All diabetic patients in both groups had been using oral antidiabetic drugs for at least 6 months. All patients received multivitamin support after surgery (iron, B-12, folic acid, and vitamin D). Vitamin doses were adjusted according to postoperative control blood tests. The surgery data involved the surgery time and the hospital stay time. All procedures were performed by a single surgeon (U.B.) and the same surgical team. The patients were called for control visits in third month and sixth month after surgery, and height and weight were measured, and their comorbidities were evaluated.
Surgical procedure
Both surgical procedures were performed as previously described.7,8 All procedures were performed using a 30° camera and five-port technique by the same surgeon (U.B). In brief, RYGB was performed by the 70 cm of biliopancreatic limb and 150 cm of an alimentary limb. The gastric pouch was ∼15–20 cc, and the gastrojejunostomy was created by linear stapler with an anastomosis 1.2 cm diameter wide. In the OAGB procedure, after creating a narrow stomach tube (37-Fr bougie) using a linear stapler, an omega-shaped gastrojejunostomy anastomosis was performed ∼200 cm distal to the Treitz ligament.
Ethics
Board of ethics approval for this study was obtained from the Ethics Commission of İstanbul University (No.: 2017/371). All authors declare that the research was conducted according to the principles of the World Medical Association Declaration of Helsinki “Ethical Principles for Medical Research Involving Human Subjects.”
Statistical analysis
The obtained data were analyzed using the Statistical Package for the Social Sciences (SPSS) for Windows 22.0 program. The descriptive statistical methods of number, percentage, mean, and standard deviation were used in the evaluation of the data. The Student's T test was used in the comparison of the quantitative continous data between two independent groups. The difference between the repetitive measurements of the parameters was evaluated using the matched pair T-test. The obtained data were evaluated in a 95% confidence interval and in 5% significance level.
Results
Eighty patients were participating in this study. The patients in Group I (n = 42) underwent LRYGB, and patients in Group II (n = 38) underwent LOAGB. Perioperative characteristics are shown in Table 1. The mean weight of Group I was 144.730 kg and Group II was 142.180 kg. The mean BMI of Group I was 50.272 kg/m2 and Group II was 49.008 kg/m2. There was no statistical difference between age, gender, and baseline BMI in both groups. FBG, HbA1c, fasting insulin, and HOMA-IR levels were investigated as the diabetes parameters in both groups.
Perioperative Characteristics of All Patients
LOAGB, laparoscopic one-anastomosis gastric bypass; LRYGB, laparoscopic Roux-en-Y gastric bypass.
Clinical and laboratory improvements were detected in all diabetic patients in both groups starting from the third-month control after surgery. The decrease in HbA1c level was more rapid in Group II in third- and sixth-month controls, which was statistically significant (p = 0.019 and p = 0.016) (Fig. 1). In Group I, 24 patients (57.1%) were T2DM and used medications, and 12 patients were at risk of diabetes. In Group II, 21 patients (55.2%) were T2DM and used medications, and 14 patients were at risk of diabetes. At postoperative 3 months, eight patients (33.3%) in group 1 and nine patients (43%) in group 2 stopped using antidiabetic drugs. Antidiabetic drug doses of five patients (21%) in group 1 and seven patients (33.3%) in group 2 were reduced. Patients who used antidiabetic medication in both groups before surgery did not need to use the medication in the sixth-month control.
