
Abstract
Background:
The aim was to assess the long-term impact of laparoscopic sleeve gastrectomy (LSG) on weight loss, postload hypoglycemia, and nutritional status of 25-OH-vitamin D, cyanocobalamin, albumin, creatinine, ferritin, and hemoglobin.
Methods:
A prospective, longitudinal analysis of collected data from 60 sleeve gastrectomy patients was performed on a 5-year follow-up period.
Results:
Therapeutic success rate (excess body mass index loss ≥60%) was 80% at 5 years. The prevalence of postload hypoglycemia increased progressively, reaching a maximum at 1 year (20.3%) and then drop out to 0% at 5 years postoperatively. Glycemic profile and insulin resistance improved significantly from the 1st month postoperatively, remaining stable thereafter, whereas the C peptide had a decreasing trend throughout the study period. Prevalence of nutritional deficiencies at baseline, 1 month, 3 months, 1 year, and 5 years postsurgery were specifically for cyanocobalamin (0%, 3.3%, 15.5%, 27.1%, and 30.0%), vitamin D (21.7%, 48.3%, 63.8%, 76.3%, and 85%), and albumin (0%, 16.7%, 1.7%, 1.7%, and 11.7%, respectively). Ferritin and hemoglobin levels showed a significant drop in the 1st month postoperative and remain stable afterward, whereas creatinine decreased significantly after the 1st year postoperative in comparison with preoperative.
Conclusions:
LSG was effective in terms of weight loss, insulin sensitivity, and glycemic profile improvement, but with the risk of nutritional deficiencies and postload hypoglycemia.
Introduction
The prevalence and incidence of obesity are increasing worldwide, particularly in developing countries, despite its recognition as major risk factor for cardiovascular diseases and diabetes.1–3 Obesity is one of the most frequent metabolic diseases, with an estimated prevalence of 32.4% in the United States, 16.7% in Europe, and 31.9% in Romanian adult population.1,2,4
Nowadays bariatric surgery is considered an effective long-term therapeutic option for obesity and its comorbidities, inducing a sustained weight loss of 20–30% over a period of 15–20 years. 5
Laparoscopic sleeve gastrectomy (LSG), as a restrictive procedure, has been proved to be effective in treating weight excess and diabetes through a significant effect on energy intake and carbohydrate metabolism.6,7 However, at present, there are few data regarding glycemic profile during oral glucose tolerance test (OGTT) and postload hypoglycemia risk after LSG. Postbariatric hypoglycemia is increasingly encountered, but the true prevalence of this condition remains uncertain, owing to differences in the diagnostic criteria and also to relative lack of patient awareness of hypoglycemic risk and symptoms.
Given the effectiveness of LSG in inducing significant weight loss, there is a potential risk of nutrients deficiencies and protein malnutrition, despite routine supplementation of micronutrients.8,9 However, LSG as a purely restrictive procedure tends to induce micronutrient deficiencies less significantly than malabsorptive interventions.8,10,11 The most common deficiencies associated with LSG were cyanocobalamin, 25-OH-vitamin D, ferritin, and albumin, but the mechanisms by which these deficiencies are induced are incompletely elucidated.8,9,11
The psychological impact of bariatric surgery, decreased food intake, reduced gastric volume, and changing the secretory profile of mediators involved in regulating appetite and satiety are potential factors that explain at least in part the postload hypoglycemia and nutritional deficiencies attributed to bariatric surgery.
Current knowledge of nutritional deficiencies (water and fat-soluble vitamins, essential minerals, and albumin) secondary to bariatric surgery does not provide enough data to establish the micronutrients requirement and to prevent hypoglycemia in patients undergoing bariatric surgery.
The aim of this study was to assess the medium and long-term clinical outcomes of LSG in terms of OGTT glycemic profile, postload hypoglycemia, nutritional status, and deficiencies in albumin, cyanocobalamin, and 25-OH-vitamin D.
Materials and Methods
A prospective, longitudinal study assessing the efficacy and nutritional deficiencies related to LSG was carried out between 2009 and 2014 in the “N.C. Paulescu” National Institute of Diabetes, Nutrition and Metabolic Diseases Bucharest and in the Clinical Hospital “Euroclinic—Regina Maria” Bucharest. The study was performed according to World Medical Association Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Participants and was approved by the Ethics Committee of University of Medicine and Pharmacy “Carol Davila” Bucharest (No. 199/2009). The care team of patients who underwent bariatric surgery included a surgeon, a specialist in nutrition and metabolism diseases, a dietitian, a psychologist, and physiotherapist.
