
Abstract
Purpose:
In this meta-analysis, we aim to compare the changes in glycemic status of patients without diabetes undergoing sleeve gastrectomy (SG) versus Roux-en-Y Gastric Bypass (RYGB) and the incidence of postoperative hypoglycemia.
Methods:
We included studies from Medline and CENTRAL databases from inception until October 2021 and extracted glycemic outcome values at their furthest follow-up time. The number of participants was 687 from 6 studies.
Results:
The results revealed no significant difference between patients who underwent RYGB and SG in the means of hemoglobin A1c (HbA1c; 95% confidence interval [CI]: −0.07 to 0.11) and fasting glucose (95% CI: −0.12 to 0.02). A significant difference was observed in the means of body mass index (95% CI: 0.66–2.37), fasting insulin (95% CI: 0.92–2.41), and Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) (95% CI: 0.15–0.50) as these measures were lower following RYGB. The pooled prevalence of hypoglycemia was 36% (95% CI: 31–41).
Conclusion:
There was no significant difference in HbA1c and fasting glucose between the two procedures. However, RYGB led to lower insulin levels and HOMA-IR scores.
Introduction
According to the International Federation for the Surgery of Obesity and Metabolic Disorders worldwide survey, sleeve gastrectomy (SG) and Roux-en-Y gastric bypass (RYGB) are the most commonly performed bariatric procedures worldwide. 1 Although RYGB is more effective in the surgical treatment of type 2 diabetes mellitus (T2DM) and the control of metabolic syndrome, it carries the potential for higher short-term complications. 2 Both surgeries, however, remain to be associated with a myriad of complications such as anastomotic leak/stenosis, cholecystitis, nutritional deficiencies, dumping syndrome, and glycemic fluctuations.3–5
Hypoglycemia, a well-documented complication following bariatric surgery, could be severely distressing to patients and can adversely affect their quality of life. 6 It usually occurs postprandially more than 6 months after surgery. 7 Although most patients are asymptomatic, hypoglycemia can present with symptoms ranging from mild to life-threatening complications, such as seizures, syncope, and motor vehicle accidents.7,8 The prevalence of hypoglycemia varies depending on the testing method and the tools used to measure glucose levels; however, it is estimated that the prevalence of postbariatric surgery hypoglycemia ranges from 0.1% to 34%. 9
Previous literature has thoroughly investigated the consequences of SG versus RYGB in patients with T2DM. However, only few articles explored such data among patients without T2DM and no reviews have been conducted on this topic. Given that bariatric surgery is well-known to induce T2DM remission in patients with an established diagnosis, we hypothesized that bariatric surgery in patients without T2DM might result in more frequent glycemic fluctuations particularly hypoglycemia, especially after RYGB because of its effectiveness in T2DM remission.
In this meta-analysis we aim to compare the changes in glycemic markers following SG versus RYGB in patients with obesity and without diabetes, and to observe if it would serve as a predictor for the rate of postoperative hypoglycemia between the different procedures in this population.
Methodology
A systematic review and meta-analysis using the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) recommendations was conducted. 10 The study was registered on the PROSPERO database.
Literature search
A systematic literature review was conducted on the MEDLINE (PubMed) and CENTRAL databases. Terms and keywords such as hypoglycemia, dumping syndrome, reactive hypoglycemia, hemoglobin A1c (HbA1c), fasting blood sugar, random blood sugar, glucose, sleeve gastrectomy, laparoscopic sleeve gastrectomy, gastric sleeve, bariatric surgery, gastric bypass, laparoscopic gastric bypass, and Roux-en-Y gastric bypass were used to conduct the search. The database was searched from inception up to October 2021.
Clinical trials and observational studies that were published in English were included if they compared RYGB with LSG in patients without diabetes and reported pre- and postoperative glycemic measures for our primary outcome. As for our secondary outcome, which was postbariatric hypoglycemia, we included studies for patients without diabetes that underwent either RYGB or LSG and reported number of hypoglycemic events.
Exclusion criteria included nonhuman studies, studies on patients with diabetes only, studies that did not differentiate between patients with or without diabetes, and studies with a follow-up period of <1 month.
