
Abstract
Background:
There is no consensus regarding reversing neuromuscular blockade (NMB) under general anesthesia. For obese patients, complete and rapid recovery from NMB is essential.
Objective:
This study compared the effectiveness of methods to restore spontaneous breathing for obese patients who underwent laparoscopic sleeve gastrectomy after general anesthesia.
Materials and Methods:
Medical records were reviewed for those who underwent laparoscopic sleeve gastrectomy between January 2019 and December 2020. Patients were divided into two groups: (1) reversal of NMB (REV), who received a muscle relaxant antagonist; (2) received nothing (NONE). The REV group had two subgroups: sugammadex (SUG) and neostigmine (NEO). Groups were compared for extubation, recovery, hospitalization after surgery, and total hospitalization times. Major metabolic parameters were evaluated postoperatively at 1 and 6 months.
Results:
Time to extubation, recovery, hospitalization after surgery, and total hospitalization in the REV group were significantly shorter than in the NONE group. Moreover, the extubation time and hospitalization after surgery in the SUG group were significantly lower than in the NEO group. At each postoperative follow-up, both groups were comparable for all metabolism-related indicators.
Conclusion:
SUG was more effective for obese patients who underwent bariatric surgery with general anesthesia. The metabolism of obese patients might not be affected by the means to restore spontaneous breathing.
Introduction
Obesity is increasing worldwide and has become a public health problem due to increased risks of diabetes, hypertension, and coronary heart diseases, which can be better managed by bariatric surgery. 1 The characteristics of obesity are extremely challenging for anesthesiologists, such as a higher risk of obstructed breathing, which might be exacerbated during general anesthesia and paralysis.2,3 Therefore, guidelines for bariatric surgery strongly recommend that anesthesiologists recognize and manage these pathophysiological challenges. 4
When performing surgery for obese patients, especially laparoscopically, surgeons frequently request a profound neuromuscular blockade (NMB) to improve surgical performance.2,4 According to one study, 20–60% of surgical patients who received muscle relaxation agents experienced residual NMB, with an increased incidence of airway obstruction, hypoxemia, atelectasis, and life-threatening vomiting and aspiration.5,6 Moreover, residual NMB was considered an independent risk factor for 24 h postoperative morbidity and mortality related to anesthesia. 7 Therefore, the guideline suggested that anesthesiologists should wholly and rapidly reverse deep NMB at the end of bariatric surgery to ensure no residual NMB. 4
A traditional neuromuscular reversal agent and acetylcholinesterase inhibitor, neostigmine (NEO), has been dominant in the 20th century as an antagonist of nondepolarizing NMB. 8 The cholinergic side effects of NEO include stimulation of the salivary glands, which induce respiratory secretion and other complications and hard-to-reverse deep NMB.7–9 These limit the use of NEO in obese patients. A novel antagonist, sugammadex (SUG), which is a modified γ-cyclodextrin, selectively encapsulates free plasma neuromuscular blocking agent molecules in a one-to-one molecule complex. This will immediately deactivate them, particularly rocuronium, and ensure a rapid and complete recovery from deep NMB in clinical practice. 10 Therefore, SUG is exceptionally suitable for obese patients who need deep NMB for bariatric surgery to reverse deep NMB wholly and rapidly when surgery is completed. 11
There is no consensus on the use of a reversal or a specific agent, which might depend on the condition of the patient, the type of surgical procedure, or even the standard practice of the local hospital. 12 Therefore, this study aimed to determine the methods (e.g., reversal of NMB or spontaneous recovery) to restore respiratory function and their benefits for obese patients who underwent laparoscopic sleeve gastrectomy by evaluating the perioperative and long-term postoperative outcomes.
Materials and Methods
Study design
This study analyzed the medical records of obese patients who underwent laparoscopic sleeve gastrectomy from January 2019 to December 2020 at the First Affiliated Hospital of Jinan University (Guangzhou, People's Republic of China). All data were collected by searching the hospital database.