Patients meting the standard criteria 12 for LSG in 2009 were enrolled based on the inclusion/exclusion criteria described elsewhere. 13 Informed consent was signed by all subjects included in the study. Patients were assigned to a standardized follow-up program (including evaluation of clinical and biological data and completion of a standardized questionnaire applicable to all patients undergoing bariatric surgery), being consequently evaluated preoperative and at 1 month, 3 months, 1 year, and 5 years postoperatively in terms of therapeutic success (percentage of excess body mass index lost [%EBMIL] ≥60%), glycemic profile during OGTT, insulin resistance and insulin secretion, and nutrient status. Baseline and at each study visit, a questionnaire was completed with information on lifestyle elements (diet—frequency of main food groups consumption, frequency of snacks, physical activity, consumption of alcohol, smoking); administration of anxiolytics, antidepressants, sleeping pills, drugs, analgesics; eating disorders (bulimia, anorexia); use of laxatives, diuretics, enemas for weight loss; the psychological impact of the excess weight and also of the weight loss after the surgery.
%EBMIL was calculated as follows: (preoperative body mass index [BMI] – postoperative BMI)/(preoperative BMI – 25) × 100. 14
OGTT using 75 g anhydrous glucose was performed in all participants, with simultaneous determination of fasting concentration of C-peptide, insulin and plasma glucose, and afterward only glycemia was measured at 30 min, 1 h, and 2 h after glucose ingestion. In patients with preexistent type 2 diabetes mellitus (T2DM), OGTT was performed in conditions of 24 h discontinuation of antidiabetic therapy. Impaired glucose regulation categories were diagnosed according to 2019 American Diabetes Association guidelines. 15
Insulin resistance was estimated by Homoeostasis Model Assessment-Insulin Resistance (HOMA-IR), calculated using the equation: fasting insulinemia (lU/mL) × fasting glycemia (mg/dL)/405. 16
Postload hypoglycemia was defined as 2-h OGTT glycemia ≤60 mg/dL. The ratios of baseline to 1-h and 1- to 2-h OGTT glycemia were calculated to estimate the slope or degree of rise and down of glucose during OGTT. These ratios were calculated preoperative and in all time point of study evaluation.
Muscle and fat mass were evaluated by bioelectrical impedance method (OMRON brand, model 508—Body Composition Monitors).
To evaluate preoperative nutrient status and the postoperative nutritional deficiencies, the fasting serum levels of vitamin B12, 25-OH-vitamin D, creatinine, albumin, ferritin, and hemoglobin were assessed.
Surgical technique
Laparoscopic gastric sleeve was the surgical procedure applied in this study. The surgical technique involved resecting the gastric fundus and the large curvature of the stomach, by sectioning from the lateral extremity of the antrum (4–6 cm proximal to the pylorus) to the Hiss angle, using the successive application of linear staplers. The remnant gastric volume was ∼100 mL.
Statistical analysis
The general linear model analysis for repeated measures (analysis of variance) and Cochran's test were used to test the differences of analyzed continuous and categorical variables at each postoperative time point from baseline and from the previous one.
Spearman's correlation analysis was performed to identify the cross-sectional relationships between %EBMIL and variables of interest. The data were analyzed using SPSS software version 19.0 and p ≤ 0.05 (two-tailed) was considered significant.
Results
The study included 68 participants, of whom 8 subjects were lost to follow-up or had incomplete data.
This study enrolled 60 subjects with a mean BMI of 44.6 ± 9.9 kg/m2 (83.3% women, 41.7 ± 12.5 years) who underwent LSG.
The proportion of subjects who achieved therapeutic success (%EBMIL ≥60%), increased statistically significant at 1 year postoperatively, then increased steadily in the next 4 years of study, reaching 80% at 5 years after the LSG (Table 1).