Nonclinical studies such as commentaries, letters to editors, editorials, and reviews were also excluded. The chosen glycemic measures were HbA1c, Homeostatic Model Assessment for Insulin Resistance (HOMA-IR), fasting glucose, fasting insulin, and the incidence of hypoglycemia at the longest available follow-up period.
Quality assessment
Risk of bias in clinical trials was evaluated on the outcome level across the studies according to the Cochrane Handbook for Systematic Reviews of Intervention. All clinical trials were assessed for biases in randomization sequencing, allocation concealment, blinding strategies, missing data, and selective reporting using the Risk of Bias 2 (RoB 2) tool. Furthermore, the Newcastle Ottawa Scale (NOS) on the outcome level across the studies was used to assess the quality of cohort and case–control studies.
Data extraction
Two researchers (M.A. and M.I.A.) performed an independent search in MEDLINE (PubMed) and CENTRAL databases screening for relevant articles. After the full-text analysis, two reviewers (A.B. and H.A-A.) extracted the data from the included articles. The extracted data were the following: author's last name, publication year, study design, total number of participants, number of participants within each type of surgery, body mass index (BMI), type of glycemic measurement, pre- and postoperative diabetic status, fasting blood sugar, HbA1c, oral glucose tolerance test, random blood sugar, diabetic score, HOMA-IR, insulin levels pre- and postoperatively, and incidence of hypoglycemia. The longest follow-up period values were used.
Outcomes
The primary outcome was to compare the postoperative changes in BMI and glycemic status between LSG and RYGB including HbA1c (%), HOMA-IR, and fasting glucose (mmol/L) and insulin levels (μU/mL). Secondary outcomes were estimating the incidence of hypoglycemia in nondiabetic patients after bariatric surgeries.
Statistical analysis
