
Abstract
Aim:
This study aimed to determine the incidence, predisposing factors, clinical presentation, and treatment options for portomesenteric and splenic vein thrombosis (PMSVT) in patients undergoing laparoscopic sleeve gastrectomy (LSG).
Materials and Methods:
A retrospective study was conducted of 507 patients who had LSG between March 2015 and June 2020. All patients received an extended (10 day) deep vein thrombosis prophylaxis protocol.
Results:
Of 436 patients who underwent LSG, four developed (0.9%) PMSVT. There was no significant difference in age or body mass index between patients with and without PMSVT (p = 0.547 and p = 0.535, respectively). There was a positive correlation between preoperative platelet (Plt-pre) values and PMSVT (p = 0.028, r = 0.157). The cutoff value for Plt-pre was 378 × 103 in receiver operating characteristic curve analysis (area under the ROC curve = 0.937, Youden index = 0.928, p < 0.001) with 100% sensitivity and 92.8% specificity rates. Plt-pre was found to be an independent risk factor for the development of PMSVT (odds ratio = 1.031, p = 0.046). There was no statistically significant difference in preoperative mean platelet volume (MPV-pre) between patients with and without PMSVT and MPV-pre was not found to be a risk factor for the development of PMSVT (p > 0.05).
Conclusion:
PMSVT is an infrequent but serious complication associated with bariatric surgery, especially LSG. The only independent risk factor was Plt-pre count.
Introduction
Bariatric surgery has gained popularity as it has a major effect on weight loss and obesity-related comorbidities. In contrast to these favorable results, it may also be associated with some undesirable complications such as thrombotic events. Due to obese patients having many predisposing factors, many surgeons use prophylactic agents in the preoperative period and during the postoperative period until discharge or sometimes for 2–4 weeks more.1–4
Portomesenteric and splenic vein thrombosis (PMSVT) is one such thrombotic complication. PMSVT is a rare but life-threatening condition with a mortality rate of 20–50% due to accompanying intestinal ischemia and infarction. 5 Probable etiologies are surgery, intraabdominal inflammation, bowel obstruction, trauma, hypercoagulable states, portal hypertension, smoking, oral contraceptive use, immobility, and so on.6–8 Although observed mostly after open abdominal surgery, increasing rates of PMSVT have been encountered especially following laparoscopic surgery with the enhanced popularity of bariatric procedures.
A limited number of case reports and a few multicenter series discuss PMSVT in the literature. This study evaluated the results of patients from one center with procedures performed by the same surgeon with the same technique to determine the incidence, predisposing factors, clinical presentation, and treatment options for PMSVT in patients undergoing laparoscopic sleeve gastrectomy (LSG).
Materials and Methods
Study design
In our clinic, bariatric surgery is performed based upon the following criteria and guidelines: patients must have a body mass index (BMI) ≥40 kg/m2 or a BMI ≥35 kg/m2 and accompanying comorbidities (diabetes, hypertension, coronary artery disease, hyperlipidemia, etc.). Blood tests and abdominal ultrasonography were performed in all patients during an average of 3 days preoperatively. Information from 507 patients, 18–65 years of age, who underwent bariatric surgery by a senior surgeon between March 2015 and June 2020, was retrospectively reviewed. Ethics committee approval was obtained [code number: 2020/08/05]. Informed consent was obtained from all patients. A total of 71 patients who underwent open bariatric surgery, other types of bariatric surgery, or revisional surgery were excluded from the study. Data from the remaining 436 patients who had LSG procedures were analyzed.
Prophylaxis for thrombosis
As prophylaxis, patients with a BMI <50 kg/m2 received 40 mg enoxaparin and patients with a BMI >50 kg/m2 received 60 mg daily from the preoperative night until the 10th postoperative day. All patients were mobilized early.
