
Abstract
Background:
Secondary achalasia in the setting of an adjustable gastric band is a known, but rare complication. Most of the symptoms usually resolve after deflating or removing the gastric band, but dysphagia symptoms may persist. We present a case report of a patient with secondary achalasia in the setting of an adjustable gastric band, who required delayed resection of fibrous pseudocapsule to treat persistent dysphagia symptoms after removal of the gastric band.
Methods:
We performed a literature search using EMBASE and MEDLINE databases to review literature on persistent dysphagia symptoms after removal of adjustable gastric band in the setting of secondary achalasia.
Results:
We present the case of a patient who had secondary achalasia in the setting of an adjustable gastric band. Despite removal of the gastric band, dysphagia symptoms persisted, requiring delayed resection of fibrous pseudocapsule to relieve the obstructive symptoms. We review the literature from three case reports and two conference abstracts discussing persistent dysphagia symptoms after removal of adjustable gastric band in the setting of secondary achalasia.
Conclusion:
Our recommendation is to resect anterior portion of the fibrous pseudocapsule at the time of removal of an adjustable gastric band in patients with suspected secondary achalasia.
Introduction
Laparoscopic placement of an adjustable gastric band was widely used for surgical management of patients with severe obesity in the 1990s and 2000s in North America and around the world.1–5 By late 2000s, more than 100,000 individuals in the world were believed to have undergone placement of an adjustable gastric band. 6 Unfortunately, the initial enthusiasm toward and acceptance of this technique by bariatric surgeons was tempered by long-term data demonstrating high rates of complications and poor weight loss results.7,8 Common reported complications after placement of an adjustable gastric band include port revision and gastric band slippage or erosion.2–4,9 Over 50% of patients who had an adjustable gastric band placed will eventually undergo band removal.10,11 The most common reasons for removal of an adjustable gastric band include dysphagia, failure of weight loss or weight regain, band slippage, and gastroesophageal (GE) reflux symptoms. 1 One of the less common long-term complications of adjustable gastric band is secondary achalasia usually seen with longstanding esophageal obstruction. We present a case of a patient with secondary achalasia in the setting of an adjustable gastric band, who required not only removal of an adjustable gastric band but also a delayed resection of fibrous pseudocapsule to achieve resolution of the dysphagia symptoms. We also review the available literature on persistent dysphagia symptoms after removal of adjustable gastric band in the setting of secondary achalasia.
Methods
We searched both EMBASE and MEDLINE databases to identify studies describing patients with persistent dysphagia symptoms following removal of adjustable gastric band in the setting of secondary achalasia. No language restrictions were made. EMBASE database was searched from 1947 to December 18, 2020, and MEDLINE was searched from 1946 to December 18, 2020. The following medical subheadings were used: (1) Exp Gastric band AND secondary achalasia mp/OR pseudoachalasia mp/OR exp esophagus achalasia and (2) Gastric band removal mp AND exp dysphagia.
Case presentation
We present a case of a 75-year-old female with past medical history of class II obesity (body mass index [BMI] = 36 kg/m2), hypertension, hypothyroidism, dyslipidemia, restless leg syndrome, and depression. Past surgical history includes appendectomy, hysterectomy, and laparoscopic insertion of an adjustable gastric band 6 years ago. Following insertion of the gastric band, the patient lost ∼50 pounds and achieved a BMI nadir of 28 kg/m2; however, she had progressive symptoms of dysphagia to solids and eventually to liquids, as well as GE reflux, which were not present before the insertion of the gastric band. One year ago, she was seen by a nonbariatric surgeon on an urgent basis and had complete deflation of the gastric band, which did not relieve her symptoms of dysphagia. The surgeon proceeded with a laparoscopic removal of the adjustable gastric band and port. This did not relieve her symptoms of dysphagia to solids and liquids, regurgitation with every meal, and epigastric pain. As such, an upper gastrointestinal series was performed and was reported as dilated tortuous esophagus and a tight GE junction suspicious for achalasia (Fig. 1A). This prompted a referral to our center for an upper endoscopy and esophageal manometry.