The Evolution of Therapeutic Success, Hypoglycemia and Nutritional Markers
Categorical variables are expressed as percent and continuous variables are expressed as mean ± standard deviation.
p < 0.05: *1 month, 3 months, 1 year, 5 years versus baseline; †3 months, 1 year, 5 years versus 1 month; ‡1 year, 5 years versus 3 months; §5 years versus 1 year.
BMI, body mass index; EBMIL, excess body mass index loss; HOMA-IR, Homoeostasis Model Assessment-Insulin Resistance; OGTT, oral glucose tolerance test.
Preoperatively, 36.7% subjects had T2DM (diabetes duration 5.8 ± 4.0 years) and 10% of participants had prediabetes. Regarding antidiabetic treatment, of the 22 patients with T2DM, 9.1% were only on lifestyle optimization, the majority (59.1%) had monotherapy with metformin, 18.2% had double therapy with noninsulin antidiabetic drugs, 13.6% had metformin associated with basal insulin, and no patient with T2DM had insulin alone. After the first postoperative year, all patients with T2DM were only on lifestyle optimization or metformin monotherapy.
Glycemic profile
Dynamic changes in glycemic profile are given in Table 1 and Figures 1 and 2.
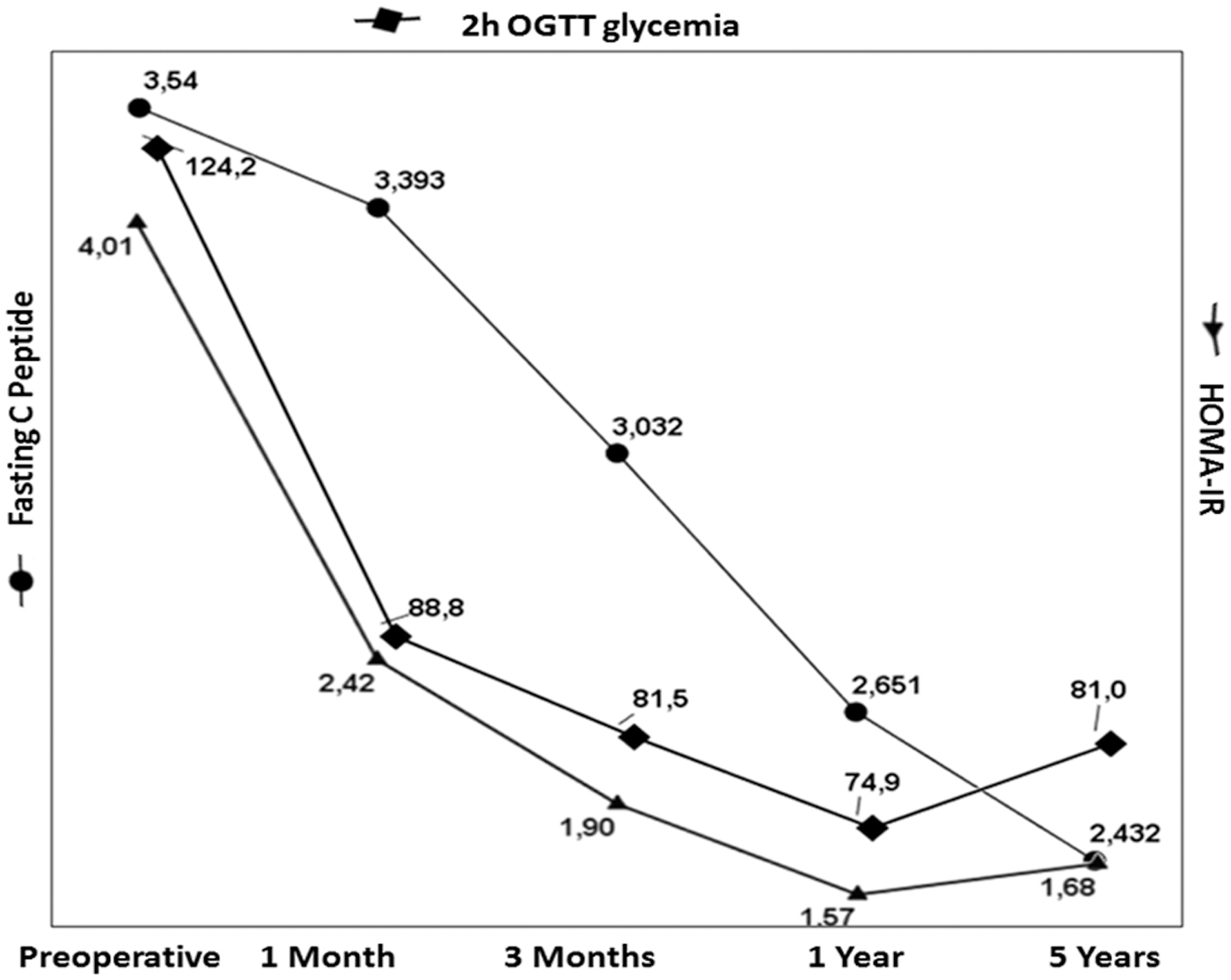
The dynamics in the changes of 2-h OGTT, HOMA-IR, and fasting C peptide levels (estimated marginal means). EBMIL, excess body mass index loss; HOMA-IR, Homoeostasis Model Assessment-Insulin Resistance; OGTT, oral glucose tolerance test.