Surgical technique
LSG was performed in a standard split-leg French position using five laparoscopic ports. Intraabdominal pressure was fixed at 15 mmHg. After a liver retractor was placed, dissection of the greater curvature was carried out 2 cm from the pylorus and terminated on the angle of His using a vessel sealer and divider (LigaSure™; Covidien). After inserting a 36-French bougie into the stomach, an articulating laparoscopic stapler was used for the transection (Echelon Flex 60™, Endopath®; Ethicon). The stapled line was oversewn entirely in all patients. Absence of staple line leakage was confirmed with methylene blue and the air-water tests. The surgery was terminated after removing the specimen and placing a drain.
Treatment
All patients admitted to the emergency department after LSG with abdominal pain were evaluated with abdominal computed tomography (CT). Patients with suspected PMSVT were diagnosed with triphasic CT. Following a bolus of intravenous heparin, low-molecular-weight heparin (LMWH) was continued twice a day. None of the patients needed systemic thrombolytic treatment such as tissue plasminogen activator. Two patients needed to be hospitalized due to the severity of the abdominal pain. After an average of 5 days, they were discharged without any additional complications. No patients required surgical exploration. Thrombophilia evaluation was conducted for all patients and only one demonstrated abnormality.
Data collection
Demographic features, anticoagulation usage, predisposing factors, laboratory parameters, comorbidities, other specific conditions, operative duration, operational details, hospitalization duration, occurrence time of complication, and diagnostic and treatment procedures were all recorded from the patients' files. Perioperative 30-day complications were also recorded from the files. PMSVT was confirmed by triphasic CT.
Statistical analyses
Statistical analyses were performed using the IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY) and MedCalc software (v16 Ostend, Belgium). Quantitative variables were expressed as mean and standard deviation and categorical variables as absolute numbers and percentages. The variables were investigated using visual (histograms, probability plots) and analytical methods (Kolmogorov-Smirnov test) to determine whether they were normally distributed.
Patients were categorized into two groups, those who developed PMSVT and those who did not. All statistical analyses were performed between these two groups. Continuous data between two independent groups were analyzed using the Mann–Whitney U test and independent samples t-test. Categorical data were analyzed using the chi-square test and Fischer's exact test. Receiver operating characteristic (ROC) curve analysis was used in predicting the presence of PMSVT by computing the area under the ROC curve (AUC). Cutoff points computed with the maximal Youden index were selected. Logistic regression analysis was performed to determine the risk factors contributing to the development of PMSVT. A p-value of <0.05 was considered statistically significant.
Results
A total of 436 patients undergoing LSG between March 2015 and June 2020 were included in this study. The demographic and clinical characteristics of patients are summarized in Table 1. None of the patients developed major intraoperative complications. Postoperatively, 4 (0.9%) developed PMSVT. All patients with PMSVT were men. One of the four had a history of smoking and deep vein thrombosis. None of the patients had known liver disease; however, in one patient, cirrhotic alteration was observed in the liver intraoperatively (Table 2). No complaints were observed during the hospitalization of these patients, and all were discharged on the 4th postoperative day taking adequate oral fluids (>2 L/day).
Demographic and Clinical Characteristics of Patients
p-Value is statistically significant.
BMI, body mass index; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; F/M, female/male; HL, hyperlipidemia; HT, hypertension; LMWH, low-molecular-weight heparin; MPV-pre, preoperative mean platelet volume; Plt-pre, preoperative platelet count; PMSVT, portomesenteric and splenic vein thrombosis.
Characteristics of Patients with Portomesenteric and Splenic Vein Thrombosis
FL, fatty liver; IR, insulin resistance; M, male.
One patient stopped anticoagulant treatment postoperatively even though it was prescribed. This patient also had a history of deep vein thrombosis 3 years previously. Patients were readmitted at a median of 15 (range 13–24) days with the main symptom of abdominal pain for ∼2 days (range 1–5). All patients had elevated C-reactive protein and white blood cell levels. Two patients had complete concomitant thrombosis of the portal and splenic veins and one had minimal thrombosis in the proximal portion of the superior mesenteric vein. The other one had only portal vein thrombosis. All patients also had hypoperfused areas on the liver. None presented with intestinal infarction (Figs. 1 and 2). The median follow-up period was 26 months (range 15–36). Patients were evaluated intermittently with Doppler ultrasonography and CT. Imaging showed a partial recanalization in three cases and portal cavernoma formation in the other. All patients currently have no complaints related to PMSVT. Thrombophilia evaluation was achieved in all patients and only one demonstrated abnormality. The clinical features and treatment details are summarized in Table 3.
