
Abstract
Abstract
Background:
In order to ascertain any bacterial contamination of donor human milk, we cultured milk samples both before and after Holder pasteurization.
Methods:
During 2003, all frozen donor milk samples were thawed and aseptically placed in pools prior to pasteurization. All individual and pooled samples were cultured and incubated for 48 hours. Specific microbiologic identification of group B Streptococcus, Staphylococcus aureus, coagulase-negative Staphylococcus, α-Streptococcus, Enterococcus, and Bacillus sp. was performed. Gram-negative rods (GNRs) were subtyped but not specifically identified. Positive cultures were expressed in quantitative colony counts.
Results:
Samples from 303 pools and 810 individual mother's donor milk were cultured. Forty-four pools (15%) represented “preterm donor milk” from milk donated by mothers who delivered prior to 36 weeks of gestation. Before pasteurization, 185 pools (62%) grew at least one lactose-fermenting GNR, and 58 pools (19%) grew a second lactose-fermenting GNR. Forty-four percent grew a non–lactose-fermenting GNR, and 20% grew an oxidase-positive GNR. The majority (87%) were colonized with Staphylococcus. Other Gram-positive organisms identified included Enterococcus (16%), α-Streptococcus (8%), and S. aureus (4%). Only one milk sample was positive for methicillin-resistant S. aureus. The majority of pooled milk samples grew two or more organisms. Milk from 22% of mothers did not grow detectable bacteria on routine cultures. The bacteriologic colonization profiles of milk from mothers delivering prematurely were similar to those of mothers delivering at term. After routine Holder pasteurization of donor milk, 93% of milk samples showed no growth on routine bacterial cultures.
Conclusions:
A wide variety of bacteria contaminate human milk from donor mothers. Most milk samples grew coagulase-negative Staphylococcus and Gram-negative organisms. Although normal skin flora was cultured typically from milk samples, there were also many prepasteurization milk samples contaminated with pathogenic organisms. Holder pasteurization was, however, an effective means by which to remove any detectable bacteria from samples of donor human milk.
Introduction
It is well known that premature infants cared for in the neonatal intensive care unit (NICU) fare better on human milk feedings. Human milk feedings are especially critical for premature infants, who are at a greater risk for acquiring necrotizing enterocolitis (NEC) if they are fed formula instead of human milk. Nearly 10–12% of formula-fed extremely premature infants will acquire NEC. In contrast, studies have shown that fewer than 2–4% of premature infants fed mother's milk will acquire NEC.13,14 Research has shown that medical care for NEC increases a baby's length of hospital stay by nearly 2 weeks at an additional cost of $125,000–250,000 (in 2002 dollars). 15 In addition, it has been shown that fewer human milk-fed preterm babies develop nosocomial sepsis compared to formula-fed babies.13,16,17 Feeding human milk results in shorter hospital stays for preterm infants and has generated both short- and long-term healthcare cost savings.8,9,13 Pasteurized donor milk for premature infants has been shown to reduce the incidence of NEC, sepsis, and infection, resulting in shorter hospital stays.13,16–20 Fortunately, some of the bioactive properties found in human milk remain viable after storage and pasteurization.21–24
The Mothers' Milk Bank at Austin (MMBA) in Austin, TX is a nonprofit organization that accepts donations of surplus milk from healthy breastfeeding women and pasteurizes and dispenses donor human milk, primarily to premature and ill infants. MMBA is a member of the Human Milk Banking Association of North America (HMBANA). In order to provide a safe product, processing and dispensing of human milk are done in accordance with the guidelines from the HMBANA. 25 Currently, HMBANA guidelines recommend that heat treatment of milk by Holder pasteurization occur before any donor milk can be fed to babies. Holder pasteurization has been thought to eradicate any (pathogenic) bacterial contamination.
Since the milk bank's opening in 1999, MMBA has dispensed donor human milk to various outpatients and to NICUs located not only in Texas, but also throughout the United States. During the calendar year of 2003, more than 300 mothers were approved to donate their milk, and MMBA dispensed over 120,000 ounces of milk to 18 hospitals and 34 outpatients. The goal of this study was to document the effectiveness of our pasteurization process by testing for any bacterial contamination and confirming the absence of any detectable bacteria in our pasteurized donor milk. In this study, we also sought to obtain bacteriological surveillance of all donor human milk samples submitted to MMBA throughout one calendar year. We wanted to describe the nature of bacterial contamination of donor human milk and to examine whether donor milk from mothers who delivered prematurely was more often colonized with pathogenic organisms than milk from mothers who delivered at term.