A baseline and follow-up model were created for each of the outcomes. To pool the included studies, the random-effects model was used if I2 > 50% and the fixed-effect model was used if I2 < 50%. Furthermore, a separate model was created to assess the prevalence of hypoglycemia among bariatric surgery patients without diabetes postoperatively using the random-effects model with the double arcsine transformation. Meta-XL, version 5.3 (EpiGear International, Queensland, Australia), was used to pool the data from the included studies. The heterogeneity was assessed using Cochran's Q heterogeneity test and I2 statistic.
Results
The search yielded 828 articles and after duplicates were excluded, 752 remained. Reviews, commentaries, editorials, protocols, and irrelevant studies were excluded. The remaining 76 studies were evaluated in their full-text form. Finally, six studies were eligible to be included in the analysis (Fig. 1).11–16 The total number of participants was 687 patients (Table 1).
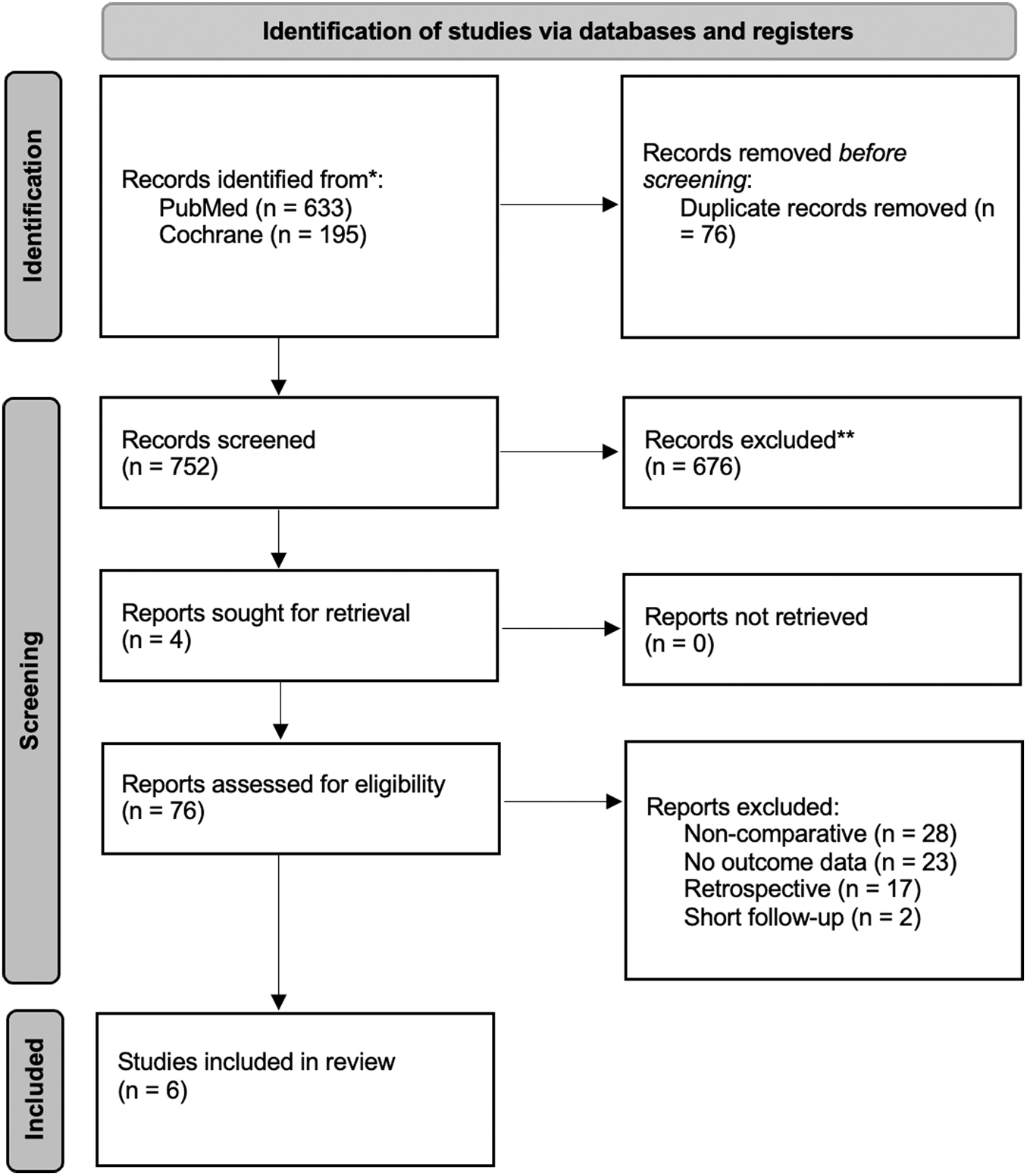
PRISMA flow chart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analysis.
Characteristics of the Included Studies
BMI, body mass index; HbA1c, hemoglobin A1c; HOMA, Homeostatic Model Assessment; LSG, laparoscopic sleeve gastrectomy; MGB, Mini-Gastric Bypass; RCT, randomized controlled trials; RYGB, Roux-en-Y Gastric Bypass; SG, sleeve gastrectomy.
Body mass index
BMI baseline model that included four studies revealed that the mean difference of BMI preoperatively between SG and RYGB patients was not significant (Weighted Mean Difference [WMD] = −0.98; 95% confidence interval [CI]: −3.13 to 1.18); the heterogeneity of this model was significant (I2 = 71%, Q = 10.52, p = 0.01) (Fig. 2).11–13,15 Postoperatively, significant mean difference was noticed between SG (mean = 31.01; 95% CI: 29.81–32.21) and RYGB (mean = 29.45; 95% CI: 28.22–30.68) patients as RYGB patients had lower mean BMI compared with SG patients (WMD = 1.52; 95% CI: 0.66–2.37). The follow-up time used in the included studies ranged from 1 to 2 years. The heterogeneity of this model was insignificant (I2 = 0%, Q = 1.40, p = 0.71) (Fig. 2).