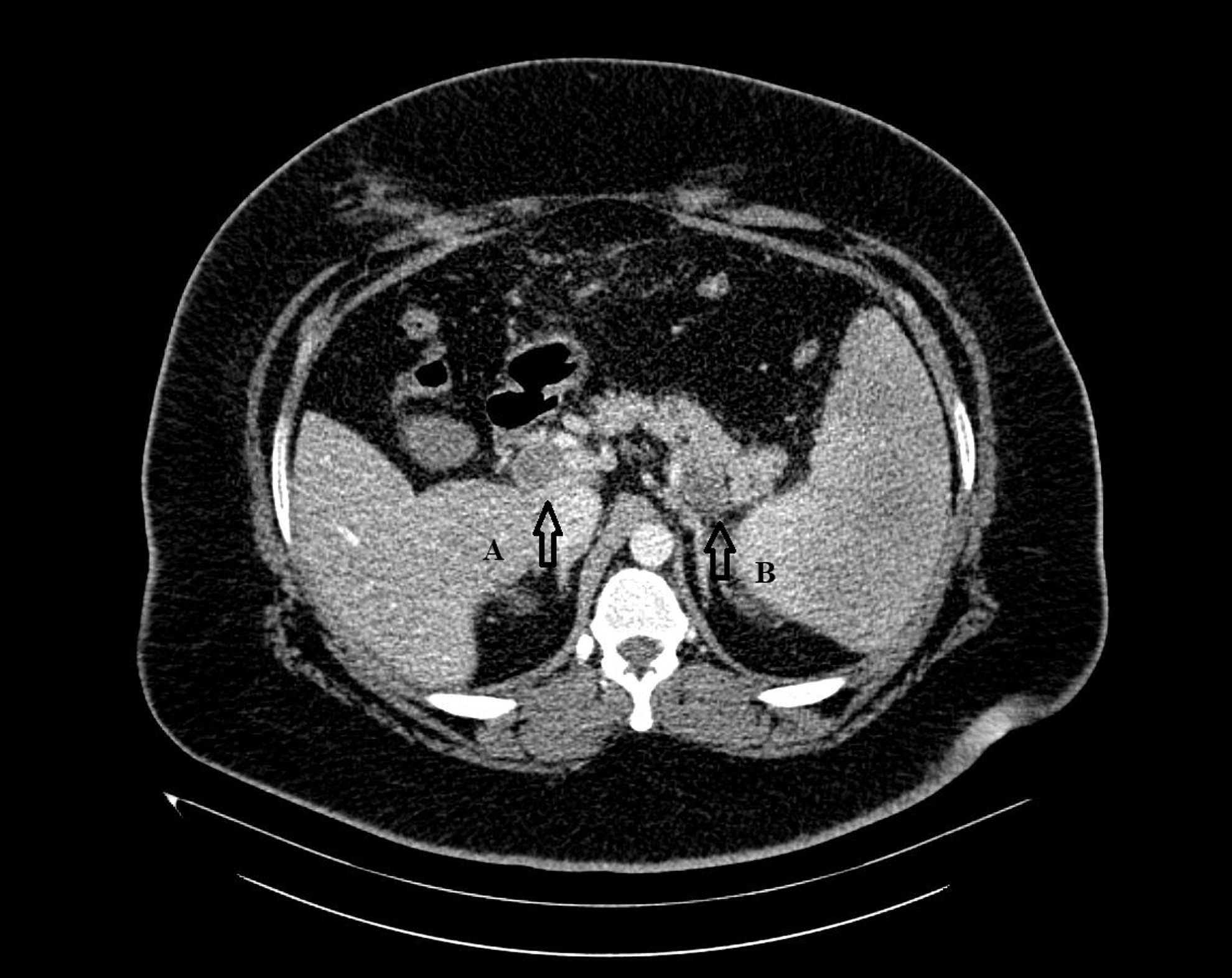
Portal and splenic vein thrombosis

Thrombosis beginning from the portosplenic junction.