For this analysis, the patients were allocated into two groups, which were based on whether the reversal agent for NMB was administered after surgery: (1) reversal of NMB (REV), and (2) nothing (NONE, spontaneous recovery or no reversal). Specifically, for the REV group, there were two subgroups: (1) the SUG group received 2 mg/kg SUG as a single dose for the reversal of rocuronium; and (2) the NEO group received 50 μg/kg neostigmine plus 0.02 mg/kg atropine to prevent the cholinergic complications of NEO, which was used for reversal of rocuronium or cisatracurium. 13 Dose calculations for the anesthetic drugs were based on corrected body weight (CBW), which has the formula CBW = IBW +0.4 (TBW − IBW) (IBW = ideal body weight and TBW = total body weight).
This retrospective study was approved by the Institutional Review Board (IRB) of the First Affiliated Hospital of Jinan University (KY-2021-103) and conducted following the Declaration of Helsinki. Informed consent was obtained from all participants.
Patient information
In China, the standard definition of obesity was modified to a body mass index (BMI) of ˃28 kg/m2 by the China Obesity Task Force based on the differences in comorbidity, mortality, and body composition data in the country. 14 In the present study, the inclusion criteria for patients were 18–60 years of age with BMI ˃28 or ˃27.5 kg/m2 and comorbidity ≥1, such as hypertension, diabetes, dyslipidemia, or obstructive sleep apnea (OSA) syndrome. Patients with any of the following conditions were excluded from this study: (1) they had previously undergone bariatric surgery, and (2) had neuromuscular disorders, end-stage renal diseases, congestive heart failure, or cancer.
Each patient in the operating room received standard monitoring of their vital signs, which included electrocardiography, pulse oximetry, end-tidal carbon dioxide, and noninvasive or invasive (if necessary) blood pressure monitoring. General anesthesia induction was started after preoxygenation. All patients used the bispectral index to monitor the depth of anesthesia, and the values were maintained between 40 and 60. At the end of the surgery, the anesthesiologist decided whether to use a muscle relaxant antagonist or not according to the recovery of the obese patient's consciousness and NMB. If they decided to use one, it was administered after skin dressing. Extubation could be performed when patients could follow instructions, such as opening their eyes, and nodding, and SpO2 was maintained at ˃90% in the deoxygenated state. Then, the patient was transferred to the postanesthesia care unit (PACU) for further observation. At Aldrete Score >9, they were transferred to the ward.
Data collection
All data for this analysis were retrieved from the clinical and anesthesia charts in the hospital database. Patient demographics and procedural data, such as patient gender, BMI, procedural time, and anesthesia time, were collected from the electronic medical records. The primary objective of this study was to evaluate the efficiency of recovery between both groups during the patient stay by comparing the following timed outcomes: the need for extubation, recovery, hospitalization after surgery, and total hospitalization. The time required for extubation was from operative skin closure to extubation. Recovery time was from operative skin closure to leaving the PACU. Hospitalization after surgery was from the first day after surgery to the day of discharge. Total hospitalization was calculated as the total number of nights in the hospital.
Follow-ups
The secondary objective was to determine whether the following major relevant metabolic parameters of obese patients in both groups differed during postoperative follow-up at 1 and 6 months. The laboratory data, such as fasting glucose, insulin, hemoglobin A1c (HbA1c), C-peptide, cholesterol (CHOL), total bile acid (TBA), triglyceride (TG), low- and high-density lipoprotein cholesterol (LDL-c, HDL-c, respectively), alanine transaminase (ALT), and aspartate transaminase (AST) were collected from the blood test records at each follow-up.
Statistical analysis
PASS 15 (NCSS, Kaysville, UT) was used to calculate when the number of cases in the SUG group was 153 and the minimum number of cases in NEO was 24 to make the power ˃80%. There were currently 32 patients in the NEO group, >24, so the two groups were comparable. If the continuous data met the parametric assumptions of normality and equal variance by the Shapiro–Wilk test, an unpaired t-test was used to compare the means of both groups. Data were analyzed by a nonparametric Mann–Whitney U test if these assumptions were not met. A chi-squared test was used to compare the gender differences between both groups. Data were expressed as (1) a number if it was a categorical factor or (2) median (interquartile range [IQR]) if the data distribution was not normal, and (3) mean ± standard deviation if it was normal. GraphPad Prism 9 (GraphPad Software, Inc., San Diego, CA) was used for analysis. All tests were two-tailed; p < 0.05 was considered a statistically significant difference.