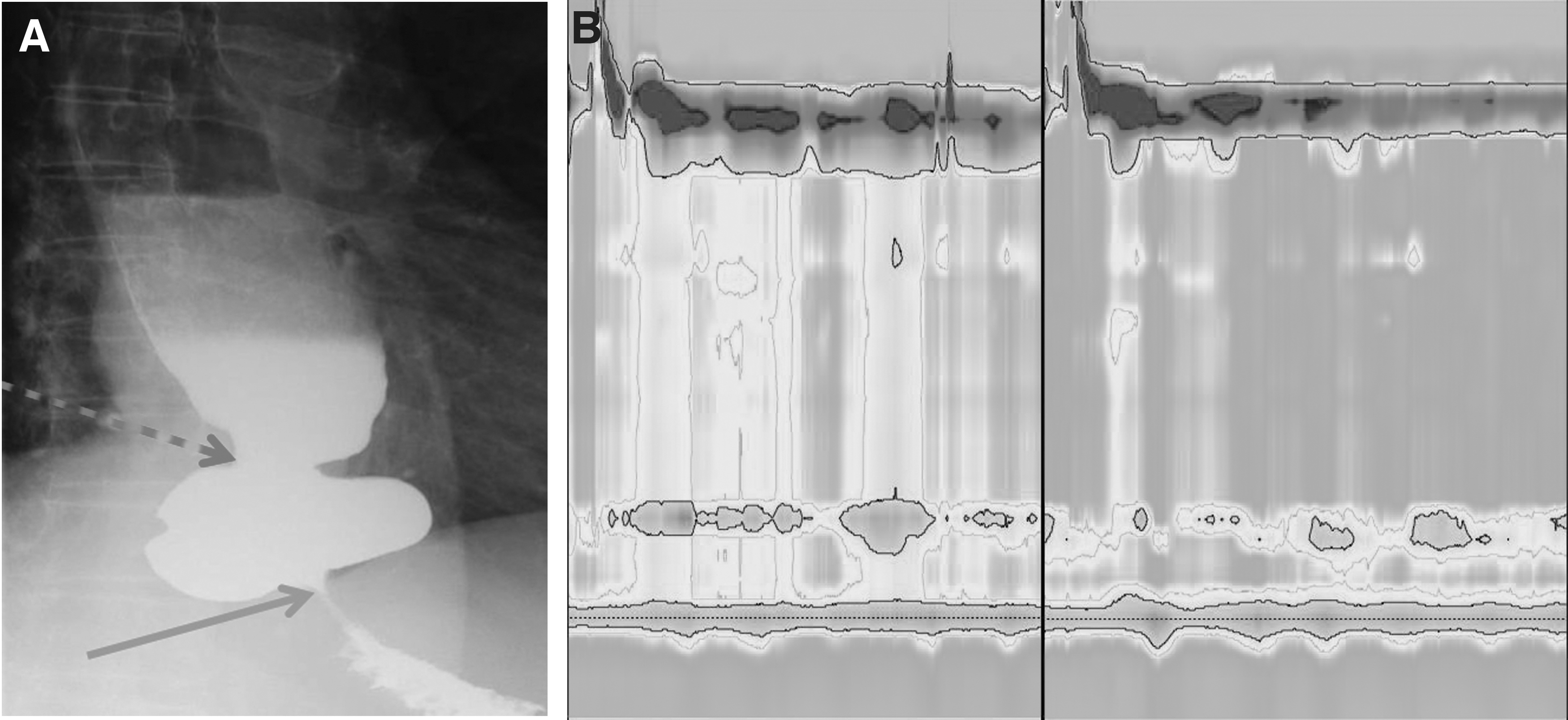
Upper endoscopy demonstrated a dilated esophagus with retained food and pills, as well as severe stasis esophagitis. The GE junction was patent, which was not in keeping with primary achalasia; however, there was an area of obstruction 2–3 cm distal to the GE junction at the location of the adjustable gastric band. Esophageal manometry demonstrated aperistalsis and panesophageal pressurization of the esophagus, normal relaxation of lower esophageal sphincter, and a fixed high-pressure zone distal to the GE junction at the prior location of the gastric band (Fig. 1B). Esophageal manometry was consistent with secondary achalasia. Review of the upper gastrointestinal series (Fig. 1A) confirmed persistent obstruction at the site of prior adjustable gastric band below the GE junction. Repeat upper endoscopy with through-the-scope balloon dilation of site of obstruction to 20 mm did not improve her symptoms and the patient continued to lose weight.
