
Abstract
Background:
In laparoscopic bariatric surgery the enhanced recovery after surgery pathway is proven beneficial for the rapid postoperative recovery of patients. Thoracic epidural analgesia is considered the gold standard for this type of surgery, but the placement of a thoracic epidural catheter can be difficult sometimes. The aim of this study was to evaluate the efficacy of erector spinae plane (ESP) block compared with transversus abdominis plane (TAP) block in the management of postoperative pain for laparoscopic bariatric surgery.
Materials and Methods:
Fifty-one patients were divided into two groups and received TAP block or ESP block and the primary outcome for this study was the assessment of postoperative pain intensity expressed as numeric rating scale (NRS) at 1, 6, 12, 24, and 48 h.
Results:
There was no statistical difference between ESP group and TAP group for NRS at the first hour (p = 0.101), whereas postoperative pain scores were lower in the ESP group compared with TAP group from 6 and 12 h after surgery (p = 0.032 and p = 0.010) respectively.
Conclusion:
The study showed a statistically significant superiority in postoperative pain control of ESP block from the 6th to the 12th-hour postoperative.
Introduction
Bariatric surgery is the most effective treatment for pathological obesity. Body mass index (BMI) ≥40 kg/m2 or ≥35 kg/m2 with comorbidities and the numbers of bariatric surgery are steadily increasing worldwide, 180.177 in 2014 to 394.431 in 2018.1,2
For obese patients, often suffering for obstructive sleep apnea, each type of surgery is high risk especially for perioperative respiratory complications and the opioid use for postoperative pain control can contribute to increasing the risk of respiratory depression. 3
To improve the perioperative path, the enhanced recovery after surgery (ERAS) protocol (Table 1) recommends an excellent multimodal management of postoperative pain, including techniques of regional anesthesia and without opioid use. 4
Enhanced Recovery After Surgery Protocol—Città di Castello Hospital
ERAS, enhanced recovery after surgery; ESP, erector spinae plane; TAP, transversus abdominis plane; TOF, train of four.
Currently in the literature there is no consensus or strong recommendation on which regional analgesic technique could be recommended or indicated in the first line in laparoscopic bariatric surgery.
Transversus abdominis plane (TAP) block has already proven its effectiveness in the management of postoperative pain both in abdominal and bariatric surgery 5 but, despite its effectiveness, still little used.
Ultrasound-guided erector spinae plane (ESP) block, a regional anesthesia technique, described by Forero et al. 6 in 2016 for use in thoracic neuropathic pain, leads to effective intra- and postoperative analgesia both for breast and thoracic surgery and for abdominal surgeries.7–12
The aim of this study was to compare the effectiveness in the postoperative pain control of TAP block and ESP block in 51 obese patients, to undergo laparoscopic surgery using the numeric rating scale (NRS).
Materials and Methods
A prospective observational study was designed.
Fifty-one patients, to undergo laparoscopic surgery at the hospital of Città di Castello, were included in the study in a period spanning from February 2019 to October 2019, subject to their signing of informed consent for the study and the consent form for the processing of their personal data in anonymous form.
All data management adhered to the Declaration of Helsinki.
Patients included in the study were aged from 22 to 70 years with an American Society of Anesthesiologists (ASA) risk ranging from II to III, BMI ≥40 kg/m2, BMI ≥35 kg/m2 with comorbidity, with no contraindications for the execution of regional technique.
Patients with allergies and/or contraindications for the administration of drugs used in the study were excluded from the study, as well as patients who presented chronic opioid use for therapeutic purposes and patients transferred to intensive care unit for the postoperative period.
According to the regional anesthesia technique used, the patients were divided into two groups:
Group 1 (25 patients): received single shot bilateral ultrasound-guided TAP block Group 2 (26 patients): received single shot bilateral ultrasound ESP block.
The primary outcome for this study was the assessment of postoperative pain intensity expressed as NRS at 1, 6, 12, 24, and 48 h.
The secondary outcomes were as follows:
Patients with postoperative nausea and vomiting (PONV) during the first 24 h
Patients who required rescue analgesic (nonsteroidal anti-inflammatory drugs)
Days of hospitalization.
All patients were admitted to hospital in the morning on the day of surgery and in all cases the same two anesthesiologists performed the block and the same surgeon performed the surgery.