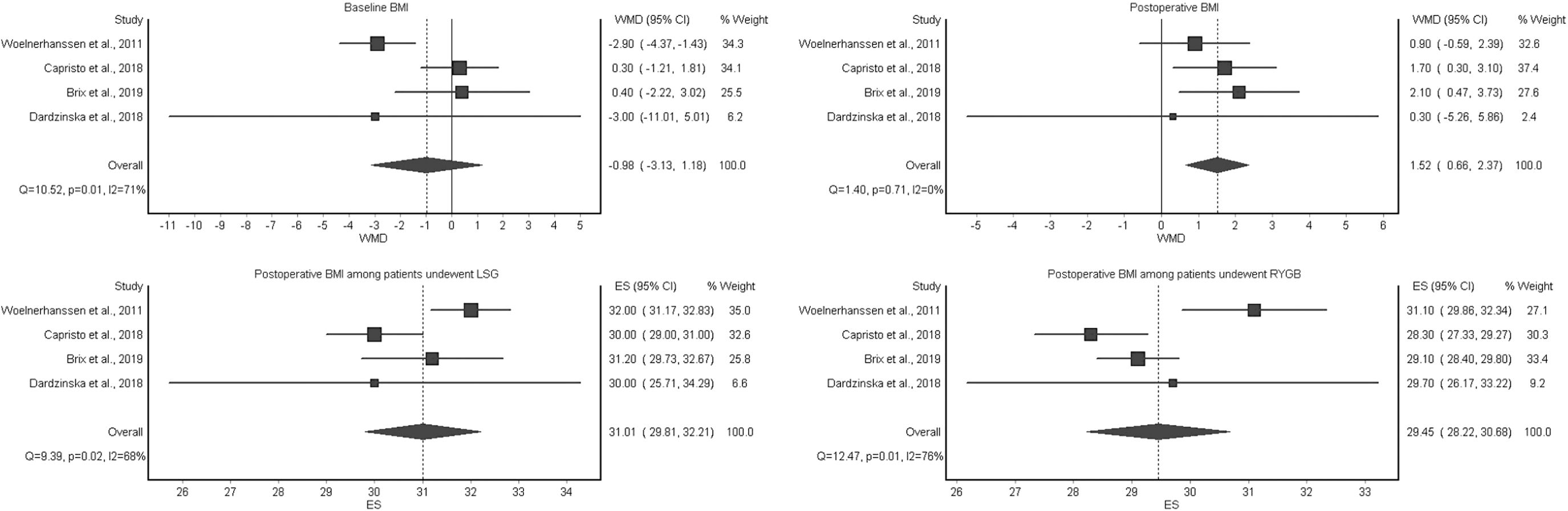
Comparison between SG and RYGB in BMI preoperatively and postoperatively (WMD = SG-RYGB): This figure shows that patients with RYGB and SG were not significantly different in BMI preoperatively. However, patients who underwent SG had significantly higher BMI postoperatively. BMI, body mass index; RYGB, Roux-en-Y Gastric Bypass; SG, sleeve gastrectomy; WMD, Weighted Mean Difference.
Hemoglobin A1c
Baseline and postoperative HbA1c models included three studies.12,13,15 The mean HbA1c difference was insignificant at baseline between the SG and RYGB patients (WMD = −0.04; 95% CI: −0.29 to 0.21); the heterogeneity of this model was insignificant (I2 = 43%, Q = 3.52, p = 0.17) (Fig. 3). Postoperatively, this insignificant mean difference of HbA1c between the SG patients (mean = 5.25; 95% CI: 5.15–5.36) and RYGB patients (mean = 5.19; 95% CI: 4.95–5.43) persisted (WMD = 0.02; 95% CI: −0.07 to 0.11). The follow-up time used in the included studies ranged from 1 to 2 years. The heterogeneity of this model was significant (I2 = 0%, Q = 0.86, p = 0.65) (Fig. 3).
