
Abstract
Background:
More than 250,000 laparoscopic sleeve gastrectomy (LSG) are performed annually accounting for about 61.4% of all bariatric procedures. The national average cost for LSG ranges between $15,000 and 33,000 with an estimated economic impact of $7.5 billion yearly in the United States alone, expenditures are likely to continue increasing steadily. LSG has already emerged as the preferred surgical choice for obesity.
Materials and Methods:
Retrospective review of 198 patients who underwent LSG. Among the several clinical parameters collected, the pertinent ones were length of stay (LOS) after LSG, operative time, anesthesia time, complications, readmissions, radiation exposure, economic impact between those who underwent intraoperative esophagogastroduodenoscopy (IEGD) and postoperative upper gastrointestinal series (PUGI).
Results:
LOS was significantly different with mean difference of 1.835 ± 0.8645 days (confidence interval [95% CI]: 0.1298–3.540) and p-value of 0.0351, mean LOS in IEGD was 1.088 and PUGI 2.923 days. Time to initiation of diet—mean difference 16.50 ± 0.9250 h (95% CI: 14.68–18.33), p-value of <0.0001. Radiation exposure in IEGD was nil, whereas in PUGI Fluro time was 6–78 s, mean time 26.73 s, standard deviation 19.69. Procedural and anesthesia times with a mean of 66.05 min and 109.7 min respectively, and p-value of 0.0174 and 0.0182 both being significantly different. There was no statistical significance between the groups for complications, emergency department visits, and readmissions.
Conclusions:
Our study clearly illustrates that IEGD is superior to PUGI on several parameters. This translates into increased efficiency, reduced economic burden, decreased hospital LOS, radiation exposure, and increased overall patient satisfaction.
Introduction
Bariatric surgery has emerged to curtail and negate the detrimental consequences of obesity and its comorbidities. In the past two decades several basic science and clinical research in this field had shed light into deeper understanding of the homeostatic alterations rendered by various individual bariatric surgeries. Obesity in itself casts a huge economic burden of >$215 billion annually in addition to its health effects and comorbidities in the United States alone. 1
There has been a drastic change in the bariatric procedure of choice in the past decade alone. In 2011 36.7% of Roux-en-Y gastric bypass (RYBG), 35.4% gastric band (GB), and 17.8% sleeve gastrectomy (SG) were performed among all bariatric procedures in the United States, whereas in 2018 only 17% of RYBG, 1.1% of GB, and a whopping 61.4% of SG were performed. 2 This clearly depicts the transition in the emerging procedure of choice backed by strong research. Although laparoscopic sleeve gastrectomy (LSG) is widely practiced across the globe and more so in the United States, it is important to note that there are several protocols that are usually established on an international, national, locoregional, and institutional basis. 3 These protocols span over patient selection, preoperative workup, intraoperative management, and postoperative follow through. Several institutions perform a postoperative upper gastrointestinal series (PUGI), computed tomography (CT) scan, intraoperative esophagogastroduodenoscopy (IEGD), methylene blue leak to test the integrity of the stapled gastric sleeve on a routine or selective basis. 4 We set to assess and compare IEGD against PUGI over several parameters as it has never been done before in our search of literature to provide guidance to those seeking.
Materials and Methods
Study design
Ethical approval from the hospital Institutional Review Board (IRB) for Health Sciences Research was sought and approved. This retrospective study entails data collection of all bariatric patients who underwent LSG from 2019 to early 2020 that met National Institutes of Health criteria for bariatric surgery.
Data collection
Further review using the electronic medical record (EMR) was undertaken to obtain the parameters included in this study namely diagnosis, age, gender, ethnicity, body mass index (BMI), procedure time, anesthesia time, IEGD findings, PUGI findings, hospital length of stay (LOS), complications, readmissions, costs associated with care.
Inclusion and exclusion criteria
Included 197/198 patients who underwent LSG between 2019 and early 2020.
Excluded 1/198 patients. Missing EMR parameters.
Statistical analysis/methods
Baseline characteristics of all patients who underwent bariatric surgery included in our study were described in detail, gross numbers with percentages calculated and used. We summarized the continuous variables using mean and standard deviation (SD), whereas categorical variables were summarized using counts and percentages. Sensitivity, specificity, predictive values, and comparison of diagnostic tests were accomplished using Fisher's exact test. Subgroup analyses were performed using two-tailed chi-square test. p-Value <0.05 was considered statistically significant. Microsoft Excel spreadsheet was used to display extrapolated data. GraphPad Prism 8 (GraphPad Software, La Jolla, CA) was used for statistical analysis.