TAP block was performed after general anesthesia induction, whereas ESP block was performed before general anesthesia induction.
Ultrasound-guided TAP block13–15 was performed after general anesthesia induction, before surgery starting, under aseptic conditions and patient in supine position, with a linear probe (10–5 MHz) and a Tuohy needle, 18-G × 80 mm.
We used subcostal and lateral approaches bilaterally, into the fascia between rectus abdominis and transversus abdominis muscles and between rectus abdominis and transversus abdominis muscles, and administered a total of 40 mL levobupivacaine 0.375%. 16
ESP block was performed before general anesthesia induction; in the operating room the patient was monitored with three-lead electrocardiogram, noninvasive blood pressure and pulse oximetry and, with the patient placed in sitting position, under aseptic conditions, we infiltrated 2 mL of 1% lidocaine at each level and a bilateral ultrasound-guided ESP block at T5 and T7 level was performed using Tuohy needle, 18-G × 80-mm and “in-plane” technique with a linear (10–5 MHz) or convex (3.5–5 MHz) probe.
When the needle came into contact with the transverse process, correct tip position was confirmed by the injection of 1 mL of saline solution 0.9% and by the visualization of linear fluid spreading and 10 mL of levobupivacaine 0.375% was injected for each level (total of 40 mL levobupivacaine 0.375%).
All patients were preoxygenated for 3 min in the ramp position and general anesthesia was induced with intravenously (IV) fentanyl 100 mcg, propofol 2.5 mg/kg, and Rocuronium 1.2 mg/kg and were intubated with the use of a video laryngoscope.
Anesthesia was maintained with Sevoflurane with a target of age-adjusted minimal alveolar concentration 1.0–1.5 in air and oxygen mixture with inspired oxygen fraction (FiO2) of 0.50 and sedation level was monitored with Bispectral Index System (BIS; Covidien Medtronic, Minneapolis, MN, USA).
Assisted ventilation was set in pressure mode with a tidal volume of 6–8 mL/kg, a peep: 6–8 cmH2O, a respiratory rate: 14–16/min and recruitment maneuver every 30 min.
All patients were administered 2 g of Cefazolin half an hour before the start of surgery.
All surgery were performed with laparoscopic technique with an intra-abdominal pressure of 12 mmHg, five trocars were placed (three of 12 mm and two of 5 mm) and no injection of local anesthetic on the insertion point of the trocars before performing the incision was administered.
All patients underwent anastomosis with gastrografin control on the third postoperative day and all were discharged on the third postoperative day.
Surgery was completed within a time range of 70–360 min.
Acetaminophen 1 g IV was administered 60 min before the end of surgery, and then every 8 h, and ketamine 15 mg IV was administered to all patients 30 min before the end of surgery. 17
During the surgery all patients benefited from prevention for nausea and vomiting based on dexamethasone 4 mg intravenous after tracheal intubation and Metoclopramide 10 mg intravenous before tracheal extubation.
Tracheal extubation was carried out in a semisitting position, with the help of train of four and with the use of sugammadex.
All patients were monitored in the recovery room for an hour after waking up, in a semisitting position, and pain was assessed before returning to the ward.
Postoperative pain was assessed using NRS 1 h after the end of surgery and subsequently in the ward at 6, 12, 24, and 48 h after surgery by ward nurses and anesthetists.
The evaluation of the NRS was obtained by means of a horizontal line with a numerical interval of 11 points. It is labeled 0–10, where 0 is an example of someone with no pain and 10 is the worst possible pain.
Wherever pain exceeded 3 according to the NRS, Ketorolac 30 mg was administered intravenously (IV) for a maximum of three times a day.
Statistical analysis
The Mann–Whitney test was used to analyzed independent discrete and non-normally distributed continuous variables (deviation from Gaussian distribution were checked by using the Shapiro–Wilk test, whereas Friedman test was utilized for repeated measures analysis. X2 test with Yates' correction and Fisher's exact test were used to compare categorical variables. Statistical significance was set at p ≤ 0.05 and all p-values were two sided. Data analysis was performed using IBM-SPSS® version 25.0 (IBM, Armonk, NY, USA, 2017).
Results
A total of 51 patients, homogeneous by demographic distribution, were enrolled in the study divided into two groups according to the postoperative analgesia protocol:
Group 1 (n = 25) who received TAP block
Group 2 (n = 26) who received bilateral ESP block.