Results
Participants
A total of 398 patients underwent laparoscopic sleeve gastrectomy in the First Affiliated Hospital of Jinan University (Guangzhou, People's Republic of China) from January 2019 to December 2020. Fourteen patients were excluded from this analysis. Therefore, 384 patients were analyzed. The patients' selection and participant diagram are shown in Figure 1. All 384 patients were allocated to two groups (e.g., REV n = 185 patients and NONE n = 199 patients). A further subgroup was allocated in the REV group, which included 153 patients from the SUG and 32 patients from the NEO groups.
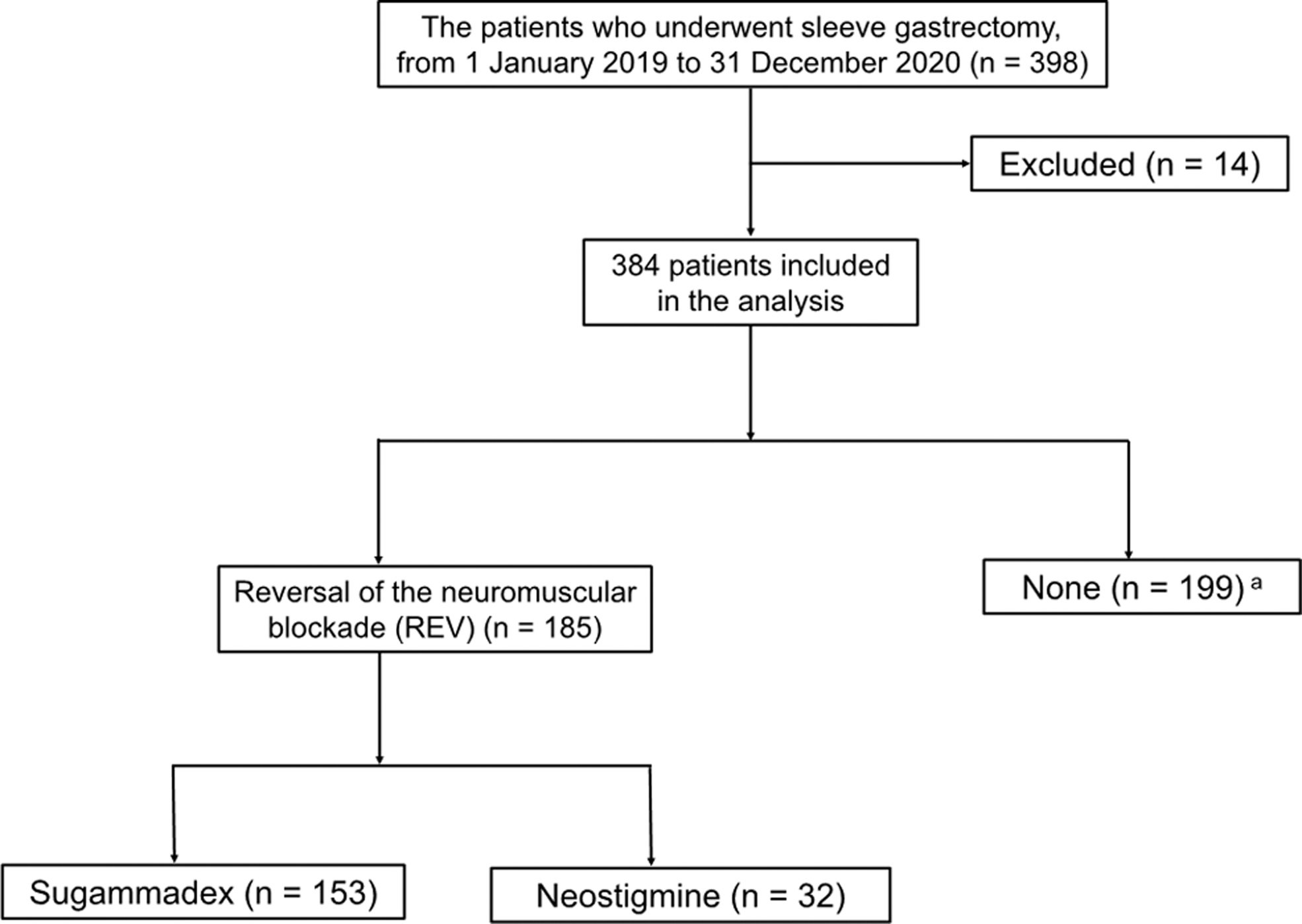
Flow chart of patient selection. aSpontaneous recovery.
