
Abstract
Gastric fistula is one of the most dreadful events after sleeve gastrectomy (SG). That is justified by the fact that there is no consensus regarding what would be the optimal management for this morbid event. In the recent years, authors have pointed to the benefits of endoscopic interventions, with the implantation of stents, aiming to relieve the intragastric pressure and facilitate the natural closure of the fistulous path. However, the literature on this topic is scarce and the results are quite heterogenous. This article reviewed the use of endoscopic stents combined or not with surgical or percutaneous drainage in the treatment of gastric fistulas after SG, highlighting the scientific evidence that exists and discussing the need for further research on this topic.
Introduction
Today, bariatric surgery represents the most effective treatment for morbid obesity, being indicated for patients with body mass index (BMI) ≥40 kg/m2, or those with BMI ≥35 kg/m2 associated with other comorbidities, especially systemic arterial hypertension and diabetes mellitus.1–4 Between the surgical techniques performed nowadays in the United States, sleeve gastrectomy (SG) is the most popular, being performed approximately three times more compared with Roux-en-Y gastric bypass (RYGB) in this country, showing encouraging short- and long-term results regarding weight loss and improvement of the metabolic panel of patients. 5
Although usually safe, some complications may occur after SG, such as bleeding (0–2%), stenosis (0–2%), and staple line leaks (0.5–7%).6–8 An additional important complication is the fistula formation in the remnant stomach, especially in the His angle, which is a region with lower vascularization and thus more vulnerable to ischemic injury. Besides the ischemic component, fistulas may also arise due to distal stenosis of the gastric sleeve, at the incisura angularis, which impairs food outflow and raises the intragastric pressure, predisposing disruption in integrity of the staple line and leading to persistent leakage. 9
The treatment of gastric fistulas after SG is a great challenge given the lack of consensus in literature on what would comprise the ideal intervention. The initial approach in a hemodynamically stable patient consists in non-surgical intervention, including clinical support and endoscopic treatment modalities. The conservative measures include antibiotic therapy, nutritional support, proton pump inhibitors and drainage of abscesses. 10
Classically, the surgical approach was taken as the standard intervention, consisting of peritoneal toilet and apposition of intra-abdominal drains adjacent to the fistula site, which aim to reduce the inflammatory process resulting from the fistula. Nowadays, however, there is a tendency of limiting the indication of surgery for hemodynamically unstable patients or when there is an impossibility for percutaneous drainage.10,11
With the recent technological progress in the field of endoscopy and minimally invasive surgery, the implantation of endoscopic stents has proved to be a safe and effective method in the management of patients with fistula after bariatric surgery. Endoscopic self-expandable stents can be used to correct the axis deviation (gastric twist), isolate the leak site, and decrease the intraluminal pressure. In addition, they allow earlier enteral nutrition and shorten the length of hospitalization.11,12 The stent implantation should be performed early in the treatment of fistula and must be linked to the control of the septic foci with surgical or percutaneous drainage of fluid collections. The ideal length of stay for an endoscopic stent is between 4 and 6 weeks, with risk of re-stenosis with a time of permanence shorter than that. On the other hand, an extended period of permanence may predispose mucosal hyperplasia and stenosis, hindering the removal of the device. 13
This descriptive review assesses the existing literature regarding the use of endoscopic stents for the treatment of gastric fistulae after SG, trying to outline the global risks and efficacy of this procedure. The following question was asked according to Population, Intervention, Comparison, and Outcome criteria: “Is the endoscopic management with self-expandable stents safe and effective for the treatment of gastric fistulae after SG?.”
Methods
We searched in the PubMed/MEDLINE and Scientific Electronic Library Online (SciELO) databases, using the following terms in different combinations: “sleeve gastrectomy,” “fistula,” “leak,” “endoscopy,” and “stent.” This review covered all studies published between 2009 and 2019 in English, Portuguese, and Spanish language. The selection of articles was performed by two different authors from title and abstract screening. Divergences between evaluators were resolved through consensus.
