
Abstract
Background:
Due to exponential obesity prevalence, the number of bariatric surgery (BS) procedures has considerably increased. BS improves ovulatory function and natural fertility in some women. However, its effect on ovarian reserve is poorly known. The objective of this study was to carry out a systematic review of the literature to evaluate the impact of BS on ovarian reserve for women with obesity.
Methods:
In this systematic review, PubMed and EMBASE databases were searched for studies evaluating the results of ovarian reserve tests in obese women before and after BS, and published between January 1st, 2000, and March 1st, 2020.
Results:
Eight studies were included, totaling 355 women with serum antimullerian hormone (AMH) levels evaluated before and after BS. The majority of currently available studies report a decrease in AMH levels occurring 6 and/or 12 months after surgery, which could suggest an ovarian reserve impairment following BS.
Conclusions:
Although the pathophysiological mechanisms are poorly understood, this alteration raises concerns regarding long-term fertility following BS. Larger prospective controlled cohort studies will be necessary to provide a conclusion about the potential effect of BS on ovarian reserve. If a deleterious effect is confirmed, oocyte cryopreservation before surgery could be discussed.
Introduction
During the past three decades, an increase in obesity prevalence has been observed worldwide, with more than one-third of the world's population being overweight or obese in 2016. Female obesity has been associated with a high risk of adverse pregnancy outcomes, such as miscarriage, gestational diabetes, hypertension, and preeclampsia.1,2 In addition, many studies have underlined the deleterious effects of obesity on women's fertility, 3 especially on ovulatory infertility related to polycystic ovarian syndrome (PCOS). 4 After in vitro fertilization (IVF) treatments, poorer outcomes, such as higher doses of gonadotrophins, increased cycle cancellation rates, and decreased live birth rates, have been reported.5–7
Weight loss may improve fertility8,9 and is advised in clinical international recommendations.10,11 However, diet and lifestyle measures are often unsuccessful to induce sufficient and long-term weight loss in patients with severe and complex obesity. On the contrary, bariatric surgery (BS) has proven its efficiency to achieve fast and substantial weight loss, associated with decreased comorbidities and long-term mortality, and improved quality of life.12,13 Due to exponential prevalence of severe and complex obesity, the number of BS procedures has increased considerably in recent years, 14 also concerning reproductive-age patients. Weight loss after BS seems to be associated with significantly improved obstetrical and perinatal outcomes, 15 with a decreased risk of gestational diabetes, preeclampsia, and fetal macrosomia.16,17 In addition, weight loss after BS may be followed by decreased incidences of menstrual irregularity and PCOS, 18 increasing the chances of spontaneous pregnancy. 19 Even though BS could constitute a possible strategy to manage obesity-linked female infertility, some data suggested that it could be associated with a detrimental effect on ovarian reserve.
Although not strictly associated with spontaneous fertility, ovarian reserve is a key parameter to consider during fertility evaluation in women because it is associated with early follicle loss, menopause onset, and ovarian response to hormonal stimulation. Serum antimullerian hormone (AMH) levels and antral follicle count (AFC) are currently considered as the most reliable markers of ovarian reserve, 20 because they do not considerably vary within cycles or during birth control pill intakes, contrarily to other hormonal markers of ovarian follicular status. A postsurgical decrease in serum AMH levels has been reported by some authors, leading to some concerns about a potential ovarian reserve impairment following BS.
In this context, our study aims to conduct a systematic review to evaluate the impact of BS on ovarian reserve for women with obesity on ovarian reserve.
Methods
Literature search strategy and eligibility criteria
A literature search was conducted with the use of the PubMed and EMBASE electronic databases focusing on identifying articles published between January 1st, 2000 and March 1st, 2020. No restriction concerning the language of publication was applied. The following key words were used: (“Bariatric surgery” [MeSH terms] OR “Bariatric surgery” [All fields]) AND (“ovarian reserve” [MeSH terms] OR “ovarian reserve” [All fields] OR “anti-mullerian hormone” [MeSH terms] OR “anti-mullerian hormone” [All fields] OR “AMH” [All fields] OR “antral follicular count” [All fields] OR “antral follicle count” [All fields]). The systematic review was performed in accordance with The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) recommendations. 21 Ethics approval was not required for this systematic review.
