
Abstract
Introduction:
Transversus abdominis plane (TAP) blocks are routinely integrated into enhanced recovery protocols. Our pilot aimed to understand institutional TAP block practices, increase utilization, and evaluate postoperative narcotic use and length of stay (LOS) among metabolic and bariatric surgery (MBS) patients.
Methods:
An enhanced recovery protocol was implemented in May 2020 at a single academic center; retrospective review evaluated MBS patients (October 2019–February 2021) with no TAP block, anesthesiology-administered (ANES) TAP blocks, or surgery-administered (SURG) TAP blocks.
Results:
Overall, 313 patients received no TAP (n = 135), ANES TAP (n = 32), or SURG TAP (n = 146). After pilot initiation, average monthly TAP block administration increased from 34% to 75%. Further provider practice review revealed the average SURG block formulation was denser than the average ANES block along with increased usage of dexamethasone. Postoperative acetaminophen and gabapentin were ordered more frequently in the ANES group, whereas ketorolac was more frequently ordered in the SURG group. TAP block patients had significantly reduced total postoperative opioid use and LOS versus patients with no TAP blocks.
Conclusions:
Previously unknown variation within TAP block practices was identified, allowing for improved understanding and ability to address operational challenges for improvements. Next steps include standardization of TAP block administration and larger data collection efforts.
Introduction
Comprehensive enhanced recovery programs aim to achieve optimal perioperative care in surgical populations; one of the key principles of these programs is to encourage multimodal non-narcotic pain strategies. 1 Enhanced recovery pathways help reduce opioid consumption and hospital length of stay (LOS) and thus have been adopted for use in metabolic and bariatric surgery (MBS) patients.2–4 Further validation and standardization of individual enhanced recovery elements may yield additional gains in efficacy of these pathways as a whole.
Transversus abdominis plane (TAP) blocks are a commonly used non-narcotic adjunct in patients undergoing abdominal surgery. 5 Among MBS patients, TAP blocks are associated with improved pain management, decreased sedation, earlier ambulation, greater patient satisfaction, and decreased opioid consumption.6–8 Incorporation of TAP blocks has been encouraged into routine practice, MBS-enhanced recovery protocols, and opioid reduction initiatives.9,10 However, there remains limited consensus on how to perform this procedure regarding provider role (surgery or anesthesiology), visualization technique, abdominal wall injection site, and anesthetic medication choice. 11
Before enhanced recovery protocol implementation, TAP blocks were performed by the surgical team or an anesthesiology provider in 34% of institutional MBS patients. Therefore, this MBS patient pilot aimed to understand current institutional practices regarding TAP block utilization, increase TAP block administration, and evaluate total postoperative narcotic use and LOS between no TAP block versus TAP block groups, as well as the impact of TAP block administrator (surgery vs. anesthesiology) on these outcomes.
Methods
A retrospective review was performed of patients 18 years of age or older after elective primary or revisional MBS at an academic bariatric center between October 2019 and February 2021. Exclusion criteria included index-related reoperation within 30 days and revisional surgery greater than 5 years from index operation. Our study was exempt by the Institutional Review Board as a local quality improvement initiative and was deemed nonhuman subjects research.
An institutional enhanced recovery protocol for all MBS patients was implemented in May 2020 to help standardize inpatient care after index operations. Concomitantly, a standardized perioperative checklist outlining key elements of the enhanced recovery protocol was deployed, highlighting opioid reduction efforts through use of non-narcotic adjuncts and the use of TAP blocks (Supplement 1). TAP block administration was performed at the discretion of the attending surgeon.
TAP blocks were administered either by a member of the surgical team (attending surgeon, fellow, or resident) intraoperatively at the end of the index procedure or by an anesthesiology provider (attending, fellow, resident, or nurse anesthetist) as a procedure in the immediate preoperative or postoperative period. Nine attending surgeons perform bariatric surgery at the institution, which is either academically affiliated or in private practice. The surgery TAP blocks involved a laparoscopic-guided direct visualization with precise injection sites in the abdominal wall at the discretion of the performing team member, with common techniques, including bilateral 4-point or 6-point patterns, in the upper abdomen with or without additional injection at port sites.