The two groups were comparable regarding baseline characteristics of patients: age, gender, BMI, ASA physical status, comorbidities, type and duration of anesthesia, type of surgery, as well as the duration of surgery, and overall duration of the perioperative period. There was no statistically significant difference between the two groups regarding these parameters, as shown in Table 2.
Demographic, Anthropometric, and Clinical Variables
Continuous and discrete data are expressed as median, min and max; categorical data are expressed as number and percentage.
ASA, American Society of Anesthesiologists; BMI, body mass index; NRS, numeric rating scale; OSAS, obstructive sleep apnoea syndrome.
The two groups can be considered homogeneous for demographic, anthropometric, and clinical variables and for type and duration of surgery (Table 2).
Comparison of NRS score as shown in Table 2, in the first postoperative hour in recovery room, few patients have reported pain intensity of medium-low grade, median NRS 2 (0–5) for ESP block and median NRS 3 (0–6) for TAP block and was comparable between the two groups (p = 0.101): consequently, also percentage of rescue dose request between the two groups was not statistically significant.
At 6 and 12 h, postoperative pain intensity was minimal (NRS ≤ 3) on both groups but lower in the ESP group compared with TAP group (6 h: p = 0.032; 12 h: p = 0.010) and no patient asked for the rescue dose (Fig. 1).
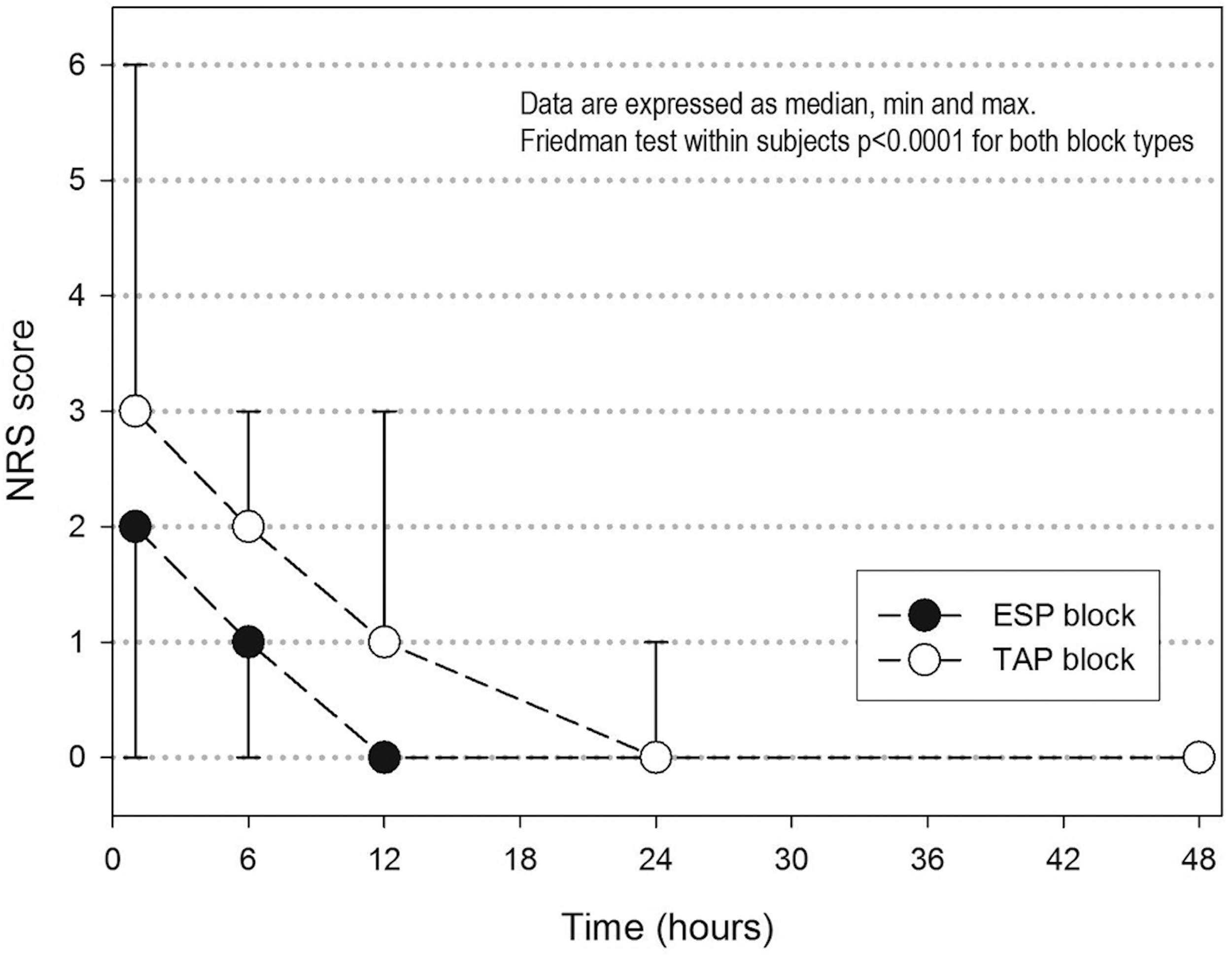
Median NRS at 1, 6, 12, 24, and 48 postoperative hours. NRS, numeric rating scale.