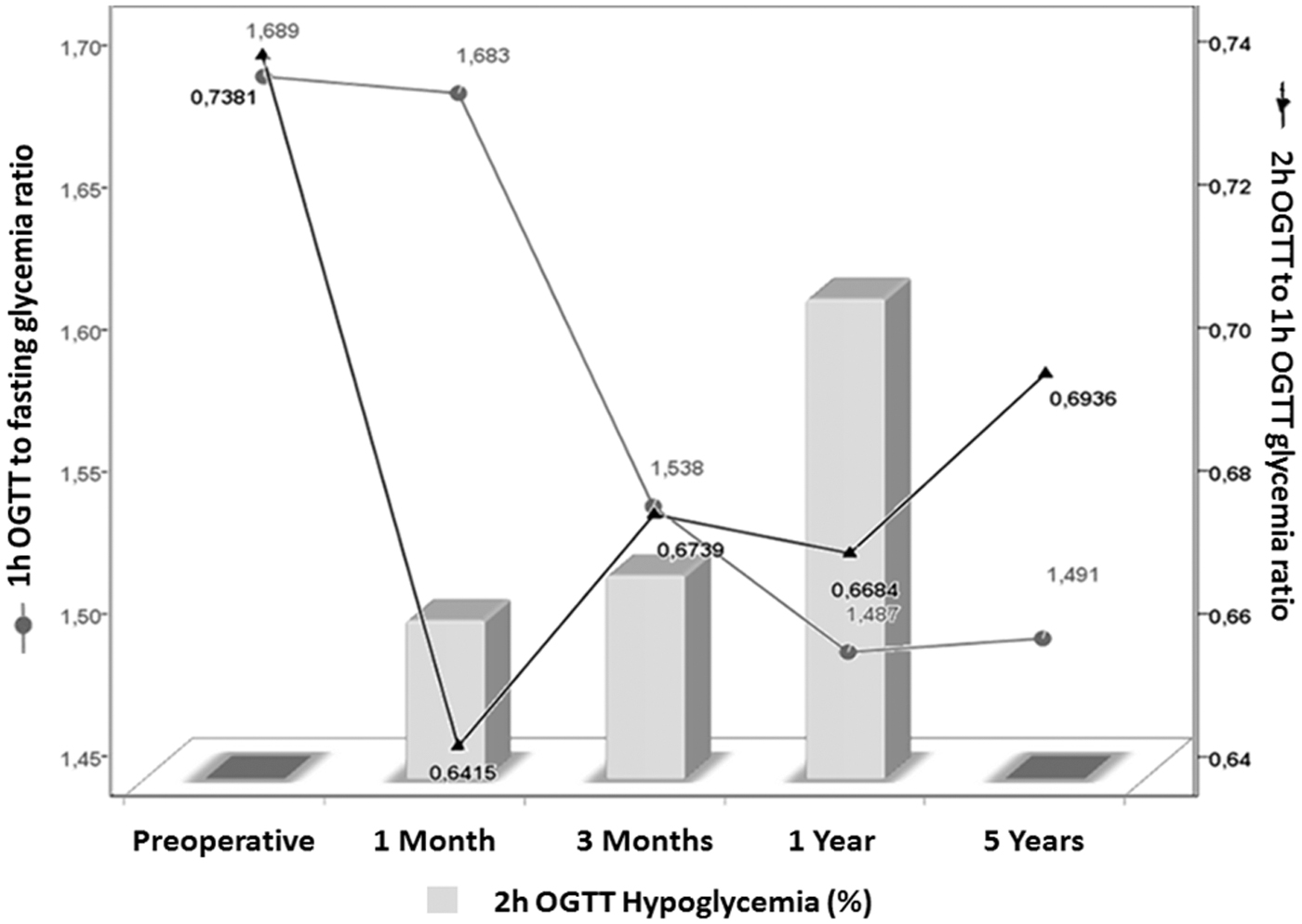
The dynamics in the changes of 2-h OGTT to 1-h OGTT glycemia ratio, 1-h OGTT to fasting glycemia ratio (estimated marginal means) and in the percentage of subjects with 2-h OGTT hypoglycemia.