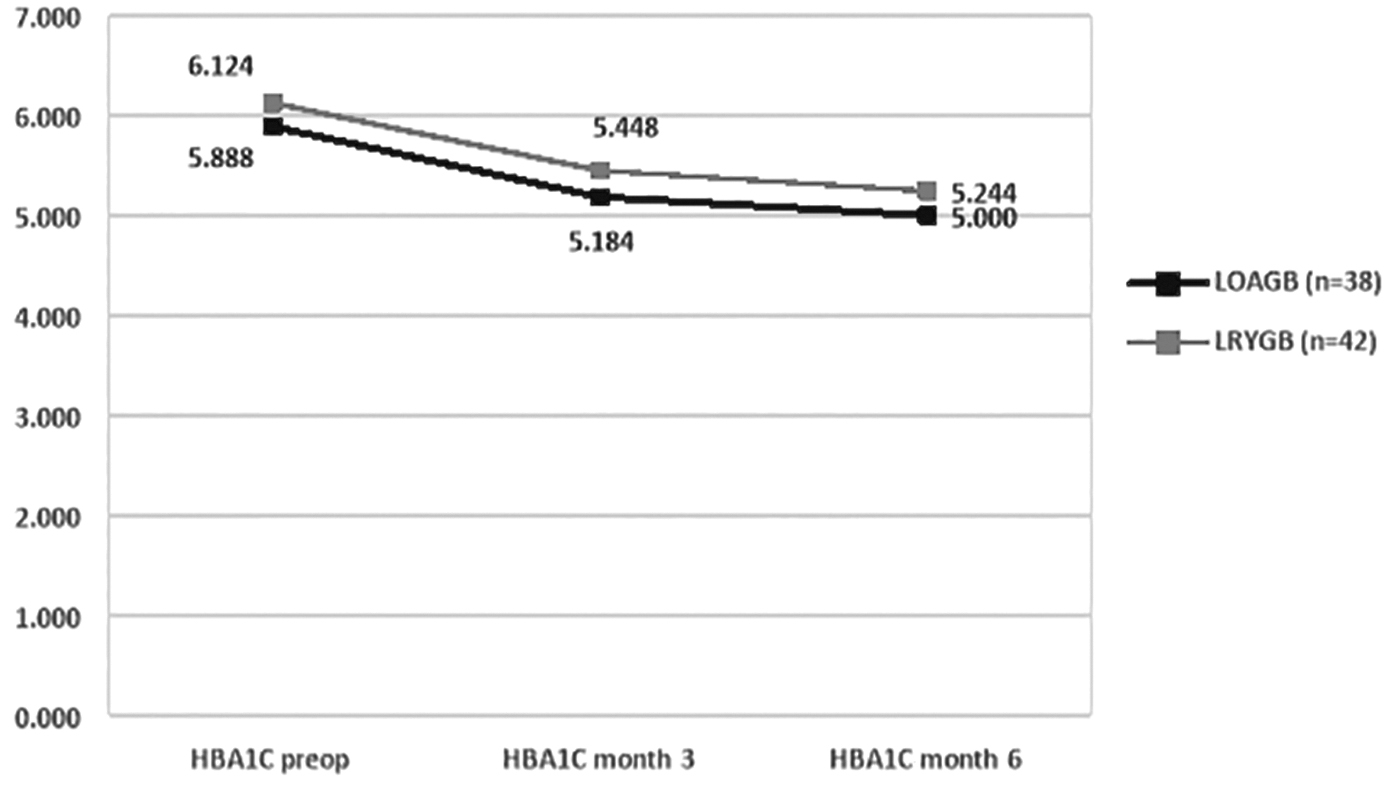
The diagram of the HbA1c measurements in accordance with the surgical technique. HbA1, glycosylated hemoglobin A1c.
A significant improvement was detected in the arterial BP in both groups. In group I, 22 patients (52.3%) were using antihypertensive drugs, and 16 of these patients (72.7%) stopped using the drug after surgery. In Group II, 20 (%52.6) patients were using antihypertensive drugs, and 15 of these patients (75%) stopped using the drug after surgery.
BMI, EWL%, and fat-free mass (FFM) levels were investigated in the evaluation of the weight loss in both groups. A significant decrease was detected in these parameters in the third-month control and sixth-month control in both groups (Table 2). Permanent weight loss was detected in the early period in both groups. The decrease in BMI was statistically higher in third- and sixth-month controls in Group II (p = 0.004 and p = 0.003) (Fig. 2). The EWL was more rapid in Group II (Fig. 3). The ratios of EWL% in third- and sixth-month controls were higher in Group II, which was statistically significant (p = 0.007 and p = 0.008). The FFM was found lower in the sixth-month control in both groups; however, there was no statistical difference between the groups.