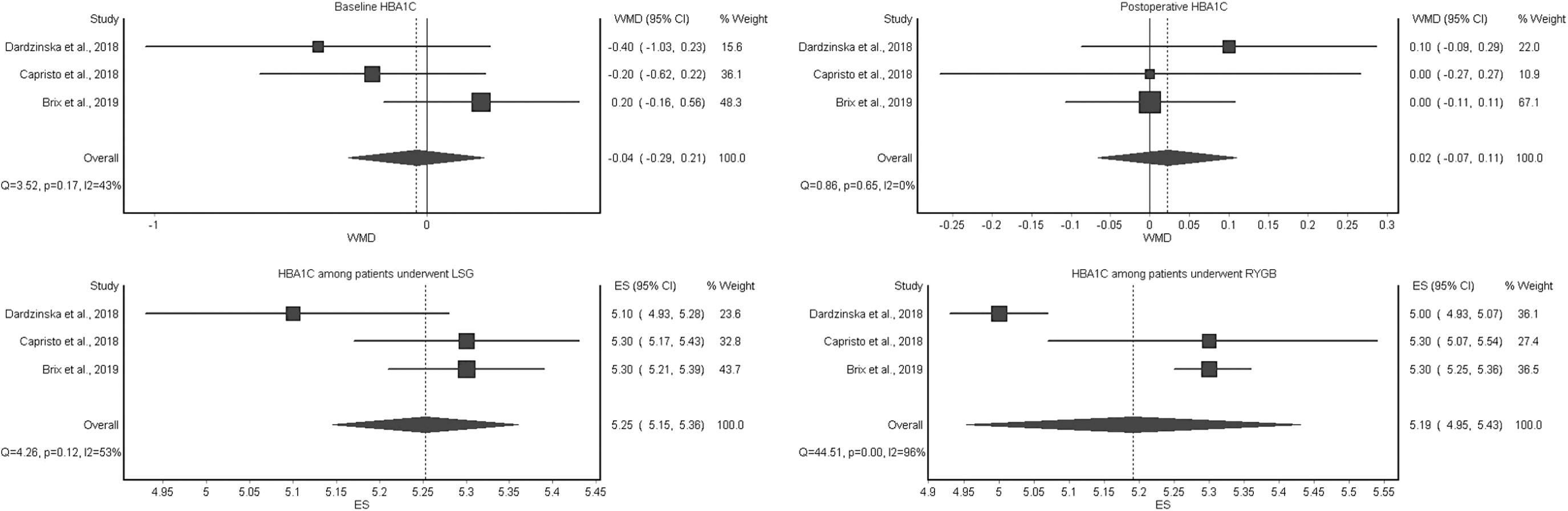
Comparison between SG and RYGB in HbA1c preoperatively and postoperatively (WMD = SG-RYGB). This figure shows that patients with RYGB and SG were not significantly different in HbA1c preoperatively and postoperatively.
Fasting glucose
The fasting glucose baseline and postoperative models included four studies.11–13,15 At baseline, significant mean difference was detected between SG patients and RYBG patients as the mean of fasting glucose was higher in SG patients (WMD = 0.11; 95% CI: 0.02–0.21) (Fig. 4). However, these differences between SG (mean = 4.64; 95% CI: 4.29–4.99) and RYGB (mean = 4.64; 95% CI: 4.16–5.13) patients became insignificant postoperatively (WMD = −0.05; 95% CI: −0.12 to 0.02) (Fig. 4). The follow-up time used in the included studies ranged from 1 to 2 years. Insignificant heterogeneity was detected in the baseline model (I2 = 49%, Q = 5.90 p = 0.12) and the follow-up model (I2 = 46%, Q = 5.55; p = 0.14).
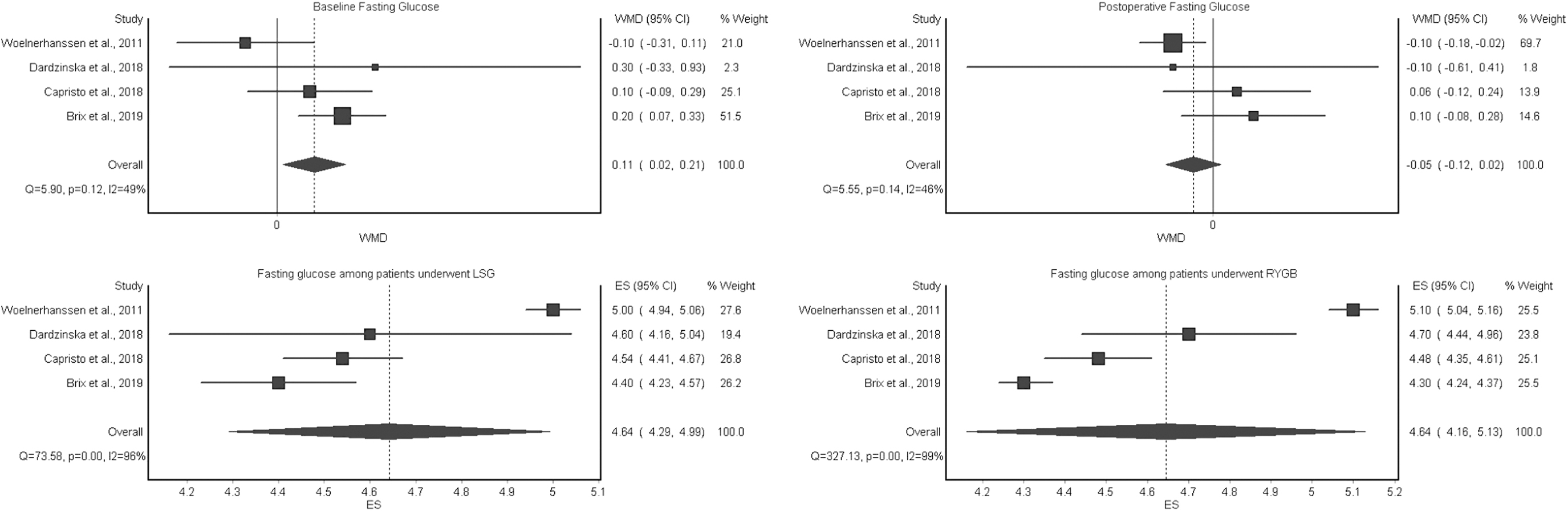
Comparison between SG and RYGB in fasting glucose preoperatively and postoperatively (WMD = SG-RYGB). This figure shows that patients with RYGB and SG were significantly different in fasting glucose at baseline. However, this difference was not significant postoperatively.
Fasting insulin
The fasting insulin baseline model that included three studies revealed that the mean difference of fasting insulin between SG patients and RYGB patients was insignificant (WMD = 1.85; 95% CI: −5.15 to 8.85).11–13 Significant heterogeneity was noticed in this model (I2 = 90%; p = 0.00; Q = 20.12) (Fig. 5a). On the contrary, in the postoperative model, which included the same studies, patients who underwent SG (mean = 10.53; 95% CI: 5.68–15.37) had a significantly higher mean of fasting insulin compared with patients who underwent RYGB (mean = 9.95; 95% CI: 4.93–14.25) (WMD = 1.67; 95% CI: 0.92–2.41). The follow-up time used in the included studies ranged from 1 to 2 years. The heterogeneity of this model was insignificant (I2 = 18%; p = 0.30; Q = 2.43) (Fig. 5a).