Symptoms and Clinical Examination of Patients with Portomesenteric and Splenic Vein Thrombosis
ALT/AST, alanine aminotransferase/aspartate transaminase; AP, abdominal pain; CRP, C-reactive protein; E, epigastrium; F, fever; N, nausea; RH, right hypochondrium; UA, upper abdomen; WBC, white blood cell count.
There was no significant difference in age, BMI, and surgery time between patients with and without PMSVT (p = 0.547, p = 0.535, and p = 0.528, respectively). There was only a significant difference in preoperative platelet (Plt-pre) count among preoperative blood parameters between patients with and without PMSVT (p = 0.028) (Table 1). There was a positive correlation between Plt-pre and PMSVT (p = 0.028, r = 0.157). The cutoff value for Plt-pre was 378 × 103 based on ROC curve analysis (AUC = 0.937, Youden index = 0.928, p < 0.001) with 100% sensitivity, and 92.8% specificity (Fig. 3). Furthermore, Plt-pre was found to be an independent risk factor for the development of PMSVT (odds ratio = 1.031, p = 0.046) (Table 4). Preoperative mean platelet volume (MPV-pre) was not a risk factor (p > 0.05).
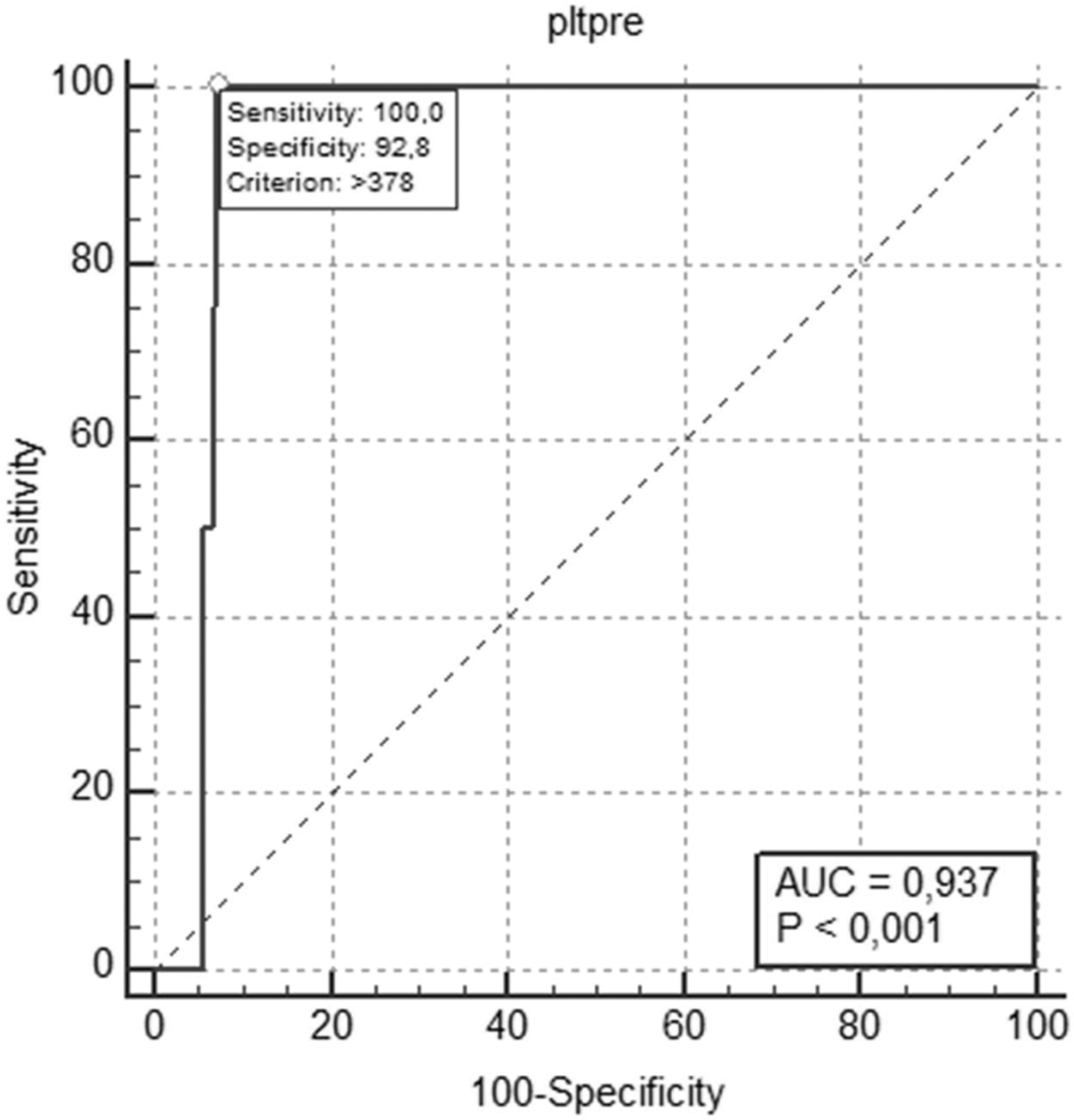
Receiver operating characteristic curve analysis of Plt-pre on the development of portomesenteric and splenic vein thrombosis. Plt-pre, preoperative platelet.
Logistic Regression Analysis of Preoperative Risk Factors on the Development of Portomesenteric and Splenic Vein Thrombosis
p-Value is statistically significant.
CI, confidence interval; OR, odds ratio.
Discussion
In this study, a 0.9% incidence of PMSVT was found. Among preoperative blood parameters, Plt-pre was determined to be an independent risk factor for the development of PMSVT. Particularly, a Plt-pre count >378 × 103 may be a stimulant for PMSVT development. Age, BMI, gender, and comorbidities were not found to be risk factors. The MPV-pre value also had no effect on the development of PMSVT.
Obese patients are known to have increased risks for venous thromboembolism as a consequence of inflammatory and hypercoagulable states.9–12 Recently, PMSVT has become much more visible in bariatric surgery and has been reported more often, especially after LSG compared to other bariatric procedures with an incidence of 0.3–1%. 13 In our study, the occurrence rate for PMSVT was compatible with that reported in the literature.