After 12 h up to 48 h no pain was recorded in either group and there was no statistical difference between the two groups.
For what about the second endpoint, the two groups had statistically comparable incidence of vomiting in the first 24 h (p = 0.726), despite anesthesiological protocol “opioid free.”
All patients were discharged from the hospital on the third day, without postoperative complications (Table 3).
Discharge Criteria
No levobupivacaine-related side effects or any complication related to both block techniques were noted.
Discussion
All patients included in this study were managed in an ERAS context, with the aim to analyze the effectiveness of the ESP block compared with the TAP block in the management postoperative pain and PONV. The obese population can be benefit from opioid-free anesthesia/analgesia only by maximizing use of locoregional anesthesia/analgesia techniques.
Opioid-free anesthesia is very important for improving the outcome of patients underwent bariatric surgery, often suffering from obstructive sleep apnea syndrome and with a high risk of respiratory depression with opioid analgesia 18
The original fast-track surgery was developed by surgeon H. Kehlet 19 for early recovery of normal vital functions and optimal pain control precisely laparoscopic mini-invasive surgery associated with thoracic epidural analgesia, but in 2016, in a meta-analysis, Borzellino et al. 20 stressed the fact that epidural analgesia might not offer any additional clinical benefits to patients undergoing laparoscopic colorectal surgery within an ERAS program.
Thoracic epidural analgesia may be the cause of rare, but serious complications such as epidural hematoma, 21 in addition to having a high failure rate from 13% to 32% in the context of major abdominal surgery. 22
TAP and ESP blocks have already proven effective in various abdominal surgeries, reducing morphine requirements.
TAP block provides an optimal postoperative pain control, with less demand for opioids, after laparoscopic bariatric surgery, lower PONV score, earlier ambulation, and a reduction of the length of hospital stay.15,18,23
ESP block has proven effective for pain management and for the reduction of morphine consumption in the postoperative in various abdominal surgeries whether laparoscopic or open.24,25
Chin et al. 26 report cases series in which ESP block was effective for the management of postoperative pain on three patients in bariatric surgery.
Few studies have compared these two techniques in abdominal surgery 27 and even less in the obese population for bariatric surgery. 28
In our study, we found that these two techniques lead to lower pain scores comparable in the first hour postoperative with the same rate of rescue dose request (Table 2).
At 6 h and 12 h, postoperative pain intensity was minimal (NRS ≤ 3) in both groups, but was lower in the ESP block compared with the TAP block (Table 2).
After 12 h, up to 48 h postoperative and until discharge from the hospital, none of the patients in the two groups had pain (Table 2).
Our results at the first hour, between the 6th to 12th, and from the 12th to 48th hour, corroborate exactly with those found by Abdelhamid et al. on a randomized study in which the ESP block was compared with the TAP block in sleeve gastrectomy. 28
Likewise, our results with regard to the management of postoperative pain with ESP and TAP block corroborate with those of the literature,23,26 with few requests for rescue dose (Table 2).
All 51 patients sat 4 h after surgery and walked 200 m after 6 h as required by the Eras protocols.
Randomized trials compared TAP block with systemic analgesia versus systemic analgesia alone, have found similar results to ours as regarding the TAP block. 18
In bariatric surgery the incidence of nausea and vomiting is variable but always present.
