
Abstract
Abstract
Breastfeeding rates have been improving in the United States. However, current rates, especially those of exclusive breastfeeding and breastfeeding duration, are still below the Healthy People 2010 objectives. Furthermore, gaps in breastfeeding rates continue to exist among different racial and socioeconomic groups. Physician mothers' breastfeeding behavior has been studied because it impacts their anticipatory guidance to their patients, which in turn influences patients' breastfeeding initiation and continuation. In this paper, we review available literature regarding breastfeeding among female physicians in the United States. The current data suggest that female physicians are initiating breastfeeding more often than the general population but their continuation rates are lower. In other words, working as a physician might be a newly identified maternal characteristic associated with low breastfeeding maintenance rates. We also review possible factors that might affect breastfeeding decisions and behaviors of physician mothers. Once modifiable factors are further identified, programs can be suggested and implemented to improve breastfeeding continuation in this newly identified high-risk group.
Background: Importance of Breastfeeding, Goals, and Trends
The Healthy People 2010 (HP2010) initiative recognizes the importance of breastfeeding and its benefits. Initially the objectives set by the U.S. Secretary of Health and Human Services were to achieve 75% breastfeeding initiation rates nationwide at hospital discharge, 50% continuation at 6 months, and 25% at 12 months postpartum. 4 In 2007, HP2010 goals were updated to include two new objectives on exclusive breastfeeding. The new goals are to achieve 60% exclusive breastfeeding rate at age 3 months and 25% at 6 months. 5
The National Immunization Survey (NIS), an annual telephone survey conducted by the Center for Disease Control and Prevention, was designed to collect nationally representative data regarding the noninstitutionalized, U.S. civilian population. 6 Analysis of NIS data shows that the breastfeeding initiation rate was 74% for infants born in 2005. In this population, continuation rates at 6 and 12 months were 43% and 21%, respectively. Of these infants, approximately 32% were exclusively breastfed at 3 months but only 12% at 6 months. 6 These data indicate that while initiation rates are approaching the HP2010 objectives, rates of duration and exclusive breastfeeding in the United States are still below desired levels. Interventions targeted at exclusive breastfeeding and breastfeeding duration are needed in order to achieve the HP2010 goals.
Importance of Studying Breastfeeding Among Physicians
Physician breastfeeding counseling is one of the interventions that successfully increase breastfeeding initiation and duration. 7 A strong predictor of physicians' breastfeeding advocacy is their successful personal or spousal breastfeeding experience.8–11 These observations are consistent with findings by Frank 12 that physicians' personal healthy behavior is a powerful predictor of counseling patients about preventive issues. As such, strategies to enhance breastfeeding in physician families are important, not only for their own breastfeeding success and health of their child, but this behavior may also affect how well they can serve as role models and information sources of breastfeeding for their patients. To date, our understanding of breastfeeding among physicians in the United States has been based on cross-sectional questionnaire surveys administered to residents and/or practicing physicians.13–16
According to these studies, breastfeeding initiation rates among female physicians ranged from 80% to 94%, exceeding the HP2010 goals (Table 1). However, breastfeeding continuation rates at 6 and 12 months were usually below HP2010 objectives, regardless of whether the group surveyed was still in training or not (Table 1). In studies conducted prior to the 80-hour work week mandate, 6-month continuation rates ranged from 15% to 21%.13–15 A more recent study with a smaller sample size found a 6-month continuation rate of 58% among female obstetrics-gynecology and family medicine housestaff in one institution in the post–80-hour work week era. 16 The difference in 6-month continuation rates could be due to differences in sample sizes or be a reflection of impact of maternal work hours on breastfeeding duration. Another possible explanation is association of maternal specialty and breastfeeding duration because specialties such as obstetrics-gynecology and family medicine might be more “family-friendly” than specialties such as surgery that were included in the earlier studies. Breastfeeding continuation rates at 12 months have been much lower than the HP2010 objectives in all studies, ranging from 7% to 8%.13–16 No data, to our knowledge, have been published regarding exclusive breastfeeding among physicians.
Ob/Gyn, Obstetrics and Gynecology; FM, Family Medicine.
Disparity in Breastfeeding
According to existing studies, physician mothers initiate breastfeeding more often than mothers in the general population. However, they usually maintain breastfeeding for a shorter duration (Fig. 1). Therefore, disparities exist between physician mothers and non-physician mothers in the United States.
