
Abstract
Abstract
Objectives:
Little is known regarding modifiable factors that may explain sociodemographic disparities in breastfeeding rates among women in the United States. Using a mediation model approach, we examined the relative contributions of breastfeeding and formula feeding psychosocial factors in explaining disparities in breastfeeding intentions.
Methods:
We interviewed 532 expectant first-time mothers regarding exposure to breastfeeding by others (breastfeeding exposure), comfort with ideas of breastfeeding (breastfeeding comfort) and formula feeding (formula feeding comfort), and breastfeeding self-efficacy. We used logistic regression to evaluate the independent and mediating effects of these variables on strength of intention to fully breastfeed for 6 months (breastfeeding intention).
Results:
The ethnic distribution of the sample was 41% white, non-Hispanic; 27% Hispanic; 14% African-American; 12% Asian; and 6% mixed or other ethnicity. In the overall sample, formula feeding comfort, breastfeeding comfort, and breastfeeding self-efficacy all independently predicted breastfeeding intention (p < 0.0001), but formula feeding comfort had the largest effect: adjusted odds of stronger breastfeeding intention increased threefold for each 1-level decrease (among four levels) in formula feeding comfort. The unadjusted odds (95% confidence interval) of stronger breastfeeding intention were 0.37 (0.24–0.58) for African-American versus non–African-American women; African-American women had higher formula feeding comfort (2.08 [1.32–3.29]) but similar breastfeeding comfort, breastfeeding self-efficacy, and breastfeeding exposure. Formula feeding comfort mediated 37% of the disparity in breastfeeding intentions between African-American and non–African-American women.
Conclusions:
Formula feeding comfort strongly predicted and substantially mediated ethnic disparity in breastfeeding intention. These results suggest that research and public health efforts aimed at increasing exclusive breastfeeding rates should include consideration of formula feeding attitudes.
Introduction
While it is important to be aware of the demographic groups most at risk for low breastfeeding rates, it is equally important to identify modifiable factors that influence the infant feeding practices of women in the United States. The few studies that examined modifiable risk factors associated with breastfeeding practices were primarily focused on breastfeeding attitudes, knowledge, and perceived barriers,6–9 with little attention to formula feeding attitudes. Studies of modifiable risk factors that focus on African-American women are particularly sparse. In an analysis of data from the National Survey of Family Growth Cycle V, the most common reason cited by black women for not breastfeeding was that they “preferred to bottle-feed.” 4 Among 441 low-income African-American women interviewed at entry into prenatal care, physician support for breastfeeding and support from the father of the baby were independent predictors of maternal intention to breastfeed. 10 In a study of 150 low-income women in Alabama (93% African-American), breastfeeding for >1 month postpartum was more likely among those who were older or had close relatives who breastfed, 11 arguably relatively non-modifiable factors.
As part of a longitudinal study examining the barriers to early lactation success in a multiethnic cohort, we used data gathered from the initial prenatal interview to examine whether potentially modifiable breastfeeding and formula feeding psychosocial factors explain the observed relationship between demographic variables and breastfeeding intentions. We tested the hypothesis that four psychosocial factors amenable to community or individual level intervention—degree of exposure to others breastfeeding, level of comfort with the idea of breastfeeding, level of comfort with the idea of formula feeding, and level of self-efficacy with breastfeeding—are significantly associated with breastfeeding intentions and at least partially mediate the relationship between non-modifiable demographic variables and breastfeeding intentions (Fig. 1). We further sought to determine the independent effects of these psychosocial variables on breastfeeding intentions when considered simultaneously.