Studies selection and data extraction
After eliminating duplicates, two independent reviewers (S.D. and N.S.) independently performed a screening from the title and abstract of all articles to exclude irrelevant citations. Any disagreement or uncertainty was resolved by the involvement of a third reviewer (C.D.). Full texts of potentially relevant articles were retrieved and assessed for inclusion by two reviewers (S.D. and N.S.), and data were extracted from included articles using a data extraction form developed for the present review. Main evaluation criteria for ovarian reserve tests were serum AMH levels and AFC. Studies evaluating the results of one or both of these ovarian reserve tests following BS in women with obesity were eligible for inclusion. Review articles were excluded.
Data synthesis
The following study details were extracted to characterize the included studies: study authors, publication year, country, study design, sample size, mean age of included patients, type of BS, body mass index before and after BS, AMH levels before and after BS, and details about subgroups (in particular, women presenting with PCOS).
Results
Study selection
The search strategy identified a total of 63 articles, including duplicates and articles that finally had no relevance to primary research questions. After review of 45 abstracts, 16 full-text articles were assessed for eligibility. Among them, eight articles were appropriate to be included in the systematic review (Fig. 1).
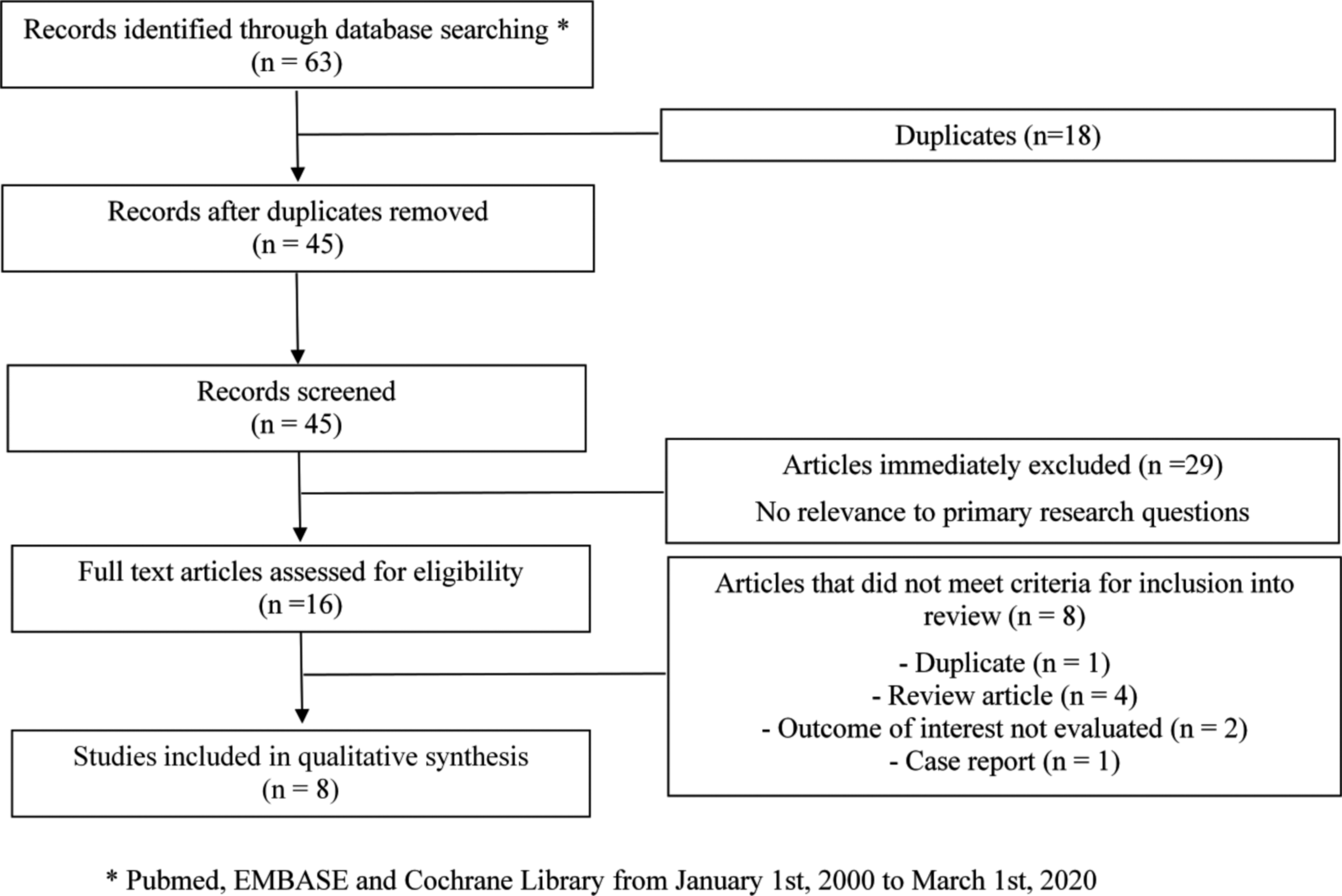
Flowchart of study selection for systematic review.