Many mechanisms have been associated with bariatric surgery and PMSVT, such as increased intraabdominal pressure related to gas insufflation and/or decreased portal/splanchnic venous blood flow,14,15 thermal injuries, Trendelenburg position (causing portal venous stasis), hypercarbia (correlated with mesenteric vasoconstriction and subsequent vasopressin release),16–19 and dehydration.20,21 The issue of liver retraction is contradictory in that while some studies considered it to be associated with PMSVT because of the pressure in the portal area, some argued that it did not affect.20–22 We always used liver retraction.
Hypercoagulability was the most commented issue associated with PMSVT. While protein C or S deficiency and prothrombin G20210A mutation are the most common hereditary risk factors, Factor VIII elevation was found to be related to PMSVT. 13 Activated protein C resistance, antithrombin III deficiency, Factor V Leiden mutation, elevated factor VIII, JAK 2 mutation, methylenetetrahydrofolate deficiency, lupus anticoagulants, and increased fibrinogen level are linked to thrombosis as well. 23 In our study, one patient had a history of thrombophilia (Factor V Leiden mutation). Thus, while thrombophilia appears to be the most potent factor in this case, it should be kept in mind that PMSVT can be multifactorial.
As mentioned, LSG is the operation most associated with PMSVT in bariatric surgery, even though some research alleges otherwise. 24 However, the reason for this association is not clear and may be related to it being a more popular operation. On the contrary, it is difficult to answer the question of why all patients are not affected if the cause is the manipulation of short gastric vessels. Furthermore, PMSVT is more often observed in a narrower LSG due to edema formation and dehydration, which bring about venous obstruction. 25 We did not include the other bariatric procedures in our study. Further investigations are needed in this regard.