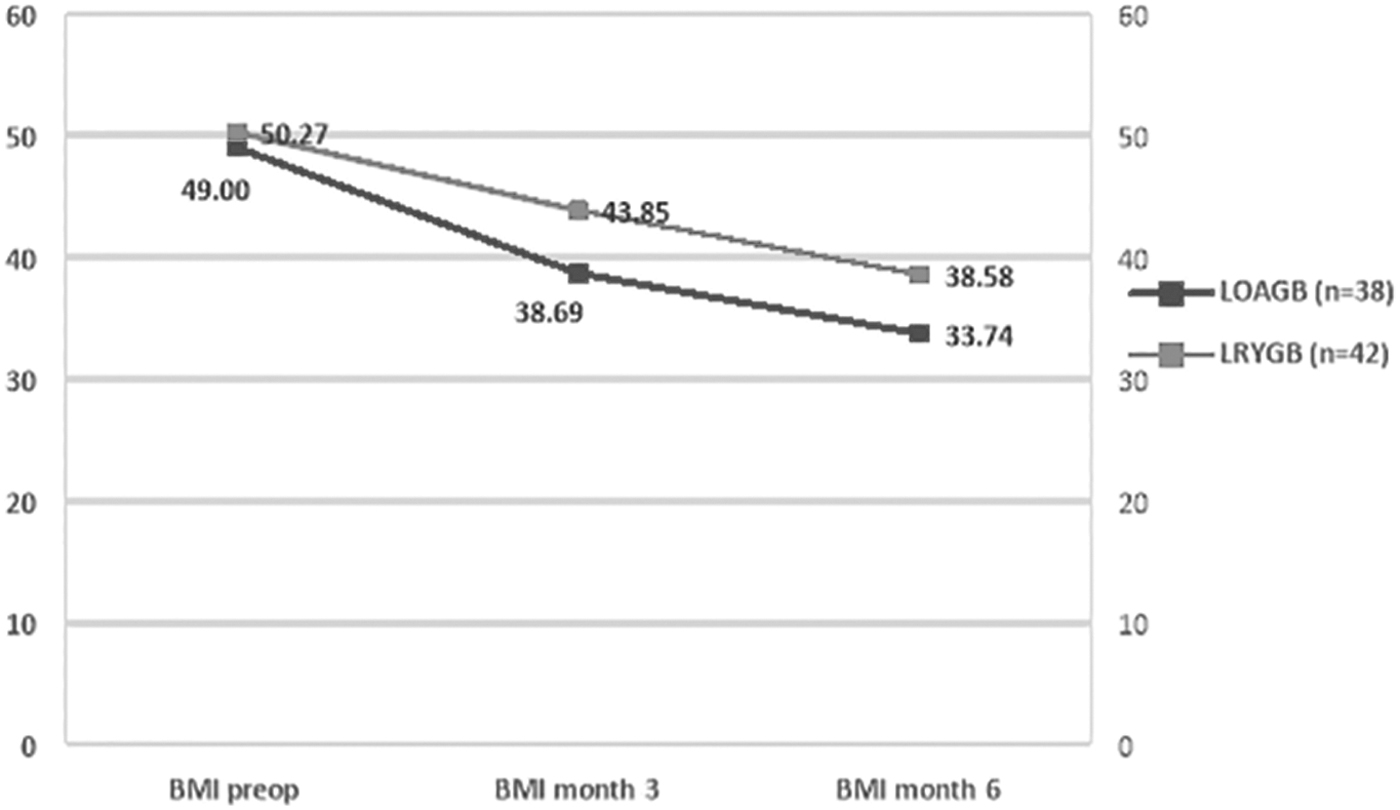
The diagram of the BMI measurements in accordance with the surgical technique. BMI, body mass index.