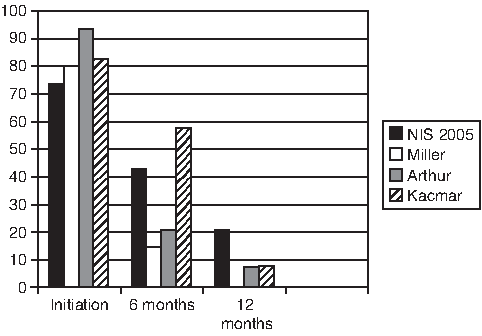
Comparison of breastfeeding rates of mothers in the general population (NIS 2005) and physician mothers at hospital discharge (initiation), 6 months, and 12 months. NIS data from 2005 are used for breastfeeding rates of mothers in the general population. Rates of breastfeeding of physician mothers were obtained from three studies: Kacmar et al., 16 Arthur et al., 15 and Miller et al. 13
Physician mothers are not the only disadvantaged group. While the overall rates of breastfeeding have increased in the United Sates in recent years, significant disparities continue to exist among different racial/ethnic and socioeconomic classes.17–21 The HP2010 initiative calls for elimination of health disparities and an increase in breastfeeding initiation and continuation as well as exclusive breastfeeding rates across all socioeconomic classes.4,5 Attempts to eradicate these disparities have included research to identify infant and maternal characteristics associated with low breastfeeding rates.17–21
Maternal characteristics associated with lower breastfeeding rates include non-Hispanic black race, poverty, young age (less than 20 years), and less than a high school education. 17 In fact, the lowest 12-month breastfeeding continuation rates in 2004 were among mothers less than 20 years (8.6%) and those of non-Hispanic black race (11.9%). 22 Previous research has also suggested that maternal fulltime employment outside home is associated with shorter breastfeeding duration. 23 On the other hand, women employed as professionals breastfeed longer than other working mothers.24,25 Older maternal age, at least some college education, and being above the federal poverty threshold have also been associated with higher breastfeeding initiation and continuation rates. 17 As a group, women physicians possess these characteristics, including professional occupation, high family income (>$25,000), older age (>25 years), and a college education. 26 So the poor breastfeeding maintenance among this group is somewhat surprising.
Even more noteworthy is that breastfeeding continuation rates among physician mothers are generally even lower than previously identified high-risk groups (Fig. 2). In order to improve breastfeeding continuation among this group, we should attempt to identify factors that influence breastfeeding decisions and practices of its members. Existing studies have identified some of these factors (Fig. 3).
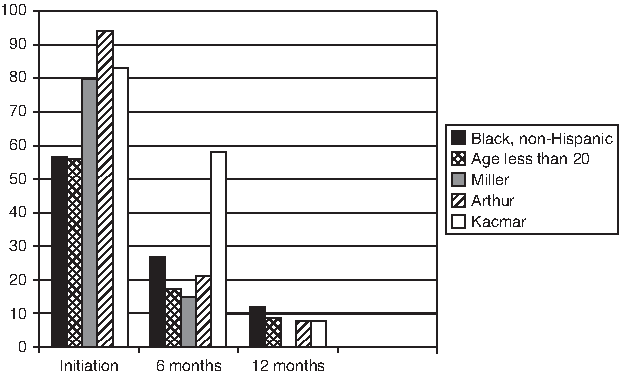
Comparison of breastfeeding rates of mothers in previously defined high-risk groups and physician mothers at hospital discharge (initiation), 6 months, and 12 months. Black non-Hispanic race and age less than 20 years are maternal characteristics associated with low breastfeeding rates. 22 Rates of breastfeeding among physician mothers are obtained from studies by Kacmar et al., 16 Arthur et al., 15 and Miller et al. 13
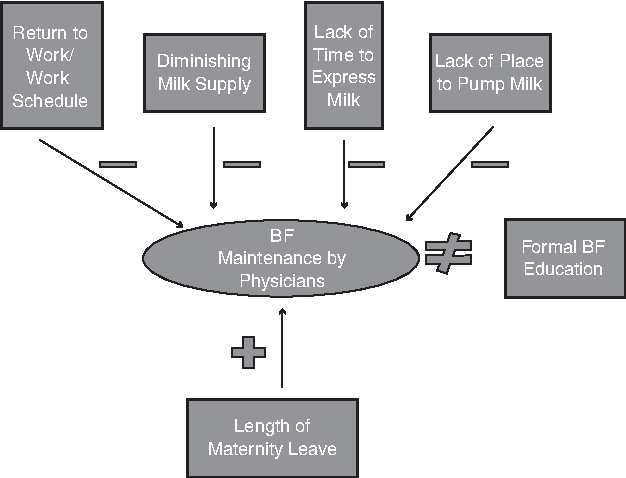
Factors that might affect breastfeeding (BF) duration of physician mothers.