The patient's demographic characteristics and procedural factors for the REV and NONE groups are given in Table 1, and the subgroups of the REV group (e.g., SUG and NEO groups) are given in Table 2. The groups were comparable for the demographic's valuables regarding age, gender, BMI, diabetes, OSA, hypertension, gastroesophageal reflux, smoking, and drinking. However, OSA in the REV group was significantly higher than in the NONE group. The total time for the operations and anesthesia of both groups was similar.
Patient Demographics and Procedural Factors for REV and NONE Groups
Values are expressed in median [IQR], or number.
Spontaneous recovery.
BMI, body mass index; GERD, gastroesophageal reflux; IQR, interquartile range; OSA, obstructive sleep apnea.
Patient Demographics and Procedural Factors for SUG and NEO Groups
Values are expressed in mean ± SD, median [IQR], or number.
SD, standard deviation.
Clinical outcomes
Primary outcome
Comparison of REV and NONE
The times to extubation, recovery, hospitalization after surgery, and total hospitalization were analyzed to determine the effect of postoperative recovery for obese patients. The time to extubation in the REV group was significantly less than those in the NONE group (6 min vs. 11 min, p < 0.0001). A significantly faster recovery time was observed (REV vs. NONE, 80 min vs. 95 min, p = 0.02), in hospitalization after surgery (REV vs. NONE, 4 [3.0–4.5] vs. 4 [4–5] days, p = 0.0001), and total hospitalization (REV vs. NONE, 7 days vs. 8 days, p = 0.006) (Table 3). These results indicated that reversal with NMB was faster than no reversal for obese patients who underwent laparoscopic bariatric surgery for their postoperative recovery.
Recovery Efficiency Parameters of the REV and NONE Groups During Hospitalization
Values are expressed in median [IQR], or number.
Spontaneous recovery.
Comparing SUG with NEO
Because two muscle relaxant antagonists were used in clinical practice, a subgroup analysis of the REV group was performed. The extubation time in the SUG group was significantly lesser compared with the NEO group (5.0 min vs. 12.5 min, p < 0.0001). In addition, the same significant difference was found for the hospitalization time after surgery (SUG vs. NEO, 4 [3–4] vs. 4 [4–5] days, p = 0.004). The recovery time in the SUG group was shorter compared with the NEO group (80 [55.0–107.5] vs. 83 [65.0–123.5] min, p = 0.208), but the difference was not significant. The total hospitalization in the SUG group and the NEO group were comparable (7 [6–9] vs. 8 [7–8] days, p = 0.656) (Table 4). The results showed that reversal with SUG was faster and more effective than with NEO.
Recovery Efficiency Parameters of the SUG and NEO Groups During Hospitalization
Values are expressed in median [IQR].
Secondary outcome
Preoperative level
The secondary outcome, major metabolic parameters reflecting carbohydrate metabolism, lipid metabolism, and liver function for obese patients, such as fasting glucose, insulin, HbA1c, C-peptide, CHOL, TBA, TG, LDL-c, HDL-c, ALT, and AST, were collected from the laboratory blood test records. These indicators in the REV and NONE groups (Table 5) and the SUG and NEO groups (Table 6), which were subgroups of the REV group, were similar at the preoperative level. This indicated no significant difference in the preoperative metabolic status of obese patients between groups.