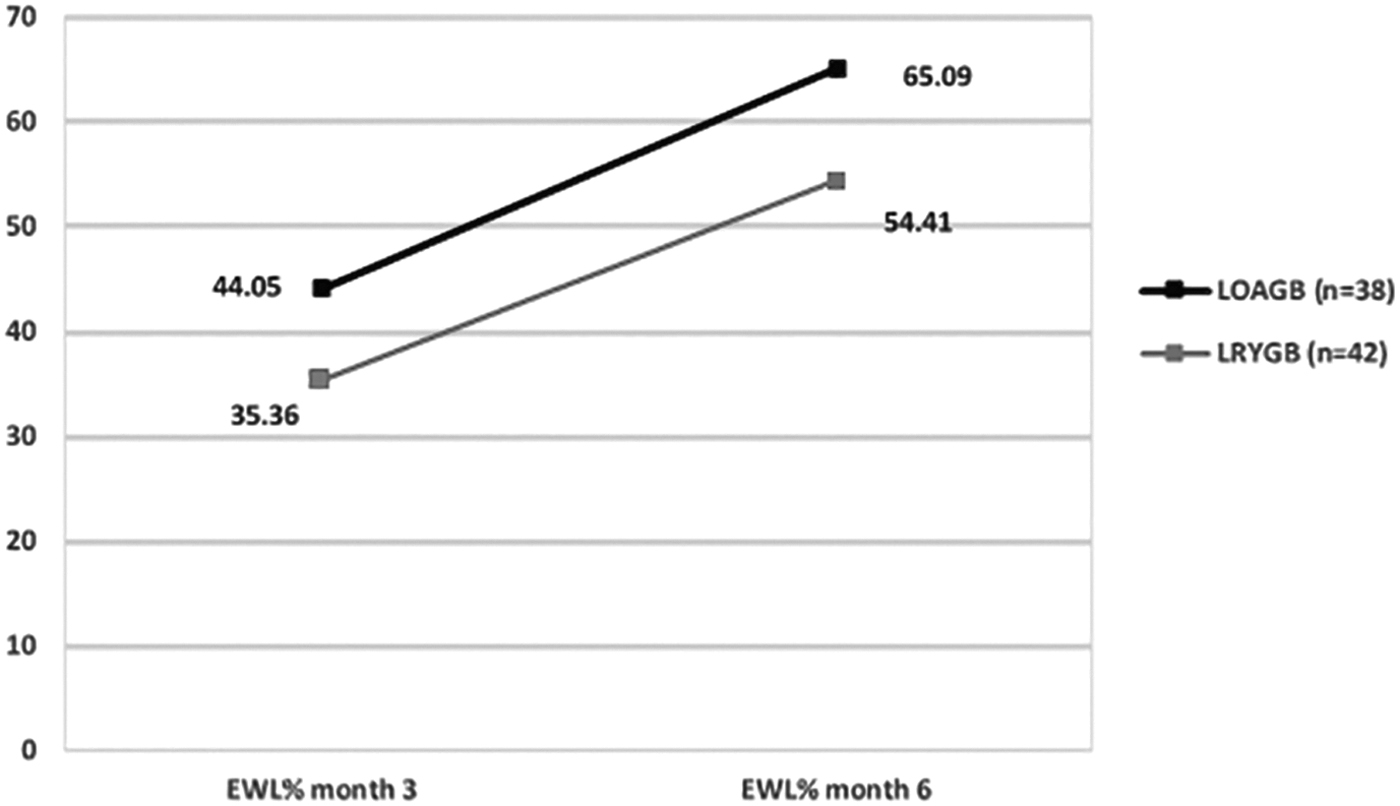
The diagram of the EWL% measurements in accordance with the surgical technique. EWL%, excess weight loss %.
The Comparison of the Parameters at Baseline, 3 Months, and 6 Months After Surgery
Differences between groups (intergroup analysis): *p ≤ 0.005; **p < 0.050; ***p < 0.100.
BMI, body mass index; BP, blood pressure; %EWL, excess weight loss %; FFM, fat free mass; HbA1c, glycosylated hemoglobin A1c; HOMA-IR, homeostasis model of assessment insulin resistance; HDL, high density lipoprotein; LDL, low density lipoprotein; TIBC, total iron binding capacity.