Homeostatic Model Assessment for Insulin Resistance
The HOMA-IR baseline model that included three studies resulted in insignificant mean difference between RYGB patients and SG patients (WMD = 0.55; 95% CI: −1.44 to 2.55); significant heterogeneity was detected in this model (I2 = 90%; p = 0.00; Q = 20.63) (Fig. 5b).11–13 However, the postoperative model, which included the same studies, revealed significant difference in the mean of patients who underwent RYGB (mean = 2.04; 95% CI: 0.85–3.23) and SG (mean = 2.15; 95% CI: 0.80–3.50) as patients who underwent SG had significantly higher means of HOMA-IR (WMD = 0.32; 95% CI: 0.15–0.50). The follow-up time used in the included studies ranged from 1 to 2 years. The heterogeneity of this model was insignificant (I2 = 28%; p = 0.25; Q = 2.79) (Fig. 5b).
Prevalence of hypoglycemia
Four studies with 650 patients were included in the analysis of hypoglycemia prevalence.13–16 The pooled prevalence of hypoglycemia was 36% (95% CI: 31–41); the heterogeneity of this model was 43% (Q = 5.24, p = 0.16) (Fig. 6). The follow-up time used in the included studies ranged from 1 to 2 years. None of the four included studies reported the prevalence of hypoglycemia in the RYGB and SG subgroups separately.

Prevalence of hypoglycemia after bariatric surgeries.
Discussion
This review analyzed all available evidence for glycemic changes among patients without diabetes undergoing SG and RYGB. Six studies, with a total of 687 pooled participants, were included in our meta-analysis. Three studies were used for the analysis of BMI, HbA1c, fasting insulin levels, and HOMA-IR, whereas four studies were included in the analysis of fasting glucose levels. Many studies were not eligible for quantitative analysis either because of the lack of comparators or underreporting of clinical values for the nondiabetic group.