Metabolic Parameters at Baseline (Preoperative) of Bariatric Surgery for the REV and NONE Groups
Values are expressed in median [IQR].
Spontaneous recovery.
ALT, alanine transaminase; AST, aspartate transaminase; CHOL, cholesterol; HbA1c, hemoglobin A1c; HDL-c, high-density lipoprotein cholesterol; IQR, interquartile range; LDL-c, low-density lipoprotein cholesterol; TBA, total bile acid; TG, triglyceride.
Metabolic Parameters at Baseline (Preoperative) of Bariatric Surgery of SUG and NEO Groups
Values are expressed in median [IQR].
Mid-term follow-up
At the 1-month follow-up for the REV group, 170 patients were followed up, and 15 were lost. For the NONE group, 178 patients were followed up, and 21 were lost. In the SUG subgroup of the REV group, 141 patients were followed up, and 12 were lost; in the NEO subgroup, 29 patients were followed up, and 3 were lost. In addition, the medical records for the major parameters of those obese patients were collected. However, there were no significant differences between the REV and NONE groups (Table 7) and the SUG and NEO subgroups (Table 8). These results might suggest that metabolic parameters were not significantly affected by the methods used to restore spontaneous breathing after general anesthesia at the mid-term follow-up after surgery.
Metabolic Parameters 1 Month After Bariatric Surgery for REV and NONE Groups
Values are expressed in median [IQR].
Spontaneous recovery.
Metabolic Parameters 1 Month After Bariatric Surgery for SUG and NEO Groups
Values are expressed in median [IQR].
Long-term follow-up
At the 6-month follow-up, records of 151 patients were collected for the REV group, and 34 were lost. There were 152 patients in the NONE group, while 47 were lost. In the SUG subgroup of the REV group, 126 patients were followed up, and 27 were lost; 25 patients were followed up in the NEO group, and 7 were lost. The results showed no significant differences between the REV and NONE groups (Table 9). The same result was found for the subgroups of REV, between the SUG and NEO groups (Table 10). These results might predict that during long-term follow-up of obese patients 6 months after surgery, the metabolic parameters of the patients did not significantly differ between the groups.
Metabolic Parameters 6 Months After Bariatric Surgery of the REV and NONE Groups
Values are expressed in median [IQR].
Spontaneous recovery.
Metabolic Parameters 6 Months After Bariatric Surgery of the SUG and NEO Groups
Values are expressed in median [IQR].
Discussion
This retrospective study compared the outcomes of two methods to restore spontaneous breathing after general anesthesia in obese patients who underwent laparoscopic sleeve gastrectomy. The results suggested that the reversal of NMB significantly improved perioperative recovery compared with spontaneous recovery. In addition, the reversal with SUG had a faster and better recovery than NEO. For the secondary objective, no association was observed between the use of an antagonist or a specific antagonist and patient metabolism.
Routine muscle relaxant antagonists to reverse NMB at the end of surgery in patients who undergo general anesthesia and receive muscle relaxants remain controversial. Some anesthetists do not routinely use reversal agents due to the associated adverse cardiovascular and respiratory effects.15,16 Our results indicated that for obese patients who were administered an antagonist to reverse NMB at the end of the surgery, the recovery efficacy was significantly higher than no reversal (Table 3). For the time to extubation, this was 1.83 times faster than no reversal. In addition, this was found by other researchers. 17 Obese patients have an increased risk of hypoxia, atelectasis, and other complications. 18 In addition, profound NMB was always required during laparoscopic bariatric surgery, and the incidence of residual NMB for obese patients increased after surgery. 19 Residual NMB easily causes upper airway obstruction, hypoxia, and other respiratory system complications. 20 These findings indicated the importance and use of antagonists to reverse NMB to ensure patient safety and comfort.