Improvement of the OGTT glycemic profile in the 1st month after bariatric surgery is the most important, especially in terms of glycemia at 2 h during OGTT and is recorded in parallel with significant decreases in HOMA-IR (Table 1; Fig. 1).
After the 1st year we observed a slight increase, without statistical significance, in the glycemic values at all the time points of OGTT, especially for 2-h OGTT glycemia, and HOMA-IR (Table 1; Fig. 1).
The fasting C peptide levels significantly decreased during the 1st month postoperative, the downward trend continuing during the 1st year follow-up. Late postoperatively, we identified a significant decrease in the fasting C peptide levels (Table 1; Fig. 1).
The 1-h OGTT to fasting glycemia ratio decreased progressively in the 1st year after LSG, whereas 2-h OGTT to 1-h OGTT glycemia ratio, after significant decrease in the 1st month, remained stable in the 1st year postoperatively (Table 1). After the 1st year we observed a slight increase, without statistical significance, in the 1-h OGTT to fasting glycemia ratio and 2-h OGTT to 1-h OGTT glycemia ratio (Table 1).
According to the results presented in Table 1, LSG induced high risk for hypoglycemia at 2-h during OGTT at 1 year after bariatric surgery, 20.3% of patients having glycemia lower than 60 mg/dL at 2-h after glucose administration. The frequency of 2-h OGTT hypoglycemia decreased significantly after the first postoperative year (Table 1; Fig. 2).
The presence of 2-h OGTT hypoglycemia at 1 month, 3 months, and 1 year postoperatively did not correlate with the preoperative presence of T2DM or prediabetes. All patients with 2-h OGTT hypoglycemia at 1 month postsurgery had normal glucose tolerance. Of the patients with 2-h OGTT hypoglycemia at 3 months postoperatively, only one patient had preoperative prediabetes and no patient had T2DM. Of the 12 patients with hypoglycemia at 1 year postoperatively, before bariatric surgery, 2 had prediabetes and 7 had T2DM of which only one was on therapy with metformin and basal insulin, but at 1 year postoperatively insulin therapy was stopped, remaining only on metformin. The rest of the patients with T2DM and hypoglycemia at 1 year were preoperatively on lifestyle optimization ± metformin. T2DM remission, defined according to Buchwald criteria, 17 was recorded in 5 of the 7 patients with T2DM and 2-h OGTT hypoglycemia at 1 year postoperatively.
Nutritional deficiencies
The mean vitamin B12 and vitamin D levels decreased significantly from the first postoperative month; however, after the 1st year the downward trend of vitamin B12 and vitamin D levels was not statistically significant (Table 1). The frequency of hypovitaminosis B12 increased progressively from 0% in the preoperative period to 27.1% and 30% at 1 year and 5 years, respectively, postoperatively (Table 1; Fig. 3).