An early adopter of surgeon-performed TAP blocks shared their formulation, which was standardized during protocol implementation as follows: 38 mL of 0.375% bupivacaine with 2 mL of 8 mg dexamethasone. TAP blocks performed by anesthesiology were done under ultrasound guidance with individual provider discretion in selecting formulation and injection site techniques, including a variable amount of bupivacaine with ad hoc additives; the average block contained 29.8 mL of 0.25% bupivacaine with the addition of lidocaine in 37.5%, dexamethasone in 9.4%, or epinephrine in 6.3%. Over 90% of anesthesiology-performed TAP blocks were done in the immediate preoperative period.
Data was retrospectively collected from electronic medical records and the institutional Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP) database. Variables collected were as follows: patient demographics and characteristics, (2) surgeon and operative characteristics, (3) TAP block performer and formulation, (4) postoperative non-narcotic analgesics (ketorolac, acetaminophen, and/or gabapentin), (5) total postoperative morphine milligram equivalent (MME) use, and (6) LOS (days). An electronic dashboard was created to facilitate standardized data collection and dissemination of results. The dashboard was shared at monthly MBS meetings, which included key stakeholders from surgery, anesthesiology, nursing, and administration to maintain transparency regarding TAP block practices.
Descriptive statistics were used for overall patient and surgical characteristics as well as administration of TAP blocks. Total postoperative MME use and LOS were compared across three groups: (1) no TAP blocks, (2) anesthesiology-administered (ANES) TAP blocks, or (3) surgery-administered (SURG) TAP