Subjects and Methods
All volunteer donor mothers completed a written health questionnaire and submitted to numerous serological blood tests (similar to those used in the screening process by blood banks in the United States), which were repeated every 6 months. Donor mothers answered specific questions about possible infectious diseases, medical history, lifestyle, and behavioral risks. Their baby's doctor validated his or her health and the mother's fitness as a donor prior to her approval as a human milk donor. Donor mothers provided written informed consent for use of their milk for clinical and research purposes. “Preterm donor milk” came from mothers who delivered before 36 weeks of gestation and was expressed throughout the first month postpartum. Donor mothers were instructed to wash their hands thoroughly with antibacterial soap; however, the breast was not specially cleansed or treated before milk collection. Milk was obtained by either hand expression or manual or electric breast pumps. Donors were not specifically instructed to discard the first portion of milk expressed. Milk samples were placed into sterile, hard plastic containers or flexible plastic milk collection bags and frozen in the donor's home freezer at a maximum of 0°C. No special instructions were given to keep the frozen milk near the rear of the freezer. All milk samples were transported to the milk bank, frozen, and maintained in freezers at −20°C for up to 6 months. Mothers with (symptoms of ) mastitis were excluded from donating milk until approximately 2 days after completion of a course of antibiotics lasting from 1 to 3 weeks.
Prior to pasteurization, frozen milk samples were thawed in batches at room temperature, then refrigerated, and later aseptically placed into pools. One to four donors contributed milk to each pool. Before processing, samples from each individual mother's milk were obtained and sent to the St. David's Hospital microbiology laboratory in Austin, TX. Glass bottles filled with pooled milk were placed in a shaking water bath preheated to 62.5°C. When the water regained a temperature of 62.5°C, the process was held for 30 minutes, with frequently check of the temperature and water movement in the bath. Constant motion was provided to keep the temperature inside the bottles at the same temperature as the bath. The milk was then rapidly cooled in an ice bath prior to being refrozen for storage and dispensation. After pasteurization (prior to storage) all pooled milk samples were cultured. Before any pasteurized milk was dispensed, bacteriological testing was done to ensure the absence of detectable bacterial growth. All contaminated milk was discarded or used for other research purposes.
In the hospital microbiology lab, milk samples were inoculated onto blood and MacConkey's agar and incubated at 37°C for 48 hours. Colony counts were calculated for each subculture. Specific bacterial-inhibitory media, which would select for growth of yeast or mold, were not used. Bacteria were identified with standard biochemical tests, morphologic structure, and microscopic characteristics found on Gram stain. Specific identification of Staphylococcus aureus, coagulase-negative Staphylococcus, group B Streptococcus (GBS), α-Streptococcus, Enterococcus, and Bacillus sp. was provided. Gram-negative rods (GNRs) were subtyped but not specifically identified. Positive cultures were expressed in quantitative colony counts from 100 to >20,000 colony-forming units (CFU)/mL. Using these routine culture techniques, we could reliably detect growth down to 100 CFU/mL. We did not perform a specific assay for Bacillus sp. and instead relied on the total aerobic counts. Examining milk cultures throughout the whole year was planned to allow for detection of any seasonal variation in bacterial contamination.
Results
Throughout the calendar year of 2003 we cultured all individual milk samples before and all pooled donor human milk samples after Holder pasteurization. Overall, 810 individual mothers' milk samples from 219 donor mothers were cultured. Ninety-three of these samples (11%) were from 41 mothers who delivered prematurely. Milk from all 219 donor mothers was used to create 303 pools of pasteurized donor milk. Forty-four pools of “preterm donor milk” (15%) originated from the 93 milk samples from mothers who delivered prematurely. Fifty-one (17%) of the pools tested consisted of milk from only one mother.
Bacteriologic screening of donor human milk before pasteurization revealed that 22% of individual donor milk samples had no detectable growth of bacteria on routine cultures. The majority of milk pools (87%) were colonized with Staphylococcus. Sixty-one percent (185) of milk pools were positive for at least one GNR, and 19% (58 samples) were positive for a second GNR. Other Gram-positive organisms identified included enterococci (16%), Streptococcus (8%), and S. aureus (4%). Only one milk sample was positive for methicillin-resistant S. aureus. None was positive for GBS (Table 1). Twenty-five percent of pooled milk samples grew two or more organisms before pasteurization. Bacteriologic profiles of milk expressed from preterm mothers in the first month postpartum did not differ from that expressed by mothers delivering at full term (Fig. 1).
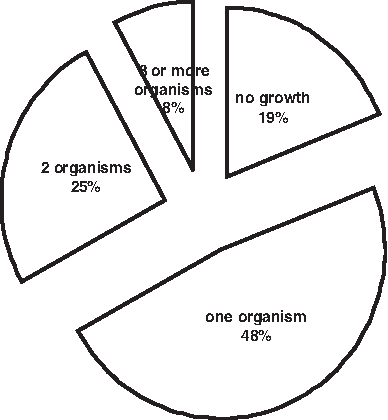
Prevalence of bacteria contaminating unpasteurized milk from mothers delivering prematurely <36 weeks of gestation. Note that the prevalence of any S. aureus was 5%, there was no detectable methicillin-resistant S. aureus, the prevalence of any GNR was 20%, there were no detectable Bacillus sp., and quantitative colony counts were not different from term mothers' milk samples.
After Holder pasteurization, 93% of pooled milk samples showed no growth on routine cultures. In those that were positive after pasteurization, Bacillus sp. was the predominant contaminant. Ten of 17 samples were positive for Bacillus both before and after pasteurization; seven of 17 were found to be positive only after pasteurization. Postpasteurization contamination with coagulase-negative Staphylococcus was noted rarely, in only three of 303 samples (1%). All donor human milk with any detectable bacterial growth after pasteurization was discarded or used for other research purposes.