Breastfeeding Among Physicians: Obstacles and Enablers
Miller et al. 13 conducted a national survey by mailing questionnaire surveys to 1,500 female housestaff randomly selected from 1990 graduates of American medical schools. They reported an adjusted response rate of 45% based on an adjusted base of 990. Of 450 respondents, 60 (13%) had delivered a child during residency. The authors defined primarily breastfeeding as providing breastmilk for more than 50% of the infant feedings. Eighty percent of resident mothers who were not primarily breastfeeding by 3 months reported that residency work schedule interfered with breastfeeding or made it impossible. 13 In fact, 50% of resident mothers who had initiated breastfeeding weaned around the time of returning to work from maternity leave. Seventy-nine percent of resident mothers who continued to breastfeed after returning to work felt there was insufficient time during work to express milk, and 42% reported no appropriate place at work for the activity. 13 Only 54% felt supported by their attending physicians and 67% by their colleagues in their breastfeeding efforts. 13
Arthur et al.14,15 surveyed 350 female physicians in Mississippi. They reported a 61% response rate, but only 146 of their respondents had had personal breastfeeding experience. The three major factors that contributed to breastfeeding cessation among these women were return to work (45%), diminishing milk supply (31%), and lack of time to pump (18%).14,15 Obstacles to breastfeeding upon returning to work were similar to those found by Miller et al., 13 i.e., lack of space and time for milk expression.14,15 Only 14% reported expressing milk in a “designated room,” while 64% had used a private office to express milk, 25% a call room, 19% a restroom, 5% a car, and 5% other locations. 14 On the other hand, a statistically significant positive association was found between the length of maternity leave and breastfeeding duration, but only for the first- and second-born children. 14 These findings are consistent with studies in the general population that have found a highly significant association between length of maternity leave and duration of breastfeeding. 25 Interestingly, the association between length of maternity leave and breastfeeding duration was not significant for third and fourth children of female physicians. 14 However, duration of breastfeeding was consistent among children for each respondent. The authors hypothesized that these findings can be explained by the impact of mother's experiential learning on future breastfeeding behavior. 15
Kacmar et al. 16 surveyed 66 male and female housestaff in departments of family medicine and obstetrics/gynecology at Brown Medical School. Only 15 respondents were parents. Consistent with previous studies, they found excellent initiation rates for both female physician mothers and spouses of male housestaff (93% overall, 83% of female housestaff, and 100% of male housestaff spouses). However, only 8% of resident physician mothers were breastfeeding at 1 year, compared to 50% of spouses of male resident physicians. 16 Since this study did not report data about spousal occupation, conclusions cannot be made regarding the impact of work status and workplace on breastfeeding continuation from its results alone. However, research in the general population has shown that while fulltime work does not affect breastfeeding initiation, it does significantly affect its continuation and duration. 25 In fact, return to fulltime employment outside of home within a year after delivery has been identified as a barrier to breastfeeding in the general population.24,26,27
Conclusions
Breastfeeding rates have been improving in the United States. However, current rates, especially those of exclusive breastfeeding and breastfeeding duration, are still below the HP2010 objectives. 6 Furthermore, gaps in breastfeeding rates continue to exist among different racial and socioeconomic groups.17–21
Physician mothers' breastfeeding behavior has been studied because it impacts their anticipatory guidance to their patients, which in turn influences patients' breastfeeding initiation and continuation.8–11 Review of available literature suggests that female physicians are initiating breastfeeding more often than the general population. However, their continuation rates are lower than the general population (Fig. 1). It would have been interesting to compare breastfeeding behavior of physician mothers with other professional mothers, such as lawyers or scientists, with long and stressful hours. However, no such data have been published to date. Nonetheless, working as a physician seems to be a newly identified maternal characteristic associated with low breastfeeding maintenance.
Based on excellent breastfeeding initiation rates observed among female physicians, it is possible that education and occupation play important roles in their decision to start breastfeeding. However, poor duration rates among the same population imply that these characteristics alone are not sufficient for breastfeeding maintenance. Based on results of current literature, modifiable factors that might affect breastfeeding duration of physician mothers include length of maternity leave, protected time and space for milk expression when mothers return to work, and support and reinforcement at the work site (Fig. 3). Programs to promote breastfeeding duration need to be implemented and evaluated among this population. 28 These programs might be easier to implement and study first among housestaff and include part-time employment opportunities, longer paid maternity leave, child care and lactation facilities in the workplace, and educational campaigns to promote workplace recognition and awareness that breastfeeding for the first 6 months is optimal. Improving breastfeeding among physicians is important not only for the well-being of their children, but also for enhancing their efficacy as breastfeeding advocates for their patients.
Breastfeeding advocates have argued that public health programs to promote breastfeeding should especially target the high-risk groups with the lowest breastfeeding rates. These advocacy efforts should then include physician mothers who might have been overlooked so far because of their professional and medical background. More investigation is warranted to further identify factors other than education that can affect breastfeeding decisions of physicians. Better characterization of these factors will potentially allow for endeavors to improve breastfeeding practices of not only physician mothers, but all mothers in general, and will be paramount to the development and implementation of successful practices and programs that increase rates of breastfeeding and realization of HP2010 objectives.
Footnotes
Disclosure Statement
No competing financial interests exist.