Results
Patient characteristics
Total number of patients included in the study was 197 of the total 198 as detailed in the inclusion/exclusion criteria of the methods section. All of our patients underwent LSG that was performed by 2 surgeons, 113 by Surgeon A (57.36%) and 84 by Surgeon B (42.64%). Patient's age ranged from 19 to 76 years with a mean of 39.56 and SD 11.21, there were 34 males (17.26%), 163 females (82.74%), BMI ranged between 32.42 and 79.78 kg/m2, mean 43.61, SD 7.67, of which 2 belonged to Class I (1.02%), 61 in Class II (30.96%), 134 in Class III (68.02%), ethnic distributions included 160 Hispanics (81.22%), 34 African Americans (17.29%), 3 Caucasians (1.52%) as depicted in Table 1.
Patient Characteristics Among Intraoperative Esophagogastroduodenoscopy and Postoperative Upper Gastrointestinal Series
BMI, body mass index; EGD, esophagogastroduodenoscopy; HH, hiatal hernia; IEGD, intraoperative esophagogastroduodenoscopy; PUGI, postoperative upper gastrointestinal series; UGI, upper gastrointestinal series.
IEGD versus PUGI clinical parameters
Every patient who underwent LSG had either IEGD or PUGI performed to detect the integrity of the stapled gastric sleeve. We compared several parameters across all patients belonging to both groups as detailed hereunder (Table 2 and Figure 1).
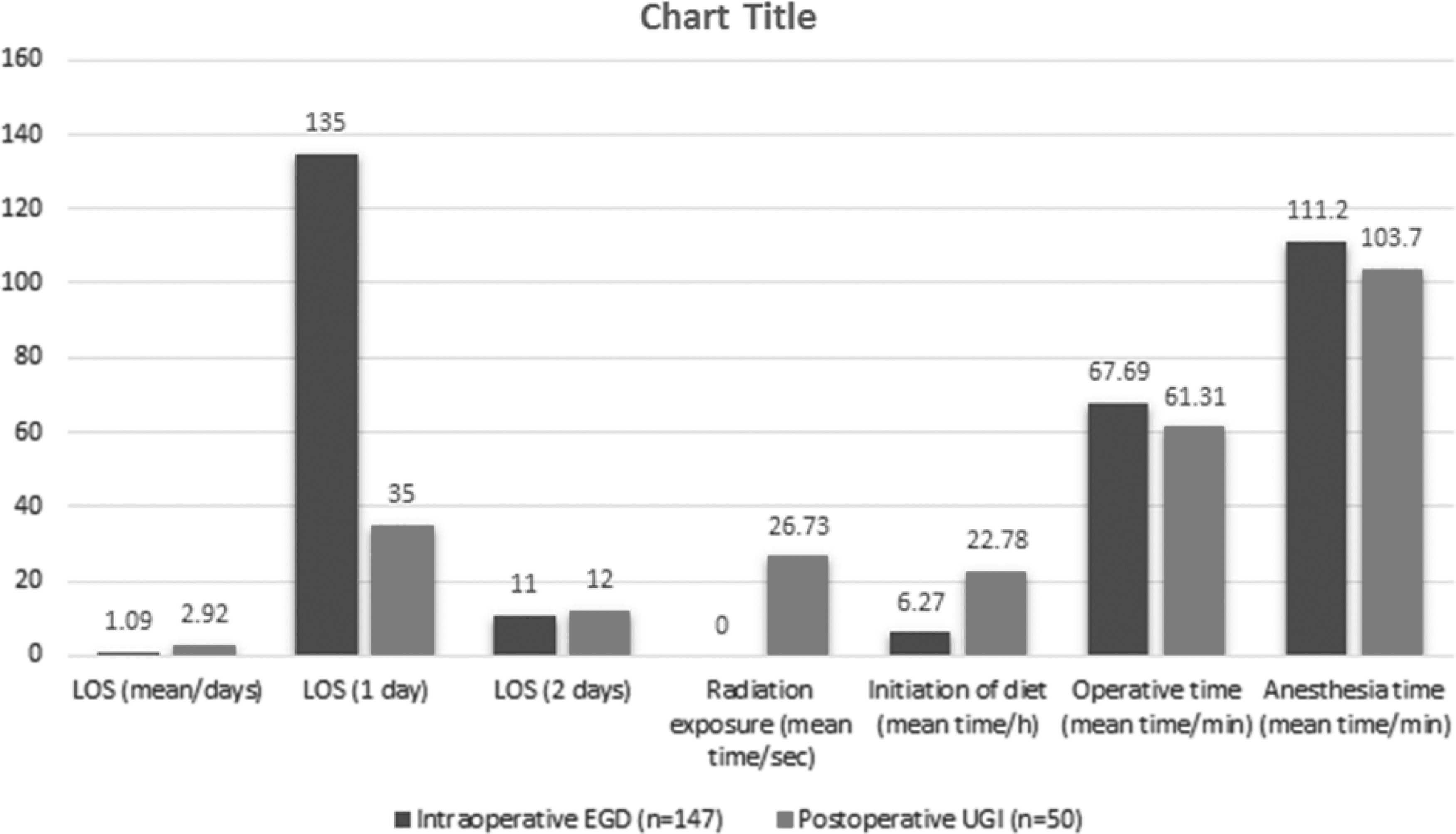
Intraoperative EGD versus postoperative UGI clinical parameters. EGD, esophagogastroduodenoscopy; LOS, length of stay; UGI, upper gastrointestinal series.