blocks. GraphPad Prism (version 9.0; GraphPad Prism Software, La Jolla, CA) was used for statistical analysis. The Grubbs outlier test was used to assess single statistical outliers per group before completing statistical analysis. Significance was determined at p-value <0.05.
Results
A total of 313 patients were identified across the study period. The patients were grouped as follows: 1) no TAP block (n = 135), 2) ANES (n = 32), and 3) SURG (n = 146). Patient demographics, preoperative medical comorbidities, and surgical approach are displayed in Table 1.
Patient and Surgical Characteristics for Study Period by Intervention Group
Mean ± standard deviation.
ANES, anesthesiology administered; SURG, surgery administered; TAP, transversus abdominis plane.
The monthly percentage of patients receiving TAP blocks increased over the study period with a baseline average of 34% improving to an average of 75% (Fig. 1). The observed increase in TAP blocks was predominantly due to higher utilization among surgeons (Fig. 2). SURG TAP blocks increased from an average of 4 patients a month before enhanced recovery protocol initiation to an average of 12 patients a month. One month after enhanced recovery protocol implementation, 24 patients received a SURG TAP block, which was 89% of total TAP blocks performed and 59% of total patients undergoing bariatric surgery that month.
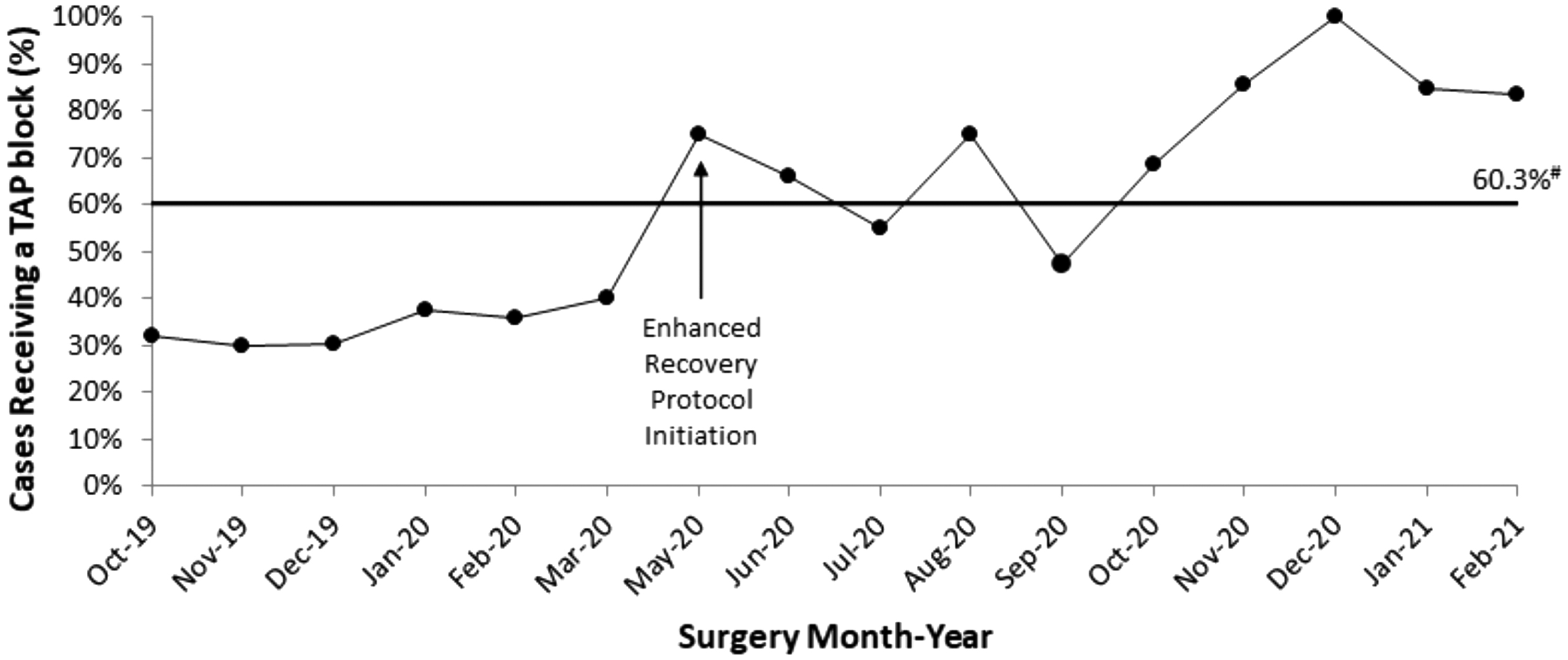
Percentage of cases receiving a TAP block over time. #Median value. TAP, transversus abdominis plane.
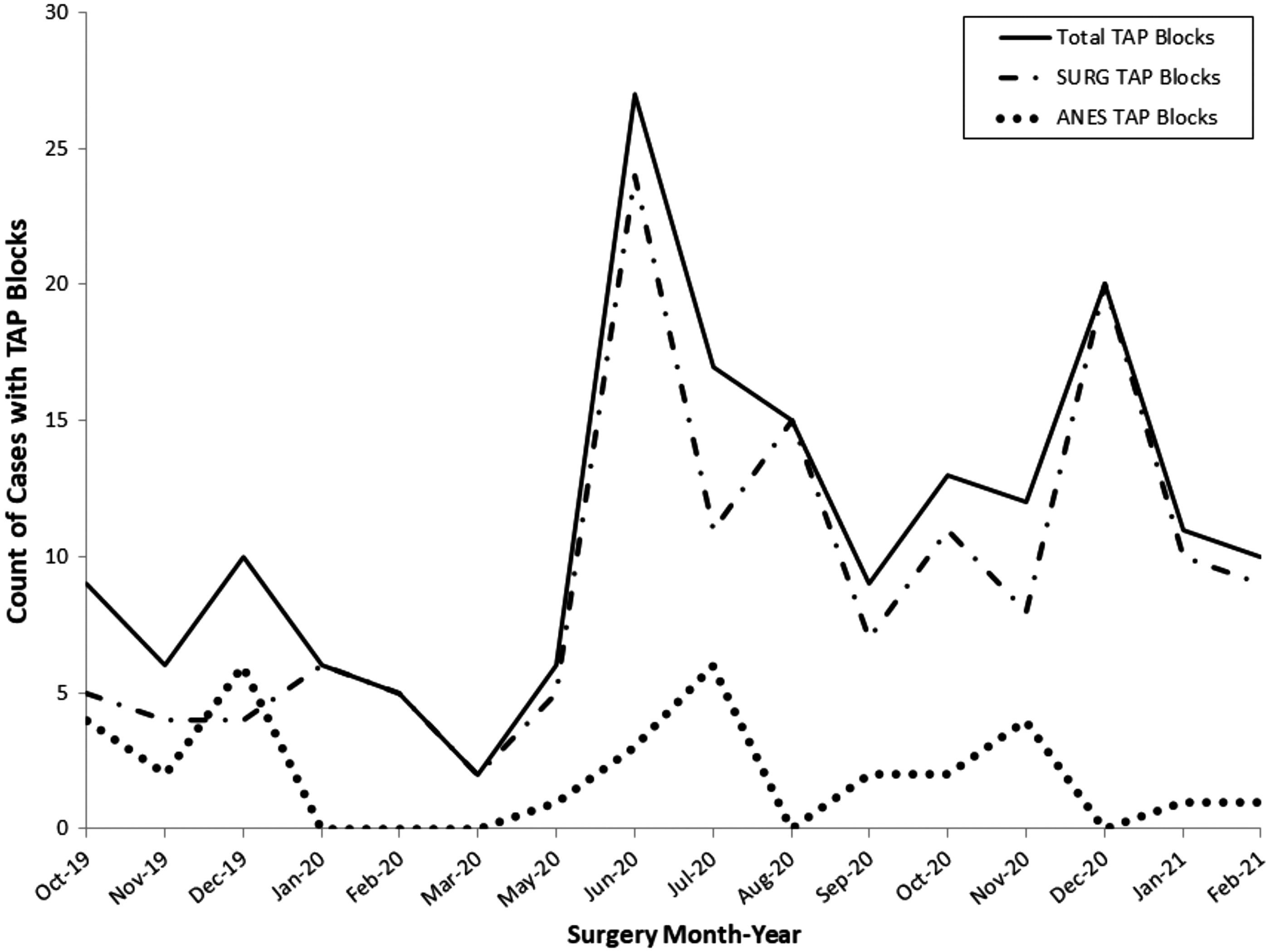
Total number of cases with TAP blocks performed by month. ANES TAP blocks ranged from 0 to 6 patients monthly during the entire study, whereas SURG TAP blocks increased from 2 to 5 patients monthly before enhanced recovery protocol initiation to as high as 24 patients monthly thereafter. ANES, anesthesiology administered; SURG, surgery administered.