Our analysis showed a significant difference in the mean BMI value between SG and RYGB postoperatively, as RYGB patients had significantly lower postoperative BMI compared with their SG counterparts. Such a trend was notable among all the studies included within the quantitative analysis and therefore was expected. Hayoz et al. 17 explored the metabolic differences in randomized controlled trials (RCT) involving SG and RYGB. The meta-analysis found no significant differences in terms of BMI among its pooled cohort at all postoperative follow-up intervals; however, it showed meaningfully significant postoperative BMI differences among a diabetes-only cohort at 12 and 24 months favoring RYGB. Furthermore, an RCT comparing the metabolic changes among patients with diabetes undergoing bariatric surgery demonstrated significantly higher BMI reductions in patients undergoing gastric bypass compared with their SG counterparts. 18
On the contrary, Li et al. 19 conducted a meta-analysis to evaluate the efficacy of RYGB and SG in treating obesity among diabetes nonspecific cohorts and found that both bariatric modalities are indifferent in terms of weight reduction percentages. Such indifference might be owing to the significantly high level of heterogeneity amount included studies. Nonetheless, an 11-year single-center experience of 1146 patients undergoing either RYGB or SG demonstrated significantly higher weight loss among patients undergoing RYGB despite the cohort having a higher percentage of diabetes and a higher initial BMI; however, the differences in weight loss and weight regain between RYGB and SG diminished at the 8-year follow-up interval and beyond, among the small number who followed up. More patients were lost to follow-up in the SG group. 20
We compared glycemic markers including fasting insulin, HOMA-IR, HbA1c, and fasting glucose levels between RYGB and SG pre- and postoperatively at follow-up intervals ranging from 12 to 24 months. Our results showed that the drop in fasting insulin levels and HOMA-IR were significantly higher in patients who underwent RYGB.
With regard to HOMA-IR, Woelnerhanssen et al. 11 prospectively demonstrated the efficacy of both RYGB and SG in improving HOMA index; however, the study did not show a significant difference between the two bariatric procedures. The latter observation is further supported by Dardzińska et al. 12 in which RYGB did not show a significant HOMA-IR difference in comparison with both SG and one-anastomosis gastric bypass.
A prospective study showed that patients without diabetes who underwent RYGB and SG had significantly lower insulin resistance, as measured by HOMA-IR, at a short follow-up period of 6 days. However, the difference between the two bariatric procedures was not significant. 21 A similar trend persisted even within the context of longer follow-ups reaching up to 52 weeks.22,23 As for fasting insulin, available literature indicates that bariatric surgery is effective in lowering postoperative fasting insulin levels; however, no clear distinction between RYGB and SG has been made.11,13
In addition, our analysis revealed that there was no statistically significant change in HbA1c following either bariatric modality in obesity patients without diabetes. Among the included studies, Capristo et al. 15 demonstrated that both RYGB and SG contribute to a significant postoperative decrease in HbA1c. Dardzińska et al. 12 showed that only RYGB contributed to significant lowering of HbA1c in comparison with its SG counterpart. However, this study was conducted on a small sample size (n = 23). On the contrary, Brix et al. 13 reported that both procedures failed to meaningfully impact HbA1c levels in patients without diabetes.
Overall, the aforementioned studies failed to show any statistically meaningful difference in the magnitude of HbA1c decrease between the two bariatric techniques. Similarly, the pooled analysis does not reveal statistically significant differences in fasting glucose levels between either RYGB or SG. Although such conclusions were similarly reported by Capristo et al. 15 the dominant notion throughout the literature supports that bariatric surgery, whether RYGB or SG, results in significant changes in terms of decreasing post-operative fasting glucose.11–13
Furthermore, RCTs that compared patients with diabetes who underwent SG and RYGB showed that RYGB was associated with significantly lower levels of postoperative HbA1c and fasting glucose.18,24,25 In their meta-analysis, Hayoz et al. 17 provided reliable evidence for the superiority of RYGB in terms of decreasing both HbA1c and fasting glucose levels at 12 and 24 months of follow-up among both patients with and without diabetes.
Regarding hypoglycemia, we found that the combined incidence after both procedures was 36%. This incidence rate, while similar to rates reported by Capristo et al. 15 and Rebelos et al. 14 (36.75% and 37.4%, respectively), was higher than that reported by Brix et al. 13 among a strictly nondiabetic population (30%). Meanwhile, a study by Natoudi et al. 16 on patients without or with borderline diabetes following SG demonstrated an incidence rate of 44%.