Outcomes Among Intraoperative Esophagogastroduodenoscopy and Postoperative Upper Gastrointestinal Series
ED, emergency department; LOS, length of stay;
Length of stay
91.84% of patients in IEGD were discharged within 24 h and their LOS was 1 day, 7.48% in 2 days, and 0.68% in >3 days, whereas in contrast only 70.59% patients of PUGI group stayed for 1 day, 23.53% for 2 days, and 5.88% for >3 days. The overall difference between the groups was statistically significant with mean difference of 1.835 ± 0.8645 days (confidence interval [95% CI]: 0.1298–3.540) and p-value of 0.0351. The delayed hospital stay was directly attributable to the time the test was made available and the initiation of oral diet as per bariatric pathway for LSG in most circumstances.
Radiation exposure
Radiation exposure occurred only to patients belonging to the PUGI group and none of the patients in IEGD. The minimum fluoroscopy time was 6 s to a maximum of 78 s. The mean exposure time was 26.73 s and SD of 19.69.
Initiation of diet
Patients belonging to IEGD grouped had their bariatric stage I diet initiated at or before 6 h postoperative on average, whereas the patients belonging to PUGI group had their diet started at or before 23.84 h on an average, ranging from 20 to 76 h. When both groups were compared, there was significant difference with a p-value of <0.0001.
The mean difference was 16.50 ± 0.9250 h (95% CI: 14.68–18.33).
Complications
Only 2 of our 197 (1.01%) patients had complications; 1 patient with blood loss anemia with dropping hematocrit (Hct) and the other with perisplenic collection and abdominal pain, they belonged to IEGD and PUGI group, respectively. Both patients were managed conservatively and subsequently discharged upon adequate response.
Readmission
There were a total of five readmissions within 30 days of their index surgery accounting to 2.54% of the total. All of them belonged to the IEGD group. The reasons for their readmissions were pulmonary embolism in one patient, oral intolerance with acute pancreatitis in another and oral intolerance with nausea and vomiting in the rest. All of them were successfully managed and subsequently discharged. We do not believe it is related to the choice of leak test and hence consider unrelated and nonsignificant.
Emergency department visit postoperatively
We also looked at the emergency department visits within 30 days from the index admission among all patients belonging to both groups. A total of 19 patients (9.64%) of the total with 16 (10.88%) from IEGD and 3 (5.88%) from PUGI. The reasons for their visits were predominantly nausea, abdominal pain, and some unrelated reasons to the surgery. There is no significance and the p-value is 0.2830 and not significant. We believe they cannot be attributable to any particular clinical parameters in this study as well.
Operative and anesthesia time
We also calculated the operative time as well anesthesia times to see if there is a difference between IEGD versus PUGI. In the IEGD group the operative times ranged from 33 to 133 min, mean 66.05 min, SD 16.56 min, and anesthesia times ranged from 62 to 178 min, mean 109.7 min, and SD 21.06 min. We then compared the groups to determine if there was a difference in the procedural and/or anesthesia times, upon comparison there was significant difference between the groups in both times as follows: procedural time p-value 0.0174 with a mean difference of 6.380 ± 2.660 min (95% CI: 11.63–1.1.34), anesthesia time p-value 0.0182 with a mean difference of 8.099 ± 3.4 min (95% CI: 14.81–1.392).
IEGD versus PUGI economic parameters—considering the national average, state specific, and individualized reimbursement criteria versus a package, LSG is reimbursed at $1175, cost of a single day admission is $2152, PUGI at $166.23, cost of IEGD is usually not reimbursed as it is part of the operative procedure. Average total cost in the IEGD group is $3327 and the PUGI is $7797.23 considering that the mean LOS in IEGD being 1.088 and PUGI 2.923 without and with upper gastrointestinal (UGI), respectively. This amounts to a 134.36% increase in the total costs in the PUGI group compared with IEGD on an average.