In contrast, ANES TAP blocks were administered on average to 2 patients a month, with a range from 0 to 6 patients a month during the entire study. This aligns with our findings at the provider level; before enhanced recovery implementation, four surgeons were performing their own TAP blocks (two routinely and two intermittently); after implementation, seven individual surgeons were performing their own TAP blocks. Throughout the pilot, one surgeon utilized ANES TAP blocks that were performed by 20 different anesthesiology providers.
The use of routinely scheduled non-narcotic pain medications starting postoperative day 0 varied. Acetaminophen and gabapentin were ordered more frequently in the ANES group (87.5% and 81.3%) versus the SURG group (54.1% and 42.5%) and no TAP block group (60.7% and 40.7%). In contrast, ketorolac was more frequently ordered in the SURG group (74.0%) and no TAP group (68.1%) versus the ANES group (43.8%) (data not shown).
Overall, 311 patients were included in the statistical analysis, with two outliers that were removed. Total postoperative MME use and LOS were significantly reduced in patients who received any TAP block (SURG and ANES combined) versus no TAP block. Average total postoperative MME use was 45.7 ± 44.5 in patients receiving any TAP block versus 64.0 ± 51.8 in the no TAP block group (p < 0.001) (Fig. 3A). Average LOS was 1.6 ± 0.8 days (any TAP block) versus 1.9 ± 1.1 days (no TAP block) (p = 0.02) (Fig. 3B). There was a significant positive linear correlation between all patients' total postoperative MME use and LOS (Pearson's r = 0.4885, p < 0.001) (Fig. 3C).