Fischer et al. 26 found the overall prevalence of postoperative hypoglycemia in patients with and without T2DM to be 38.5%. Of interest, the study also reported that although patients with diabetes had higher pre-and postoperative rates of hypoglycemia, the prevalence in patients without T2DM following RYGB had the most significant increase from baseline rates (2.8–36.4%).
In a nationwide Swedish cohort comprising 5040 patients undergoing bariatric surgery, RYGB was shown to increase the risk of postoperative hypoglycemia by twofold to sevenfold. 27 Such incidence indicates that hypoglycemia is a common complication following bariatric surgery and should be taken into consideration when planning a patient's postoperative treatment regimen and instructions. The implications of such notion are further expanded owing to the negative effect of hypoglycemia on weight loss percentage, which might be possible owing to the diversion of patients' diets toward high-caloric foods. 14 Although able to manifest as a purely asymptomatic disease, hypoglycemia is associated with symptoms ranging from mild, including but not limited to dizziness or general weakness, up to severe manifestations often leading to inpatient hospitalization.13,28
In addition, reactive hypoglycemia owing to glucose dysregulation was reported after both procedures in the included studies. The pathophysiology behind this is multifactorial: anatomical changes, rapid nutrient transit, enhanced incretin effect, early postprandial secretion of insulin and Glucagon-like peptide 1, decreased appetite-stimulating hormones, elevated beta cell mass and enlarged islets, and beta cell function alterations.28–30
It is worth mentioning that hyperinsulinemic hypoglycemia has strong clinical resemblance to the late dumping syndrome. The two main proposed pathophysiologic mechanisms of action are loss of restriction and the hyperinsulinemic hypoglycemia with Nesidioblastosis.31,32 The concept of Nesidioblastosis as reported by Service et al. 32 suggests that the symptoms might be owing to endogenous hyperinsulinemia from abnormal islets and described the performance of partial or total pancreatectomies as a treatment option. This concept has been challenged by Meier et al. 33 who demonstrated that the B cell mass was not increased in those patients compared with those of obese or even lean controls.
This meta-analysis has several limitations. First, the analysis was conducted on studies of observational nature. This inclusion may influence the results by introducing selection bias among treated participants. Second, insulin and HOMA-IR levels exhibited significant amounts of preoperative heterogeneity, which could have impacted the magnitude of their postoperative difference in results. Glucose levels did show moderate heterogeneity in both post- and preoperative models; however, it was statistically insignificant and therefore not of major impact. Reasons for heterogeneity were not explored through any form of sensitivity analysis. Third, the analysis included a moderate number of studies, of which some had questionable statistical power as evident by their low sample sizes. Fourth, secondary outcomes, such as the relative prevalence of hypoglycemia or dumping syndrome, were not included into the statistical models because of lack of sufficient studies or data.
The review was also based on articles produced and published in the English language only, therefore, subjecting the study to language bias. Finally, the study failed to conduct a funnel plot analysis that hindered its ability to detect publication bias or treatment effects.
Conclusion
This systematic review suggests that for patients without diabetes, RYGB has a more profound effect in lowering BMI, fasting insulin, and HOMA-IR compared with SG; however, both are equally effective concerning HbA1c and fasting blood sugar in midterm follow-up. Our analysis did not show that either procedure changed postoperative glycemic markers significantly enough to induce a higher rate of postoperative hypoglycemia compared with the other inpatients without diabetes who suffer from obesity. However, further studies comparing RYGB and SG in patients without T2DM using comparable definitions and specifically looking at postoperative hypoglycemia are much needed.
Footnotes
Authors' Contributions
Study conceptualization and design was performed by M.A.-K., M.I.A., A. A.-A., A.B., and A.H. Literature search and study selection was performed by M.A.-K., M.I.A., A.A.-A., B.M., and H.A.-A. Data analysis and interpretation was performed by A.T., A.A.-A., and H.A.-A. All authors participated in article drafting. Critical revision of the article was performed by A.B. and A.H. All authors read and approved the final version of the article.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Author Disclosure Statement
A.H. is a speaker for Medtronic and Ezisurg Medical. The rest of the authors have no conflicts of interest to declare.
Funding Information
No funding was received for this article.