All eight eligible studies were cohort studies. The study sample sizes were small, ranging from 1622 to 75, 23 and totaled 355 women undergoing BS, divided in 11, 176, and 139 women undergoing gastric banding, sleeve gastrectomy, and gastric bypass, respectively (n = 29 not specified) (Table 1). In two studies, results were compared according to ovarian status (PCOS or not).23,24 Study participants were from Asia, 23 Europe,24–27 Middle East, 28 and United States.22,29
Characteristics of Studies Included in the Systematic Review
Results are presented as means ± standard errors (or ranges when means not available). Bold italic numbers are statistically different.
AMH levels were determined at 87 ± 30 days after surgery in Merhi et al. and at 65 ± 5 days in Sahab al Kabbi et al.
AMH, antimullerian hormone; BMI, body mass index; PCOS, polycystic ovarian syndrome; NA, not available.
Impact of BS on ovarian reserve tests
No study evaluating the effect of BS on AFC was currently identified in the literature. All eight articles reported the evolution of serum AMH levels after BS in women with obesity.
Five studies concluded that AMH levels decreased significantly at 6 months23,25,27,28 and/or 12 months after BS.24,25,27 This decrease similarly concerned both the subgroup of women with PCOS and the subgroup without PCOS.23,24 Among those studies, only one had a control group of normal weight women, 24 but did not report the AMH evolution in this group. On the contrary, one study reported a significant increase of AMH levels 3 and 6 months after sleeve gastrectomy. 26 At last, two studies concluded that AMH levels did not decrease significantly 6 or 12 months after BS,22,29 apart from a specific subgroup of women younger than 35 years of age. 22 Among those studies, one had a control group of women undergoing weight loss through lifestyle modifications. 29 No study mentioned any follow-up beyond 12 months. Due to strong heterogeneity across selected studies, especially with different studied populations and outcomes, it was not possible to perform any meta-analysis.
Discussion
While results remain scarce and heterogeneous, the majority of currently available studies report a decrease in serum AMH levels 6 and/or 12 months after BS. Although AMH appears to be a weak independent predictor of spontaneous fertility, this observation raises concerns regarding short- and long-term fertility of women with obesity after BS.