A randomized study on 122 patients did not show any significant statistical difference in the incidence of PONV during the first 24 h postoperative, between the group having received the antiemetics prophylaxis (60%) and the group having received placebo (67%). 29
Note that in this study, the patients had received morphine for postoperative analgesia.
Benevides et al. 30 in their study underlined as the combination of haloperidol 2 mg, dexamethasone 8 mg, and ondansetron 8 mg (HDO) does not cancel the incidence of PONV, but, nevertheless, the incidence of nausea at 0–2 h postoperatively was lower in group HDO compared with group ondansetron (O) (23.7% vs. 56.7%) and at 12–24 h postoperatively was lower in group HDO (23.3%) and group DO (dexamethasone 8 mg and ondansetron 8 mg) (26.7%) compared with group O (60%). At 0–36 h postoperatively, nausea was lower in group HDO compared with group O (53.3% vs. 86.7%). Vomiting at 0–36 h postoperatively was lower in group HDO compared with group O (20% vs. 53.3%).
In this study, opioids were administered for the treatment of postoperative pain.
Mittal et al. 15 in their study, comparing tap block and systemic analgesia in patients underwent laparoscopic sleeve gastrectomy procedures, reported lower PONV incidence, 26% in patients who performed TAP block.
Our results were in line with those found in literature: in the TAP block group we had an incidence of PONV of 20% and in the ESP group of 15.4% without significant statistical difference.
The cause of nausea and vomiting in patients after bariatric surgery is not clear; there may be direct surgical trauma gastric and incisions through branches of the vague nerves that could contribute to higher rate of PONV, but also an ineffective antiemetic prophylaxis and the administration of opioids are also favorable factors.31,32
Saber et al. 33 in their study on the use of TAP block in bariatric surgery found a benefit statistically significant in pain control only at 3 h postoperative, but there was no statistically significant difference in the request of postoperative rescue analgesia, in PONV episodes, in the time to resume walking, in hospital length of stay or time to return to work after discharge. They conclude that the efficacy of TAP block does not have an important impact on the ERAS pathway in bariatric surgery.
In contrast, another randomized trial comparing TAP block with systemic analgesia versus systemic analgesia alone found similar results to ours as regards the impact of TAP block on early outcome after laparoscopic surgery. 18
Also a prospective study with a large number patients (570) demonstrated the benefits of the TAP block integrated with an ERAS pathway for laparoscopic sleeve gastrectomy not only in term of postoperative pain, but also on nausea, vomiting, and earlier discharge. 23
In bariatric surgery, patients must follow a fast recovery path, but this path requires a multimodal management of postoperative pain as simple and effective regional anesthesia techniques and possibly not to use opioid drugs.
The two techniques proved to be very effective for the management pain during the 48 postoperative hours, with very few requests for rescue dose, low incidence of nausea and vomiting, but with an analgesic superiority in favor of the ESP block between 6 and 12 h postoperatively. All patients were able to sit in a chair at the fourth hour and walk at the sixth postoperative hour, and all were discharged from the hospital on the third day without complications.
ESP block may be a valid alternative for postoperative pain management in bariatric surgery and ERAS pathway in view of its effectiveness and simplicity of execution. Limitations of our study would be the small sample size and nonrandomized. This result must be confirmed by randomized studies with a large sample size.
Conclusions
The two techniques proved to be very effective for the management of pain during the 48 postoperative hours, but with an analgesic superiority in favor of the ESP block between 6 and 12 h postoperatively.
Ultrasound-guided ESP block in single shot is an easy, mini invasive, and effective regional analgesic technique, and can be a part of an effective multimodal analgesia in obese patients undergoing bariatric surgery for ERAS pathway reducing the postoperative requirement of rescue dose analgesics and decreasing the incidence and severity of PONV.
However, more research with larger and randomized sample are required to confirm our findings.
Footnotes
Authors' Contributions
T.C.B. and M.C. performed the anesthesiological procedures, followed the patients in the postoperative period, and helped to write the article. D.P.S. helped to write the article. A.C. and S.V. performed the surgeries, followed the patients in the postoperative period, and reviewed the article. V.B. edited the statistical part of the article. C.B. performed the anesthesiological procedures, followed the patients in the postoperative period, and helped to review the article. V.C., C.C., C.T., and S.M. followed the patients in the postoperative period and helped to review the article. M.C. performed the surgeries, followed the patients in the postoperative period, and reviewed the article. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.