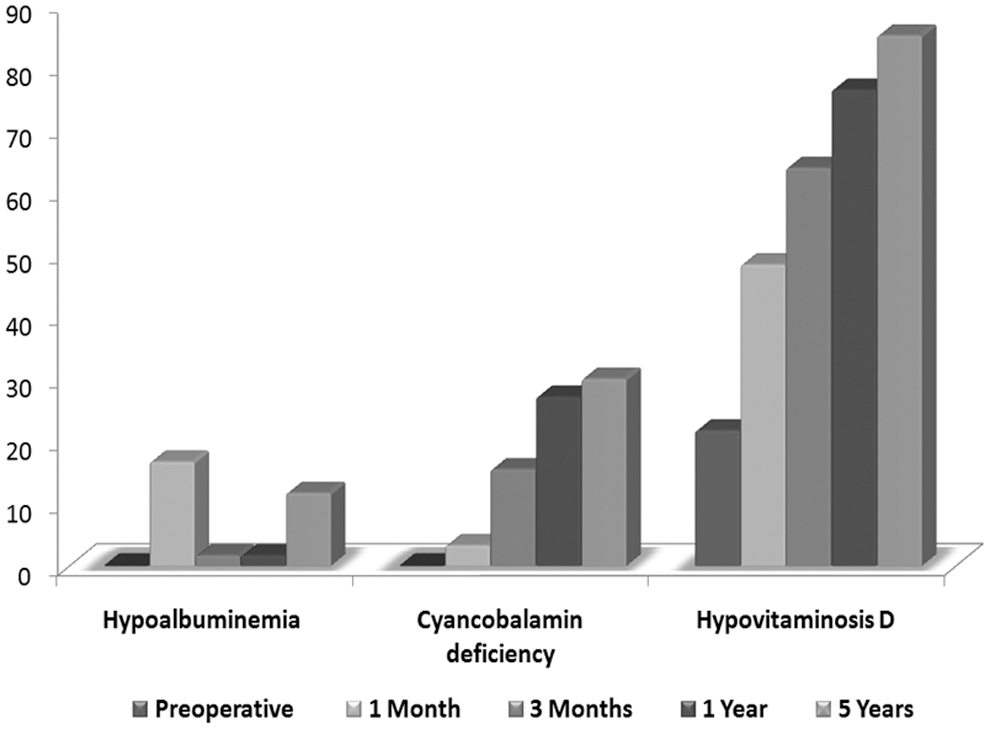
The dynamics in the changes of percentage of subjects with different nutritional deficiency.
The proportion of subjects with low levels of vitamin D increases significantly early postoperatively; after the 1st month, however, the upward trend was not statistically significant (Table 1; Fig. 3). The status of vitamin D had an inverse trend compared with the evolution of the proportion of adipose tissue during the entire follow-up period (Table 1).
The mean serum creatinine level did not change significantly in the first 3 months postoperatively, but thereafter there was a significant decreasing trend in creatinine levels, despite a significant increase in muscle mass in dynamics (Table 1).
The levels of albumin, ferritin, and hemoglobin decreased significantly in the 1st month postoperatively, had a slight upward trend in the next 2 months, remaining stable thereafter throughout the study period (Table 1).
The frequency of hypoalbuminemia increased significantly in the 1st month, after which the percentage of patients with hypoalbuminemia decreased in the first postoperative year. In the next 4 years of follow-up, there was a significant increase in the frequency of hypoalbuminemia (Table 1; Fig. 3).
We found significant association of HOMA-IR at all time points and %EBMIL at the same assessment point (p = 0.048 at 1 month, p = 0.003 at 3 months, p = 0.001 at 1 year, and p = 0.022 at 5 years) as well as between fasting C peptide level at 1 month (p = 0.026) and 3 months (p = 0.004) follow-up and %EBMIL at the same time points. Throughout the 5 years of follow-up, there were no significant correlations between %EBMIL and preoperative levels of all nutritional markers. The levels of ferritin at 1 month (p = 0.032) and 3 months (p = 0.048) were negatively correlated with %EBMIL evaluated at the same time point.
Discussion
Our study indicates that LSG provides effective weight loss, reduces insulin resistance, improves glucose tolerance, and lowers fasting C peptide levels, and also that the improvement of insulin sensitivity and OGTT glycemic profile was registered from the 1st month postoperatively, even before the weight loss became significant.