Discussion
In the modern era, obesity has become the leading cause of morbidity and is attributable to several chronic noninfectious health care-related disorders affecting more than third of the world's population. 5 The prevalence of obesity in the United States has seen a sharp surge from 30.5% in 1999–2000 to 42.4% in 2017–2018, 6 this results in a huge economic constraint and health care costs >$215 billion annually. 7 As detailed in our introduction LSG has become the procedure of choice to combat obesity and its associated diseases. Several protocols across the United States exist for LSG. Institutions perform routine leak test or selective leak test based on their institutional practicing guidelines, among those who perform routine leak test, the most widely performed test is PUGI, contrast CT scan, intraoperative air test, dye, and EGD.
Although the American Society for Metabolic and Bariatric Surgery has made it clear that there is no current evidence to suggest one test over the other based on the available literature, they do comment that it is acceptable for the surgeon or institution to have their own guidelines. Although UGI contrast study might have low sensitivity and accuracy, which might be subjected to variation and poor interpretation based on varied factors, 8 it is still being widely performed in many centers. UGI also subjects the patient to be exposed to radiation and the subjective additional test postoperatively resulting in patient discomfort and anxiety apart from the delay in initiation of diet.
A viable alternative is to perform an intraoperative test for the integrity of the stapled gastric sleeve. Some authors perform air tests, whereas others prefer methylene blue or IEGD. Whereas air test and methylene blue can indicate leaks, IEGD not only detects leaks, it can assess the integrity of the stapled anastomosis, identify bleeders and treat as necessary, it can also relay the luminal diameter and the anatomy of the sleeve. It is both diagnostic and therapeutic, is less cumbersome as performed by the same provider in the same sitting alongside the surgery. It costs nothing more than an additional 5–10 min. Some surgeons use the EGD from the beginning of the surgery as a calibrated bougie and have obtained optimal outcomes on weight loss, 9 whereas some surgeons prefer its guidance for stapling the stomach 10 and prevention of postoperative stenosis. 11
In our center we have been using the postoperative UGI as a routine practice; however, we decided to test the benefits of performing an IEGD in patients undergoing LSG. Our use of EGD at the end of the procedure to visualize the gastric sleeve and perform an intraoperative leak test and manage any bleeding if found intraoperatively does not incur additional cost compared with a PUGI. We also noted that we were able to initiate the diet as early as an hour or 2 postoperatively with most patients in the IEGD group being able to get their stage I bariatric diet within 6 h on an average, whereas patients of the PUGI group had to wait until the UGI was performed, which is usually performed the next morning and was dependent on the availability of radiology staff among other hospital logistics and bureaucracy.
On review of our data, we were able to identify that almost 91.84% of patients in IEGD group were discharged on postoperative day (POD)1, 7.48% on POD2, whereas only 70.59% patients belonging to the PUGI group were discharged on POD1. Furthermore, 23.5% and 5.88% of patients were discharged on POD 2 and 3, respectively. The decreased POD1 discharge in the PUGI group and increased POD 2 and 3 discharge were all directly attributed to obtaining UGI and delays in initiating diet in these patients in comparison with IEGD group, both of which were statistically significant. The aforementioned was in addition to the added benefit of avoiding radiation exposure that comes with UGI testing although minimal. Strikingly the costs increased by 134.36% on an average in the PUGI compared with the IEGD in our study, the primary reason stems from the fact that patients in the PUGI group subjected to PUGI routinely had it the next day leading to delayed initiation of diet and an additional day of stay. It is also important to note that several patients had delays in these tests during weekends, holidays, which further increased the LOS. Although the cost of UGI in our institution is only an additional $166.23, additional LOS costs much more heavily and added to the economic burden at no clinical advantage.
Limitations
This is a retrospective study and not a randomized controlled study, hence individual patient factors might have influenced in the prolonged stay among some of them, but our significance proved even with respect to correction of the aforementioned possible bias. Economic factors were accounted for only at national and state average; there is wide variation with patient insurance from Medicaid, Medicare to private, and this can make gross alterations. The costs are also heavily influenced based on if the reimbursement is per package and or individualized.
Conclusion
In conclusion, based on our data we interpret that the benefits of IEGD far outweighs that of obtaining an PUGI, if a surgeon or institution deems it necessary or as part of their postoperative protocol. Although there is statistically significant increased operative time in the IEGD compared with PUGI group with a mean of about 6 min, the benefits stem from the significantly reduced hospital LOS, early initiation of diet, reduced cost, and total lack of radiation exposure, early discharge, and most importantly increased patient satisfaction with similar clinical outcomes.
Footnotes
Acknowledgments
We thank Columbia University College of Physicians and Surgeons at Harlem Hospital, Department of Surgery and Bariatric Division that have contributed to our study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.