Case series and longitudinal studies that analyzed the endoscopic approach, with intraluminal insertion of self-expandable stents, for the treatment of gastric fistulae after SG were reviewed. In vitro and animal studies; previous literature reviews and case reports; studies that did not specify their results according to each endoscopic procedure; and studies that analyzed SG and RYGB as a single group were excluded.
The main outcomes studied in this review were the success rate of the endoscopic management of gastric fistula after SG and the complications related to these procedures. The clinical features of fistulae and the need of conversion from SG to RYGB were also assessed within the selected articles. The results exhibited in this review are purely descriptive. We did not conduct a proper systematic review because there were only small case series published until the time that this article was written, without any robust prospective study.
Results
The initial database search found a total of 388 articles. After the exclusion of duplicates and title and abstract screening, 339 studies were excluded. From the 45 remaining articles, 28 studies were excluded after full-text screening because they did not meet the eligibility criteria. Seventeen articles were then included in the final analysis. Figure 1 summarizes the process of selecting studies.
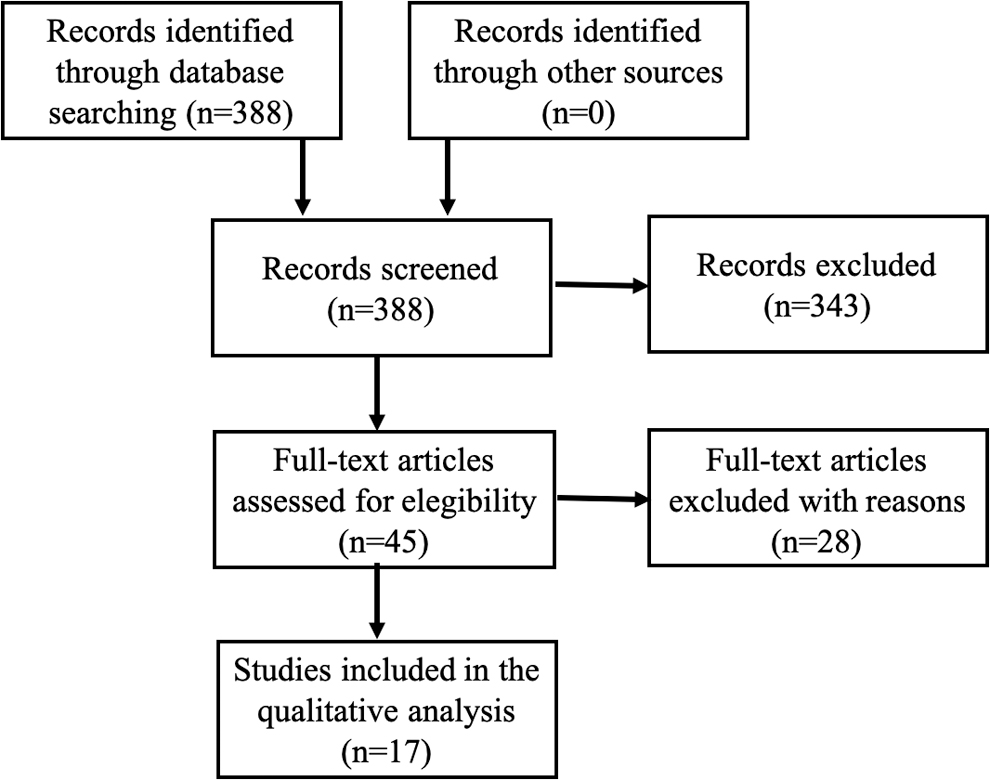
Flowchart of the study selection.
The 17 included studies comprise 296 cases of gastric fistula following SG (acute and late presentations) treated with endoscopic stents of different types. The great majority of patients presented symptoms related to the presence of the stent, including nausea, bilious vomiting, and chest pain. The migration rate varied from 0% to 60%, highlighting an important heterogeneity among the studies. There were two cases of death directly related to the stent (one due to severe bleeding and the other due to esophageal perforation). The overall success rate of the endoscopic stents in treating gastric fistula after SG among the included studies varied from 65.4% to 100%.
Table 1 summarizes the detailed data regarding all results regarding the endoscopic management of gastric fistula after SG from each of the 17 studies that were selected for this review.