A decision was made to proceed to the operating room for laparoscopic resection of obstructing fibrous pseudocapsule, concurrent placement of a feeding gastrostomy tube, and intra-operative gastroscopy. At surgery, we identified a thick circumferential fibrous pseudocapsule at the prior location of the adjustable gastric band, which was causing an ongoing partial obstruction of the proximal stomach (Fig. 2A). The anterior aspect of the fibrous pseudocapsule was resected and sent for pathologic examination (Fig. 2B). A gastrostomy feeding tube was placed to allow for supplemental enteral nutrition if patient's symptoms did not improve after surgery. Intraoperative upper endoscopy demonstrated stasis esophagitis with confirmed resolution of partial obstruction at the location of the pseudocapsule. Patient was discharged home on the day of her operation and was seen in clinic for follow-up in 2 and 6 weeks. Her dysphagia symptoms to solids and liquids, as well as GE reflux symptoms resolved completely after surgery. Gastrostomy tube was removed at 6 weeks without being used and patient continued to do well with 1.2 kg weight gain after her operation. Pathology demonstrated scar tissue with signs of chronic inflammation. No further treatment was required.

Results
In our literature review, we identified three published case reports and two conference abstracts describing persistent symptoms of dysphagia after removal of adjustable gastric band in the setting of secondary achalasia (Table 1). There were no case series or cohort studies of this rare complication following insertion of adjustable gastric band. Resection of remaining pseudocapsule was performed in four out of six patients,12–14 concurrent Heller myotomy was performed in one patient, 9 and endoscopic balloon dilation was successful in two patients. 15
Summary of Relevant Studies Found During Literature Review
Discussion
Secondary achalasia in the setting on an adjustable gastric band is a rare late complication with the true incidence likely underreported.5,16–18 Secondary achalasia appears to be responsible for dysphagia symptoms in 2–4% of patients who end up undergoing band removal.19,20 The presentation of secondary achalasia is often insidious and progressive and can occur within months or even years after the insertion of the adjustable gastric band.5,14,17 The pathophysiology of this condition is not well understood; however, the ongoing obstruction at the location of the gastric band likely results in often irreversible changes in the esophageal body peristalsis as esophageal dysmotility is reported in up to 90% in studies of symptomatic patients.17,18
Previously reported treatments for dysphagia in the setting of an adjustable gastric band with or without secondary achalasia include fluid aspiration and removal of the gastric band.17,18,21 In most cases, the symptoms should resolve with fluid aspiration or removal of the gastric band.
Our case presentation is similar to the Losh et al. 9 and Vallin et al. 13 as our patient developed both secondary achalasia and functional obstruction from the remaining fibrous tissue and different from Modia et al., 14 AlSabah et al., 12 and Scozzari et al. 15 as those patients did not have confirmed manometric evidence of secondary achalasia.
Conclusion
Secondary achalasia in the setting of an adjustable gastric band is a rare complication of adjustable gastric band surgery. Simple removal of an adjustable gastric band without resection of the fibrous pseudocapsule may not result in resolution of dysphagia and GE reflux symptoms due to the inability of the esophagus to move a food bolus through the area of partial obstruction from the pseudocapsule. As such, we recommend routine resection of the anterior component of the fibrous pseudocapsule at the time of removal of adjustable gastric band in patients with findings of esophageal dysmotility and esophageal dilation on upper gastrointestinal series to prevent ongoing dysphagia symptoms after gastric band removal.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.