Triglyceride, cholesterol, LDL, and HDL were investigated as the lipid profile in both groups. An improvement was detected in the lipid profiles compared with the levels before surgery in both groups; however, there was no significant difference detected between the groups. Iron, TIBC, vitamin B12, and folate were investigated for the vitamin and mineral deficiency in both groups. The decrease of iron levels in both groups was detected in the third-month controls; however, the decrease was found to be statistically insignificant between the groups. The decrease of TIBC levels in both groups was seen in the third-month controls; however, the decrease was found to be statistically insignificant between the groups. Total protein and albumin levels were investigated for malnutrition in both groups. No statistically significant decrease was detected in the groups.
Conversion to laparotomy was not required in any group. There was no significant difference regarding the hospital stay time of the patients. The surgical complications were similar, and port site hernia was detected in one patient and wound site infection in three patients in LRYGB group; however, wound site infection was detected in two patients in LOAGB group, and there was no major complication. The factor which mostly elongated the hospital stay was the wound site infection. No mortality was detected in any group.
Discussion
In this study, we found improvement in metabolic and clinical results after surgery in both groups. More rapid diabetes regulation was detected, and the decrease in BMI and EWL% was more rapid in Group II.
Although various different methods and techniques have been used in the treatment of obesity, bariatric surgery is considered when the other treatments fail. There is no actually efficient and long-term treatment option of obesity rather than surgery. 9 The effects of the available bariatric procedures are unclear in the comparison with medical management and within themselves. Regardless of the method, obesity surgery promotes more improvement in the weight loss results and weight associated comorbidities compared with the nonsurgical interventions. 10
In parallel with the improvements in the minimal invasive technology, one of the most commonly performed techniques is LRYGB. However, LRYGB is a technically difficult procedure. The technical difficulty is mainly associated with the high anastomosis proximal to the esophagogastric junction. The learning curve is very steep and is associated with longer operative times and higher perioperative complication rates. 11 LOAGB is a comparatively efficient and technically simple surgical procedure. The presence of single anastomosis is the most significant technical convenience.
Most of the studies showed that obesity surgery had a statistically significant effect on weight loss. Lee et al. detected in a prospective randomized controlled study that the EWL% was significantly greater in the LOAGB than in the LRYGB in the first year (64.9% vs. 58.7%, p < 0.05); however, no significant difference was detected in the second year between the groups. 12 In a comparison study of mini-gastric bypass (MGB), RYGB, and SG by Jammu et al., including 1107 patients, EWL was most significantly detected in MGB (92.2%), in RYGB (72.3%), and in SG (53.6%), respectively. 13
In 2019, Robert et al. demonstrated that in their study (YOMEGA), excess BMI loss was at 2 years 85.8% (standard deviation [SD] 23.1) in the RYGB group and 87.9% (SD 23.6) in the OAGB group. They found that OAGB is not inferior to RYGB in terms of percentage excess BMI loss at 2 years. 14 Similar to our study (OAGB to 200 cm biliopancreatic limb [BPL] and RYGB to 70 cm BPL), the YOMEGA study compared OAGB to 200 cm BPL and RYGB to 50 cm BPL. In contrast, Ruiz-Tovar et al. 15 the authors found a significantly higher percentage of BMI loss in the OAGB group at 2-year follow-up compared to the RYGB group (103.4% vs. 87.2%; p < 0.001). In their study, the length of the biliopancreatic limb was longer than in our study, varying from 200 to 350 cm depending on the length of the total bowel by use of the ratio of 60% biliopancreatic limb to 40% common limb. 15
In our study, it was found that LOAGB provided more effective weight loss than LRYGB (p = 0.007 and p = 0.008, respectively). The BMI decreased to 33.7 kg/m2 from 49 in LOAGB group and to 38.5 kg/m2 from 50.2 in LRYGB group in the controls in month 6 (p = 0.003). It is unclear whether the current situation will result in favor of LRYGB as the follow-up period increases. We hope to share our long-term results with the increase in our follow-up period.