Characteristics of the Included Studies
GEJ, gastroesophageal junction; NR, not reported; RYGB, Roux-en-Y gastric bypass; SEMS, self-expandable metallic stent; SEPS, self-expandable plastic stent.
Discussion
In the retrospective series of Alazmi et al., 19 patients who had fistula after SG were studied. 14 The initial approach for all patients was laparoscopic intervention with cavity drainage associated with broad-spectrum antibiotic therapy. After clinical stabilization, the patients were submitted to endoscopic intervention with apposition of self-expandable stents. This procedure was divided into two different steps: first, the metallic stent was implanted and kept for approximately 6–8 weeks. Within 2 weeks remaining for the stent removal, a plastic stent was implanted inside the metallic stent. The author justifies that the utilization of the plastic stent with radial force would help in the further removal of metallic stent by reducing the local inflammatory reaction. Both stents were removed at the same time. In case of persistence of the fistula, a new stent was implanted for 4 more weeks. If still refractory, a conversion to RYGB should be performed. They achieved a success rate of 76% with this treatment protocol. It is important to observe that patients who were submitted to the endoscopic insertion of stents within the first 7 days after fistula diagnosis reached a success rate of 100%. After that time window, the rate of success would decrease down to 50%. These findings highlight the importance for early intervention in these cases. 14
In the study of Almadi et al., 64 patients who underwent endoscopic insertion of partially covered self-expandable metallic stents (PCSEMS) and fully covered self-expandable metallic stents (FCSEMS) for the treatment of gastric fistula after SG were studied. 15 Two deaths occurred: one due to pulmonary embolism and the other due to hypovolemic shock secondary to an aorto-esophageal fistula that was developed 35 days after the insertion of a PCSEMS. Despite this adversity, the authors observed overall better results with the PCSEMS over the FCSEMS, including shorter time for fistula resolution, less need for further endoscopic sessions, and lower stent migration rates, however, with more technical difficulty in its removal. The authors state that the FCSEMS, due to its easier removal, can be a good choice for patients who have difficulties in follow-up. 15
De Aretxabala et al. studied eight patients who developed fistula after SG, among which, only four were submitted to stent insertion. 16 One patient required removal of the stent after 30 days due to the constant migration, despite repositioning. The other patients remained with the stent for 6 weeks. One of these patients presented esophageal stenosis and needed endoscopic esophageal dilation. The stents were placed within 15 days of the diagnosis of fistula, except in one patient, who had the stent implanted 9 months after diagnosis, as an adjuvant treatment. The authors reinforce the need for satisfactory drainage as a fundamental part of therapeutic success and highlight the importance of the stent in accelerating reintroduction of oral nutrition and hospital discharge. 16
A case series by Fishman et al. included 26 patients with gastric fistula after SG treated with endoscopic stents. 17 The duration of the treatment was individualized based on drainage output, the aspect of the secretion, and the patient's tolerance to the stent. The stents were removed within an average of 28.2 ± 18.4 days. The clinical resolution was achieved in 65% of the sample; however, considering only the cases in which technical success was obtained (stent maintenance for more than 2 weeks without evidence of intolerance)—which represents 80.8% of the sample, a complete resolution of the fistula was achieved in 85.0%. Therapeutic failure occurred in nine cases and conversion to RYGB was required in two of them. Among these nine patients, five were considered technical failure, with premature removal of the stent: four with severe reflux and retrosternal pain and one with severe duodenal ulcer hemorrhage. Migration occurred in 27% of the cases. 17
Garofalo et al. studied patients with fistula after SG treated with PCSEMS (n = 5) and fully covered self-expandable megastents (n = 6). 18 It was observed that the PCSEMS failed in three cases. The authors attribute the lack of success to the stent length since it does not exceed the incisura angularis, resulting in an insufficient reduction in the intragastric pressure. In the three cases of failure, the authors proceeded with the introduction of longer stents and achieved therapeutic success. One advantage of the megastent is due to its larger size, which makes migration more difficult to happen; another advantage is the easy removal. All their patients had pigtail drains internally implanted, which remained for 3 weeks before being removed together with the stent. 18