Indeed, AMH levels are routinely used worldwide to predict ovarian response to controlled ovarian stimulation in women undergoing IVF 20 and iatrogenic damage to the ovarian follicle reserve. 30 The postoperative decline in AMH levels after BS could then be related to a decrease in the number of oocytes obtained for IVF, even though it is admitted that the number of oocytes is key point for cumulative live birth rates following IVF. 31 Results from IVF cycles performed after BS remain scarce and controversial. One study reported a decrease in the number of collected and mature oocytes in 29 patients with obesity who underwent BS when compared to two control groups without surgery, 32 with no significant difference in pregnancy rates. On the contrary, Milone et al. reported a significant increase in the number of retrieved oocytes from 40 patients having undergone two IVF cycles, one before surgery and another one 12 months after surgery, 33 resulting in significantly higher pregnancy rates after surgery. Finally, in a recent French retrospective multicenter cohort study comparing 83 women with a history of BS to two different control groups, no significant impact on IVF prognosis was observed in terms of number of oocytes or pregnancy rates. 34
Several hypotheses can be made regarding the possible pathophysiological mechanisms involved. Massive and rapid weight loss could lead to the release of toxic substances and fat-soluble endocrine disrupters that could be harmful to ovarian function. The decrease in AMH levels could also be due to the malabsorption of nutrients 35 required for proper functioning of the female reproductive system and/or affecting the regulation of expression of AMH gene. This hypothesis could concur to partly explain the opposing results observed in Pilone et al. study, 25 reporting a significant increase of AMH levels, 3 and 6 months after sleeve gastrectomy, a surgical procedure that involves less malabsorption. Unfortunately, the majority of studies did not differentiate the results according to the type of surgical procedure. Finally, the postoperative decline in AMH levels could be in favor of an improvement in the hormonal profile of women presenting PCOS, leading to a short-term improvement of fertility in this subgroup of patients. Indeed, women with PCOS show markedly raised AMH levels, due to both the increased number of small antral follicles and intrinsic characteristics of granulosa cells. A recent study, 36 which could not be included in the review because of its publication date, is in agreement with this hypothesis. Indeed, in a population of 38 women undergoing BS, Nayak et al. showed a decrease in AMH levels in the PCOS subgroup in contrast with an increase in the non-PCOS subgroup. 36 However, the mean AMH levels reported in the available included studies do not seem to be consistent with this single hypothesis. Moreover, the decrease in AMH levels was observed both in PCOS and in non-PCOS subgroups,22,23 rather suggesting a mid- to long-term deleterious effect on ovarian reserve, even if the precise mechanisms still remain unknown.
Available studies evaluating the AMH level kinetics after BS have strong limitations, which make formal conclusion difficult to be drawn. Indeed, the studied population sizes are small, ranging from 16 to 75 selected patients. Few data concerning prior fertility status are reported, and various factors that could affect the level of AMH, such as smoking, alcohol, hyperprolactinemia, or hyperandrogenism, 37 have not been addressed, making the results of those studies debatable. The designs of the studies are questionable with only two out of eight studies proposing a control group, defined by women undergoing weight loss after lifestyle modifications 28 or normal weight women without any AMH evolution assessment. 23 A meta-analysis could have addressed some of the limitations of the published studies, but the heterogeneity of the presentation of the results currently limits its feasibility. Furthermore, the follow-up of patients after BS is imperfect with no follow-up after 12 months in any publication. It would then be interesting to set up larger and longer prospective cohort studies to provide a clear conclusion about the effect of BS on ovarian reserve, including serum AMH levels, and also AFCs, which were not evaluated in any available study. Those studies should investigate the AMH levels evolution after 12 months or even more, to clarify whether the decrease could be transient and parallel to the weight loss, or, on the contrary, would be confirmed over time. Finally, because the impact of BS on AMH levels may be very different according to age, especially because of physiological ovarian reserve depletion, subgroup analyses according to female age at BS should be performed.
The discussion regarding the proposition of BS for women with obesity and infertility should remain personalized, as its interest largely depends on the context (age, ovarian function, including ovarian reserve, and indication of IVF). It is usually not recommended to achieve a pregnancy during the first year after surgery because of higher risks for prematurity and/or small for gestational age. 38 Then, the risks associated with ovarian reserve decrease due to physiological aging during this interval, and possibly following the surgery itself should be individually balanced with the awaited benefits of weight loss, especially in terms of obstetrical and neonatal outcomes. In this context, cryopreservation of oocytes after controlled ovarian stimulation before surgery could be discussed. Although data on the oocyte quality of obese women still remain controversial, 39 it would make it possible to avoid the consequences of ovarian aging, while allowing a subsequent pregnancy under more favorable uterine and systemic conditions.
Conclusions
Finally, the literature tends to show a decrease in serum AMH levels at 6 and 12 months after BS, which could correspond to ovarian reserve impairment. Nevertheless, the published studies are based on small numbers mostly without any control group. Prospective studies will be needed to formally conclude not only on the impact of BS on ovarian reserve, but also on spontaneous fertility and IVF results, as well as on the relevance of oocyte cryopreservation before BS in women of childbearing age with obesity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.