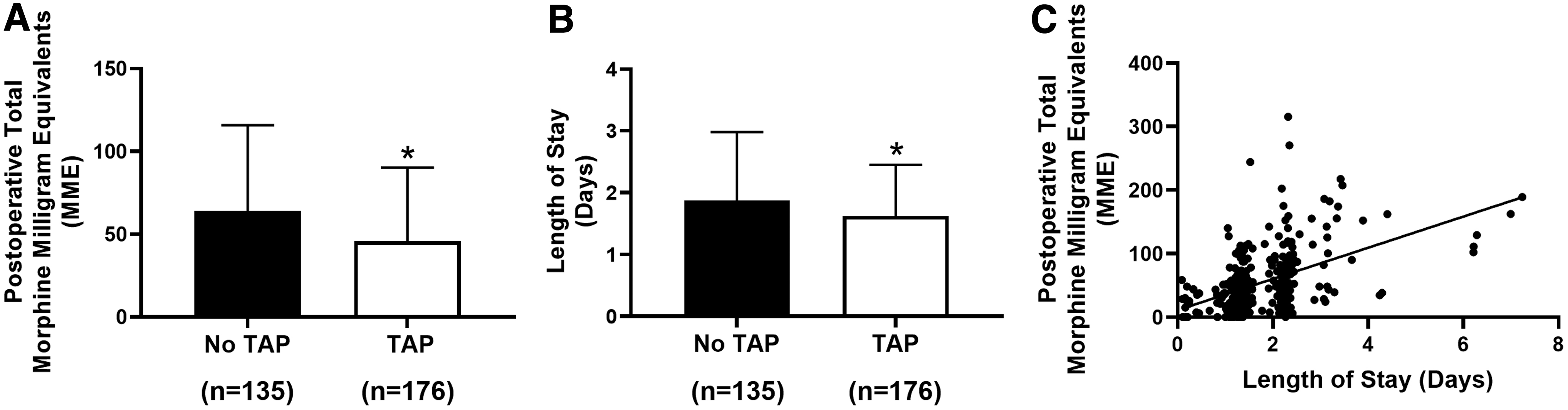
TAP block administration is associated with reduced narcotic use and length of stay in MBS patients. Univariate ANOVA and Fisher's LSD post hoc analysis of no TAP versus any TAP block (SURG and ANES) for
Furthermore, SURG TAP blocks were associated with a significant reduction in total postoperative MME use compared to no TAP blocks (45.1 ± 46.2 vs. 64.0 ± 51.8 respectively; p = 0.001), but not compared to ANES TAP blocks (48.5 ± 36.4; p = 0.7) (Fig. 4A). In addition, SURG TAP blocks were associated with significantly reduced LOS (1.6 ± 0.8 days) compared to both no TAP block (1.9 ± 1.1 days; p = 0.005) and ANES TAP block groups (2.0 ± 0.9 days; p = 0.03) (Fig. 4B). No difference was observed between ANES TAP blocks and no TAP blocks for both total postoperative MME use (p = 0.10) and LOS (p = 0.63). Despite the variability in intraoperative technique, there was no difference in total postoperative MME use and LOS for MBS patients between different surgeons performing SURG TAP blocks.

SURG TAP blocks are associated with reductions in postoperative narcotic use and length of stay in MBS patients. Univariate ANOVA and Fisher's LSD post hoc analysis of no TAP versus ANES TAP versus SURG TAP blocks for,
Discussion
Historically, opioids have been the mainstay therapy for acute pain after MBS. However, wide variations in discharge opioid prescriptions lead to overprescribing, unused opioids after surgery, and increased risk for chronic opioid use postoperatively,12–14 with MBS patients equally susceptible.15–17 Moreover, narcotic-related overdoses continue to have lethal outcomes in over 49,000 Americans annually. 18 Due to the negative outcomes associated with higher doses of prescribed opioids, 19 governing organizations have taken a stance on improving patient safety through opioid reduction initiatives.