Juza et al. managed gastric fistula after SG with a combined approach, laparoscopic and an endoscopic with insertion of self-expandable stents, in the same operative time. 19 All patients were submitted to, at least, three endoscopic sessions due to stent migration or persistent leakage. The average time of permanence of the stents was 29 days. This shorter length of stay of stents was probably due to the early diagnosis and intervention. 19
In the series by Klimczak et al., 14 patients who had a fully covered megastent implanted to treat gastric fistula after SG were selected. 20 Two complications resulted from the stent: one esophageal perforation and one ulceration. The authors advocate the use of this model of stent due to the easy positioning and coverage of the entire staple line. Although megastents are theoretically related to lower migration rates due to its size and diameters, in the aforementioned study, further endoscopic sessions were necessary to reposition migrated stents in six patients. The cure rate observed was 90.2% with an average time of resolution of 34 days. The average length of stay of the stent was 32 days. 20
Martin Del Campo et al., in a cohort with 24 patients in the postoperative period of SG, used fully covered stents to treat gastric fistulas. 21 The average time of stent permanence was 28.8 days. A migration rate of 22% was observed. A fact that draws attention in this study is the high rate of chronic fistulas. The author observed increased time of hospitalization in this group, in addition to a lower success rate with the endoscopic stents. In these refractory cases, other therapeutic modalities were tried such as balloon dilation, fibrin glue, and clips. Another consequence of this sample profile (fistulas of late presentations) was the high rate of conversion to RYGB (n = 5). Based on their results, the author suggests that the endoscopic therapy should be abandoned at the expense of surgical treatment in cases of chronic fistulas. 21
Moon et al. included 15 patients diagnosed with gastric fistula from a total of 539 patients submitted to SG. 22 The authors advocate that fistulas of acute presentation with <1.0 cm in size should be primarily managed with surgical glue and hemoclips. In the group submitted to the auto-expandable stent insertion, the success rate after the first stent was ∼50%. Two patients needed conversion to RYGB due to the failure of endoscopic approaches. 22
Montuori et al. 23 studied six patients with gastric fistula after SG, using the treatment algorithm published by Rosenthal et al. within the International Sleeve Gastrectomy Expert Panel Consensus Statement. 24 Fistula resolution was achieved in all cases and stent migration occurred in 50% of the sample. The authors did not recommend the suture of the fistulous orifice in cases where there was indication for the surgical approach. They advocate that the aim of this intervention must be limited to peritoneal toilet, collection of material for culture and drainage. They conclude, in addition, that the intervention with endoscopic stents was safe and effective in their small sample. 23
In the study by Nedelcu et al., 19 patients with fistula after SG were submitted to laparoscopy for peritoneal toilet and, subsequently, to an endoscopic approach. 25 They were divided into two groups according to the size of the fistula and the presence or not of distal stenosis. It was observed that fistulas with >1 cm in diameter seemed to benefit more from the stent than fistulas <1 cm. The average time for fistula resolution was 3.4 months and the success rate was 100%, with no case of therapeutic failure or death. 25
Nimeri et al. followed 14 patients who developed fistula after SG. Among these, only four were submitted to endoscopic stents. 26 The implantation of the stent was indicated in cases where stenosis or gastric twist were present. The authors recommend the surgical approach for cavity drainage and creation of a jejunostomy. They reinforce that key points for the treatment are the establishment of enteral nutrition (through jejunostomy) and correction of stenosis sites. An interesting fact in this study is the high rate of therapeutic failure with endoscopic stents (84.6%), which is possibly due to the high prevalence of fistulas of late presentation. 26
In the study by Quezada et al., 19 patients were selected to analyze the early approach of gastric fistulas with the use of fully covered stents. 27 They were divided into two groups: the first group consisted of patients submitted to reoperation or stent implantation at the moment of fistula diagnosis and the second group consisted of patients submitted to surgical drainage or percutaneous drainage and, posteriorly, if necessary, stent implantation. A shorter time of resolution was observed in the first group, with an average of 50 days until fistula resolution against 109 days in the second group (p = 0.008). The migration rate was 34.0%, probably due to the type of stent that was used. The mean length of stay of the stents was 60 days, mostly remaining more than 6 weeks. 27