Significant improvement in insulin sensitivity in the first postoperative month associated with a secondary decrease in insulin secretion may justify the significant improvement in glycemic profile during OGTT, especially 2-h glycemia. After the first postoperative year, although %EBMIL continues to increase, insulin resistance begins to increase and peptide C continues to decrease and thus glycemic levels increase during OGTT, especially 2-h glycemia. This suggests that the improvement of glucose tolerance is not the result of enhanced insulin production, as in Roux-en-Y gastric bypass, but perhaps a sharp reduction of insulin resistance. 18
Up to now, only a few studies have investigated postload hypoglycemia after LSG, and the reported prevalence of hypoglycemia are conflicting owing to differences in the diagnostic criteria. However, the frequency of postload hypoglycemia observed in our study was comparative with the overall frequency of hypoglycemia after LSG reported by Brix et al. 19
The high frequency of 2-h OGTT hypoglycemia at 1 year postoperatively may be explained by the evolution of insulin resistance and insulin secretion in the 1st year, but also by the slope of glucose during OGTT at 1 year postoperatively, characterized by the lowest glucose peak at 30 min, followed by a significant decrease in blood glucose at 2 h.
Given that after the first postoperative year, metformin was the only antidiabetic therapy in diabetic patients, postload hypoglycemia may not be secondary to antidiabetic therapy, but rather is a consequence of improving insulin sensitivity, possibly dumping syndrome or postoperative dietary restrictions.18,20
In our study, mean vitamin B12 concentration decreased progressively during the 5 years of follow-up, 30.0% of the participants having cyanocobalamin deficiency. These data are consistent with other LSG studies that reported a prevalence of vitamin B12 deficiency varying between 12.5% and 28.6%.21–24
Vitamin B12 deficiency after LSG could be primarily attributed to malabsorption owing to intrinsic factor reduction after fundus resection, and also to food choices or insufficient dose of vitamin B12 in the prescribed supplements. 24
Of interest, we observed a postoperative increase in vitamin D deficiency, despite the significant reduction of fat mass. These findings are supported by Ben-Porat et al. and may be explained by the low adherence to vitamin D supplementation or to returning to poor food choices in the long-term post-LSG. 25 Unlike our study, several studies reported improvement in vitamin D levels over long-term follow-up, and also a significant inverse correlation between vitamin D levels and weight loss.21,26–28
In our study the albumin levels significantly decreased in the 1st month postoperatively probably secondary to reduced protein intake, but, given the fact that albumin is a negative acute phase protein, hypoalbuminemia might also indicate an early postoperatively increased inflammatory status. 29 The prevalence of hypoalbuminemia increased significantly late postoperatively, our results being in line with previous findings.26,30 In addition, as an indicator of protein deficiency, creatinine levels decrease significantly late postoperatively, despite increase in the muscular mass.
Our results indicated that levels of ferritin and hemoglobin decreased over time, similar to previous reported data.22,23,28,31,32 The significant decrease in ferritin and hemoglobin levels in the 1st month postoperatively may be justified by bleeding associated with surgery. Subsequently, restricted dietary iron intake or iron malabsorption owing to a reduced secretion of hydrochloric acid may justify low ferritin levels after the first postoperative year.32,33
To our knowledge, this study is the first long-term prospective study assessing the impact of LSG on postload hypoglycemia and nutritional deficiencies in Romanian patients.
Concerning limitations, our study was performed on a small sample size given the fact that only patients with complete data in all the follow-up time points were enrolled and also that LSG was the only analyzed surgical method. Another limitation of this study is that the data regarding compliance to supplement intake and dietary consumption had not been assessed, a good compliance being assumed.
Conclusions
LSG proved to have beneficial effects in Romanian patients, in terms of weight loss, insulin sensitivity, and glycemic profile improvement, evident from the 1st month after surgery. Despite these favorable effects of surgery, there were significant nutritional deficiencies in the first postoperative year, especially in terms of vitamin B12 and vitamin D and an increased frequency of hypoglycemia. These effects have decreased over the next 4-year postoperative follow-up. These data suggest that, although the benefits of bariatric surgery exist beyond absolute weight loss, correctly establishing the timing and opportunity of bariatric surgery may be an important predictor of therapeutic success. Further studies are needed to examine the question of whether standardized measurements of nutrient blood levels are adequate determinants of clinically relevant nutritional deficiencies. Furthermore, the optimal dosage and the optimal duration of specific supplementation in the bariatric patient should be determinate for adequate treatment of nutrient deficiencies.
Footnotes
Authors' Contributions
All authors had equal contribution to conception and design, analysis and interpretation of data, drafting the article or revising it critically for important intellectual content and final approval of the version to be published.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work had no funding source.