Discussion and Conclusions
We expected to find that most samples of donor human milk, prior to pasteurization, would be colonized with normal skin flora, including coagulase-negative Staphylococcus, α-Streptococcus, and diphtheroids. Gram-negative bacilli were also found commonly in our donor milk. Our routine surveillance culture results are similar to older reports of bacteriological screening of human milk. Most of these documented growth of predominately coagulase-negative Staphylococcus and GNRs.26–28 A more recent study found similar rates of growth of coagulase-negative Staphylococcus (85%), slightly more S. aureus (13%), and fewer samples of fresh frozen donor milk colonized with GNRs (12%) than we did. 29
Given the expected prevalence of colonization with GBS among pregnant women, we were surprised that GBS was absent from our donor human milk samples. There are reports of breastmilk providing a potential source of neonatal GBS infection.30,31 In addition to GBS, other neonatal pathogens, such as S. aureus, have been found to contaminate donor human milk.32–34 One report from five Brazilian milk banks reported methicillin-resistant S. aureus contamination in 11% of fresh-frozen samples, most with counts <104 CFU/mL. 28 Another study examining quantitative bacterial contamination of raw donor human milk found bacterial growth in the range of 106–7 CFU/mL. 27 Fortunately, this report of raw donor milk use among preterm infants documented few adverse clinical effects, and, in addition, preterm mother's own milk was found to be similar to donor human milk in that both had bacterial colonization in the range of <105 CFU/mL. 27 This is consistent with our findings.
The prevalence of bacterial colonization among our samples of fresh-frozen donor human milk is similar to prior reports.26,35 As in previous reports, we found the pattern of bacterial contamination of human milk expressed by mothers delivering prematurely to be similar to that from term mothers before pasteurization. We had expected to culture more pathogenic or hospital-acquired bacteria, such as methicillin-resistant S. aureus, from “preterm donor milk” because preterm mothers by visiting in the NICU may be exposed to hospital-acquired bacterial flora. The evidence that samples of preterm donor milk are not colonized differently, qualitatively or quantitatively, from the milk of term donor mothers is somewhat reassuring.
Even though we did not specifically assay for Bacillus, we were not surprised to find Bacillus sp. on routine cultures of milk samples before and after pasteurization. A recent Norwegian study also noted a low level of contamination with Bacillus sp. of 1.5%, not unlike our rate of 5%. 29 However, any potential clinical implications of this are unclear from our data. Other member milk banks of HMBANA have corroborated this problem with occasional contamination of pasteurized donor milk by Bacillus. Bacillus sp. are well known in the food industry as contaminating organisms. Heat treatment during cow's milk pasteurization has been thought to enhance the growth of Bacillus. 36 Bacillus endospores can be resistant to hostile physical and chemical conditions and to extremes of heat and cold. In addition, some Bacillus sp. have a range of physiologic adaptations that enable survival in harsh environments. Because Bacillus spores are characteristically resistant to heat, radiation, and disinfectants, they can difficult to eliminate from human milk banks.
We found a wide variety of bacteria contaminating human milk from healthy, donor mothers. Most milk samples grew coagulase-negative Staphylococcus and Gram-negative organisms. Although normal skin flora was cultured typically from milk samples, there were also many donor human milk samples contaminated with pathogenic organisms before pasteurization. The clinical significance of this pattern of low-level bacterial colonization of human milk with regard to preterm infants who are fed their mother's own milk is unclear. Recently, a Norwegian milk bank reported nearly 90% of donor milk samples with low levels of detectable bacteria (<104 CFU/mL) in fresh frozen unpasteurized samples that were fed to newborn infants. 29 There are instances in which a sick preterm infant was thought to have acquired a particular organism from his own mother's milk.30,33 In most circumstances, however, the benefits of feeding a preterm infant his or her mother's own milk far outweigh the potential risks of his exposure to bacteria in her milk. In addition, the human milk-fed preterm infant would receive other immune factors and antibodies specific to potential pathogenic bacteria made by the mother as a result of exposure to her infant's NICU environment.
We conclude that pasteurization using the Holder method of heat treatment is an effective method to eradicate any detectable bacterial contamination of fresh frozen donor human milk. At the very least, routine bacteriological surveillance of the milk after pasteurization is necessary to screen for treatment failures and/or contamination during the pasteurization process. Enhanced growth of Bacillus sp. is particularly problematic during pasteurization in donor human milk banking and must be examined for and dealt with systematically by milk banks.
Footnotes
Acknowledgments
We wish to thank Frank Cho, M.D., for his role in setting up the microbiological screening procedures at the MMBA and Elise Kibler, M.D., in her role as Chair of the MMBA Board of Directors' Research Committee, for manuscript review and approval.
Disclosure Statement
No competing financial interests exist.
This work was presented at the National Conference and Exhibition of the American Academy of Pediatrics, San Francisco, California, in October 2004.