In the retrospective study by Simon et al., data about nine patients with fistula after SG were collected between 2009 and 2011. 28 All patients were submitted to surgical approach and cavity drainage associated with stent implantation. The stent used in this study measured 17 cm in size and remained implanted for 6 weeks. Two patients presented stent migration, needing further endoscopic sessions for repositioning. It was observed that patients who had a stent placed within <3 weeks of fistula diagnosis presented a shorter time for fistula resolution (99 days) than those who had the stent placed after 3 weeks of the diagnosis (204 days). 28
Southwell et al. described 21 cases of fistula after SG treated with endoscopic techniques. 29 It was observed that patients who were submitted to an endoscopic intervention within <2 weeks presented a shorter time for fistula resolution when compared to the group of later intervention (61 × 105 days, p = 0.07). Moreover, the group of patients who were submitted to the early endoscopic intervention was hospitalized for an average time of 58.6 days compared to 123.9 days in the group submitted to later intervention (p = 0.001). The study showed a 95.5% success rate with the endoscopic therapy. In the case success was not achieved, surgical conversion to RYGB was performed. 29
The study by Tan et al. involved 14 patients diagnosed with fistula after SG, being 8 of early presentation (<7 days) and 6 of late presentation (>7 days). 30 The average length of stay of the stents was 8 weeks for the early fistulas and 3 weeks for the later fistulas. However, four patients needed early removal of the stent: two cases of migration, one case of bleeding and one case of stent torsion. Given their results, the authors did not recommend the use of endoscopic stents as the first-choice intervention for gastric fistulas and suggest different approaches to be performed, including percutaneous drainage and apposition of a T-drain in the fistula orifice. 30
In Tringali et al.'s retrospective study, 10 patients diagnosed with fistula were analyzed and treated with endoscopic stent implantation. 31 The stents' lengths varied between 18 and 23 cm. Two patients were submitted to surgical approach, three to percutaneous drainage, and the five other patients already had a drain implanted in the primary surgery. The stent was implanted with an average of 50.9 days after fistula diagnosis, generally after surgical or percutaneous drainage. In this study, a cauterization of the margins of the fistulous orifice with argon plasma was also performed and an acellular collagen matrix was placed in extent of gastrocutaneous fistula path (n = 2). All patients developed symptoms related to the stent, as nausea and thoracic pain, managed with symptomatic medications. The stents were removed averagely 36.4 days after implantation, with no complication. Fistula resolution was achieved in 80% of the cases after stent removal. In the two cases where therapeutic success was not achieved—one due to stent migration and one due to the path closure failure, the proposed treatments were the implantation of a new stent and the insertion of a pigtail drain, respectively, with posterior resolution of both cases. Another observed complication was gastric ulceration in the distal border of the stent (n = 2). Moreover, one case presented with esophageal substenosis due to hyperplastic tissue originating in the proximal border of the stent without, however, any clinical repercussion. 31
This review addressed the existing evidence on the use of endoscopic stents to treat gastric fistulas after SG and found a great heterogeneity in the results presented by the literature. Varied combinations of interventions (endoscopic stents with or without surgical or percutaneous drainage), different stent sizes, and nonstandardized time to approach endoscopically may justify the observed heterogeneity. The major limitation of these studies included in this review resides in the relatively small number of patients presented in many of the various studies and the scarcity of standardized approaches. Furthermore, it is difficult to establish solid conclusions regarding the safety and efficacy of endoscopic stents in the treatment of gastric fistulas after SG, in part, due to the great heterogeneity of data presented with the literature.
Conclusion
By the time being, it is possible to conclude that the use of endoscopic stents is related to higher success rates when applied early after fistula diagnosis. To take more solid conclusions and establish the definitive role of endoscopic management of gastric fistulas, it is of paramount importance that bariatric investigators put efforts in promoting randomized controlled trials that include standardized protocols for stent size and length of stay, treatment algorithms, and control groups with cavity drainage without stent implantation.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interests.
Funding Information
This research did not receive any fund from funding agencies in the public, private, or not-for-profit sectors.