Many studies demonstrated that the main affected vessel was the portal vein. Contrary to these other studies, we observed that the portal and splenic veins were affected together. In such circumstances, the prognosis can be unfavorable due to fatal complications; therefore, treatment must commence immediately.
PMSVT manifests with various clinical symptoms, the severity of which depends on the localization and degree of thrombosis. The most frequent symptom is abdominal pain, which could be confused with other conditions. All PMSVT patients in our study were readmitted to the hospital with abdominal pain. Other symptoms include abdominal distension, nausea, and fever. The same symptoms can also be observed in bariatric complications such as gastric leak, twisting, and so on. With abdominal pain in particular, many surgeons suspect the presence of a gastric leak. In our study, we used CT and surprisingly visualized a thrombosis. The addition of the superior mesenteric vein increases the severity of symptoms, especially colicky abdominal pain, which occurred in one patient in our study. If the thrombosis spreads, back pain occurs as well as ileus. 21 Portal hypertension and portal cavernoma are the complications seen most frequently in the late term, resulting in ascites and gastrointestinal bleeding.26,27 After beginning treatment, patients' complaints decrease dramatically.
Studies have shown a high MPV level and platelet count to be associated with portal vein thrombosis28–30 ; however, there is no study investigating the effects of both parameters on PMSVT development after LSG. Our study is the first such report and differs from the other studies in that MPV-pre did not affect the development of PMSVT. On the contrary, Plt-pre was defined as a risk factor for PMSVT in accordance with the literature.
For PMSVT treatment, the first step is anticoagulant drugs for at least 3–6 months. 24 The time of anticoagulation may be extended to 6–12 months 5 and even lifelong in cases of persistent thrombotic risk factors. 31 Commonly, unfractionated heparin, vitamin K antagonists, and LWMH are used. The gold standard in the treatment of acute postoperative PMSVT is a continuous intravenous unfractionated heparin infusion. Due to potential risks, such as bleeding and difficulty in controlling blood levels, LWMH is usually preferred, after which oral anticoagulant agents can be added. The treatment may not be satisfied every time. Intestinal ischemia and liver failure are the most undesirable results. Thrombectomy and/or catheter-directed thrombolysis are other treatment options, but are usually not preferred due to the consequence of the risks they bear. 32
Prevention of PMSVT is more important than its treatment. Patients' medical history must be taken into consideration and detailed exhaustively. The type and duration of postoperative anticoagulant medication should be planned according to possible risks. Caruso et al. suggested the use of long-term LMWH in the presence of known preoperative risk factors. 33 Preoperative prophylactic LMWH usage is an accepted application. There are many different practices concerning utilization time (presurgery, anesthesia induction, etc.); however, there is no consensus concerning PMSVT prophylaxis during the postoperative period. In our patients, we used LMWH for 10 days and all cases occurred after 10 days; therefore, we believe that prophylactic LMWH treatment should be continued for a longer period because these patients are more immobile and they may also drink less water then they claim.
The rate of PMSVT can be greater than expected due to mild unreported cases. Some asymptomatic cases may be undiagnosed and resolve spontaneously since they are not followed by imaging methods routinely. Nevertheless, this study includes data from a limited number of patients who were operated by the same surgeon using the same technique and have a long follow-up period.
Conclusion
Early diagnosis and treatment of PMSVT can be lifesaving. A high Plt-pre count should be a warning for the possibility of developing PMSVT. Anticoagulant therapy is preventive, but there is no consensus as to treatment time during the postoperative period. There is a need for larger prospective randomized studies to further evaluate the occurrence of PSMVT, identify associated risk factors, and determine the appropriate prophylactic strategy.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Review Board and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Authors' Contributions
Study conception and design—G.B.M., O.Y.; acquisition of data—G.B.M.; analysis and interpretation of data—G.B.M.; drafting of article—G.B.M.; critical revision of article—G.B.M.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.