The hospital length of stay is considered an important quality metric for recovery from surgery and anesthesia. 21 Our data showed that hospitalization after surgery and total hospitalization duration were significantly shorter for patients who received antagonists than those who spontaneously recovered (Table 3). Some researchers think that residual NMB might occur after extubation in patients with spontaneous recovery because it is not a rapid or reliable recovery. This increased the risk of postoperative pulmonary complications (PPCs) and impaired clinical recovery. 22 Those PPCs, such as pneumonia, atelectasis, empyema, and acute respiratory distress syndrome, are associated with prolonged hospital stays. 5 Patients who receive muscle relaxant antagonists gain a more rapid and predictable reversal, consequently having less residual NMB and fewer complications, leading to a shorter hospital stay. 23
Therefore, a current guideline published in the Journal of Anesthesia recommends that if muscle relaxants are used in obese patients, NMB should be reversed to restore their respiratory capacity before waking them up. 18 Supported by these clinical guidelines, using muscle relaxant antagonists is becoming routine. Moreover, it was reported that the rate of no reversal (spontaneous recovery) gradually decreased for inpatients in the United States, from 64% in 2014 to 38% in 2019. 12 This phenomenon occurred in Europe. 7 Furthermore, a study indicated that for the reversal of NMB cases, SUG was favored over NEO for NMB reversal. 12 Therefore, this study compared whether there were differences in effects between different commonly used muscle relaxant antagonists in clinical practice.
In a systematic review that compared SUG and NEO for their efficacy and safety in adult patients, for moderate NMB, the administered SUG required 2.0 min and NEO 12.9 min. 10 Therefore, SUG was 6.45 times faster than NEO. In addition, this rate of increase could reach 16.8 times for deep NMB. 10 Similarly, in this study, for the subgroup analysis of the REV group, the administration of SUG for obese patients was 2.5 times faster than NEO for the extubation times, which were 5.0 and 12.5 minutes, respectively (Table 4). Therefore, it confirmed the promptness, safety, and effectiveness of SUG for reversing NMB. In addition, this complete and rapid reversal for obese patients is significant when there is an increased risk of pulmonary complications after surgery, such as hypoxia, atelectasis, pneumonia, and respiratory function impairment.2,3
In the present study, the difference in postoperative hospital stays between the SUG and NEO groups was statistically significant (Table 4). A single-center retrospective observational study on abdominal surgery reported that the postoperative hospitalization of the SUG group was 20% shorter compared with the group that received NEO. 24 Similarly, the postoperative hospitalization of patients that received SUG was 6% shorter compared with patients that received NEO after robot-assisted laparoscopic prostatectomy. 25 All these findings suggested that SUG is a more effective reversal agent, which provides reliable, rapid, and complete reversal and accelerates patients' recovery, reducing hospital stay after surgery. 26
This study was limited by a lack of consistent monitoring for muscle relaxation during anesthesia for bariatric surgery. Some surveys have reported occasional neuromuscular monitoring, most of which were qualitative. 27 It is also the current status of clinical use in our hospital. Notably, the COVID-19 pandemic meant that some patients were reluctant to return to the hospital for review. This was the main reason for the reduction in the number of follow-ups. Finally, although our hospital is an international weight loss center, data were collected from a single hospital. Therefore, this retrospective study could not eliminate some confounding factors, and further prospective studies are required to address these limitations.
Conclusion
The findings suggested that SUG provided a rapid reversal from general anesthesia for obese patients after bariatric surgery, with shorter extubation, recovery, and hospitalization times. Reversal of NMB or spontaneous recovery was not associated with long-term metabolic conditions of the patients. The perioperative advantages of reversal antagonists, in particular SUG, in patients' operative recovery might not sustain as metabolic advantages long term. This requires further in-depth multicenter prospective studies.
Footnotes
Acknowledgments
The first author would like to thank the China Scholarship Council for supporting this study abroad for 1 year, and for the opportunity to obtain further skills and knowledge.
Authors' Contributions
M.W. designed the study; acquired, analyzed, and interpreted the data; and drafted the article. S.L., H.J., W.Y., D.H., S.D., and J.T. each acquired and interpreted the data. Y.L. helped with the study designation and approved the final article. All the authors read and approved the final article.
Ethics Statement
This retrospective study was approved by the IRB of the First Affiliated Hospital of Jinan University (KY-2021-103) and conducted following the Declaration of Helsinki. Informed consent was obtained from all participants.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.