In support of these initiatives, the MBSAQIP has recently completed its third nationwide collaborative initiative called Bariatric Surgery Targeting Opioids Prescriptions. This initiative's aim was to reduce opioid prescriptions, while improving postoperative pain control among MBS patients comprehensively by improving education, implementing multimodal pain strategies, reducing perioperative opioid use, and complying with state prescription drug monitoring programs. 10 Collectively, by targeting early opioid reduction interventions, these efforts could mitigate the potential for MBS patients to have accidental overdoses and lethal outcomes, as well as avoiding chronic opioid use.
Our pilot's findings support opioid reduction efforts by increasing the use of regional anesthesia techniques, including TAP blocks, and provide a guide for operationalization. Through our piloted improvement, efforts deploying an enhanced recovery protocol, checklist, and electronic dashboard implementation, as well as increasing stakeholder education and sustained improvement in TAP block administration were observed, mainly attributable to increased surgeon administration. We observed reduced total postoperative MME use and LOS in patients who received any TAP block, regardless of provider, compared to those patients who received no TAP block. In addition, our findings suggested that SURG TAP blocks may be more beneficial, resulting in significantly reduced LOS and a trend toward reduced total postoperative opioid used in MBS patients.
This is not surprising, given the standardized formulation and direct intraoperative visualization of abdominal wall port sites, as well as higher percentage of local anesthetics with routine use of dexamethasone in SURG TAP blocks. However, these practices were not well established or understood before this pilot study. The use of dexamethasone has been associated with improved analgesic effects of TAP blocks. 20 Within the MBS literature, a standardized TAP block protocol is not well established. In other surgical specialty populations, SURG TAP blocks have been shown to be more efficient and provide comparable analgesia to ANES TAP blocks. 21 Thus, exploring the impacts of provider administration and various administration techniques on opioid reduction efforts are critical next steps, which may lead to standardization of TAP block administration.
In addition to TAP blocks, MBS patients routinely received postoperative scheduled non-narcotic analgesics, which may be an important confounder in our study as ketorolac was administered postoperatively more frequently in the surgery TAP blocks, whereas the anesthesiology TAP block patients more frequently received acetaminophen and gabapentin. Notably, previous evidence indicates that among MBS patients, ketorolac use reduces LOS after surgery. 22
Although this pilot focused on increasing overall use of TAP blocks and studied local TAP block practices, reducing MBS patient opioid consumption requires a multifaceted approach. Specifics of TAP block administration and other non-narcotic adjuncts together play a role in a patient's opioid consumption. 23 However, given the quality improvement nature of this pilot study, we did not control the use of multiple non-narcotic pain medications in the perioperative period, but did aim to assess the real-world execution of using TAP blocks in MBS patients.
Moreover, leveraging timely quality improvement efforts through a standardized enhanced recovery protocol and electronic dashboard helped achieve our goal of increasing awareness of TAP block practices and improving block utilization. Despite our achievable increase in TAP block use, an average of 25% of patients were not receiving a block. Quality improvement efforts are ongoing and take time for complete adoption to occur; while our innovators, early adopters, and early majority are onboard with TAP block administration, we continue to educate, engage, and share data to make strides with our late majority and laggards. 24
There are a few additional limitations of this retrospective quality improvement initiative that merit discussion. TAP block group assignments were based on surgeon preferences and did not account for potential patient-level differences. Consequently, the ANES TAP block group had less patients and our findings need to be weighted, bearing the number of observed patients in each group. In addition, important confounders beyond the control of this study included prior opioid use and postoperative non-narcotic pain medication use. Multimodal analgesia was emphasized as part of the implementation, but the postoperative non-narcotic pain medications (acetaminophen, gabapentin, and ketorolac) were prescribed at the discretion of the attending surgeon's preference.
Conclusion
This pilot provides a guide to understanding the influential factors to increasing routine use of perioperative TAP blocks among MBS patients to reduce total postoperative opioid consumption and LOS. We found large variation in local practices between surgery and ANES TAP block formulations and postoperative non-narcotic analgesic use requiring further investigation. Next steps should include multivariate analysis of patient and surgical factors and prospective studies with standardized TAP block injection techniques and formulations, as well as similar postoperative non-narcotic adjuvant use to determine the best way to utilize TAP blocks among MBS patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.