Obese patients are expected to have more comorbidities compared with the normal population, and one of the most important comorbidities is diabetes. Many publications are investigating the association of obesity and diabetes and the association of bariatric surgery and diabetes in the literature. Ribaric et al. investigated the observational studies of weight loss and remission of T2DM and bariatric surgery with conventional medical treatment in a meta-analysis. Sixteen studies, including 631 patients, and a mean 17.3 months follow-up were investigated and, accordingly, found the remission rates of type-2 diabetes as 63.5% and 15.6%, respectively, between the surgical and conventional groups (p < 0.001). 16
In the YOMEGA study, the mean decrease in HbA1c at 2 years was significantly greater in the OAGB group than in the RYGB group (−2.3% vs. −1.3%, p = 0.025), and T2DM remission rate after OAGB was 60% higher than the 38% after RYGB. 14 Improvement or recovery was detected in all comorbidities, including T2DM, high BP, and dyslipidemia 6 months after LOAGB procedure in addition to good weight loss results in our study.
Buchwald et al. reported the improvement rates in diabetes as 56.7%, 79.7%, and 95.1%, respectively, with bariatric surgery using adjustable gastric band, RYGB, and biliopancreatic diversion-duodenal switch in their meta-analysis. Complete diabetes remission was observed in 78% of the patients. The lipid profile improved in 70% of the patients. Although the total cholesterol, LDL, and triglyceride decreased, no significant change was reported in HDL. 17 In our study 24 patients (%57) in Group I and 21 patients (%55.2) in Group II had T2DM. All the patients that used antidiabetic medications discontinued medication in both groups after the controls in month 6. However, the decrease in HbA1c in the early period in LOAGB procedure was found to be statistically more significant compared with LRYGB (p = 0.016).
Another of the obesity-related comorbidities is hypertension. In a large study by Jakobsen et al., a total of 1888 patients (51% medical treatment and 49% bariatric surgery) were evaluated comparing medical and surgery in the treatment of obesity-related comorbidity. The prevalences of hypertension, diabetes, and dyslipidemia after treatment start were significantly lower in the surgical group than in the medical group (p < 0.001). 18 Similar to the literature, an improvement was detected in the arterial BP in both groups, and also total cholesterol, triglyceride, and LDL decreased in both groups. However, no statistical difference was found between the groups.
The comparison of the surgery time in the literature showed that OAGB was significantly shorter. 19 Although the LOAGB was shorter, the difference was statistically insignificant in our study. We first started gastric bypass surgery with RYGB technique, and we are more experienced in this surgical technique. We anticipate that we will obtain significantly shorter operating time in LOAGB compared to LRYGB as our experience increases.
Currently, LRYGB is the preferred procedure in the presence of serious metabolic disorders associated with morbid obesity. However, two-stage bariatric strategy (first restrictive and then malabsorbtive) is commonly recommended in the presence of excessive abdominal obesity and/or super obesity due to technical difficulties and due to a highly operative risk. 20 LOAGB procedure, which combines nutritional restriction and malabsorption, may be accepted as a better option for super obese patients aged 55 years and above with severe metabolic syndrome because LOAGB reduces the technical difficulties and promotes a lower risk of surgery compared with LRYGB. Therefore, LOAGB in practice becomes an alternative procedure in high-risk patients for LRYGB and two-stage strategy.
Limitations and strengths
The limitations of the present study were that it was not a prospective randomized controlled study, the number of patients were relatively smaller, the follow-up period was shorter (6 months), and the late complication results were unclear owing to the short follow-up period. However, the study was valuable because the weight loss in both groups was indisputable. In OAGB, the longer small bowel bypass limb is associated with increased malabsorption. 14 Another limitation of this study is that parameters related to steatorrhea and nutritional disorders were not taken into consideration.
In fact, the increased bypass limb of the small intestine is the main cause of weight loss. Weight loss is directly related to remission of T2DM, hypertension, and dyslipidemia.
Conclusions
OAGB is associated with more rapid weight loss and type 2 diabetes remission and also not inferior than RYGB in terms of other metabolic parameters. LOAGB is a relatively new procedure, and there is a lack of long period evaluation. To see the LOAGB as more efficient and reliable compared with LRYGB, randomized clinical studies conducted with high statistical power are required.
Footnotes
Authors' Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by B.G., S.D., N.A., B.F.C., T.B., and U.B. The first draft of the article was written by B.G., and all authors commented on previous versions of the article. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.