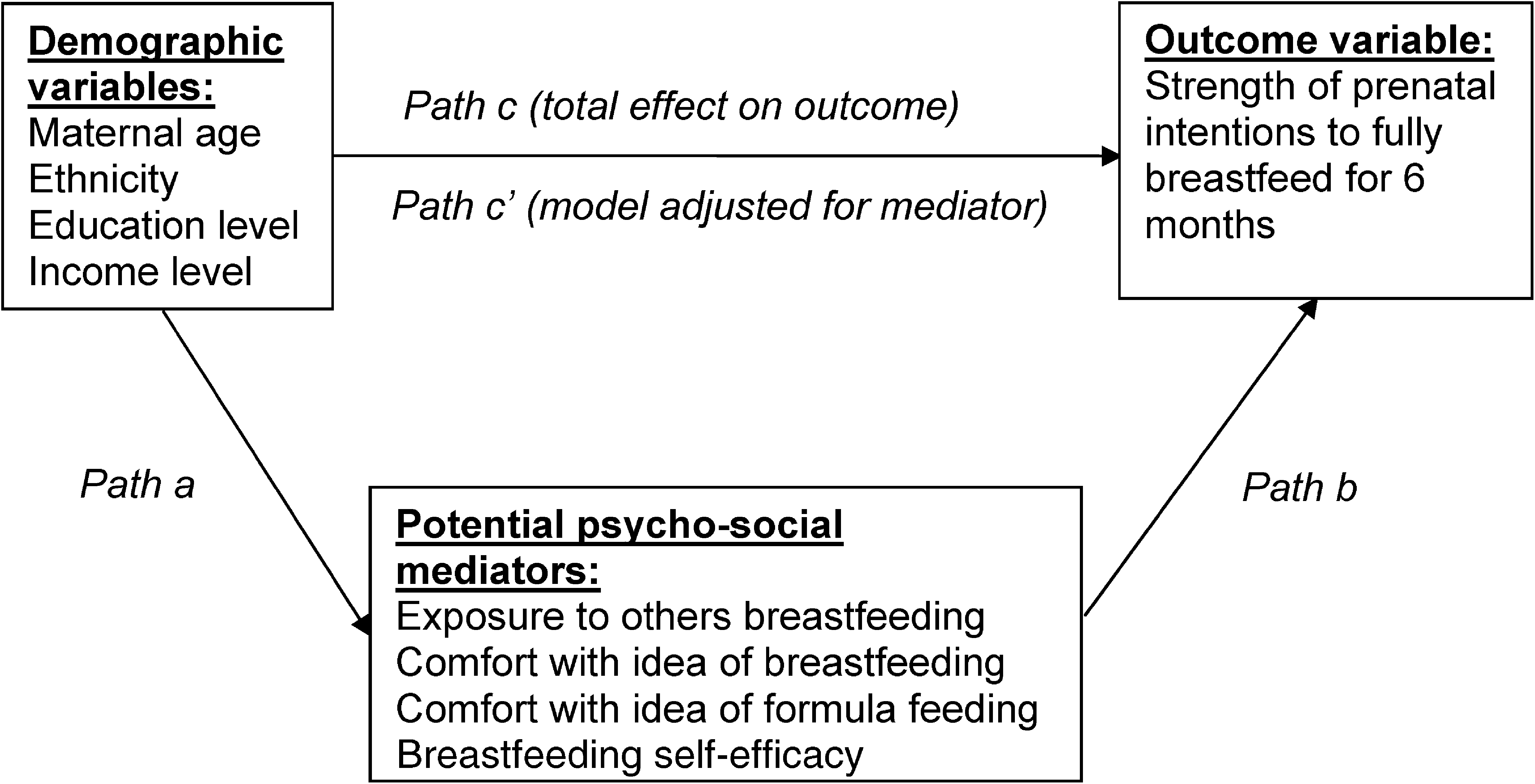
Hypothesized mediation model. For psychosocial variables found to be significant in both path a and path b, the proportion of effect mediated will be estimated from the relative change in the size of the coefficient for path c (relationship between demographic variable and breastfeeding intentions in model without mediator present) compared to path c′ (relationship between demographic variable and breastfeeding intentions in model adjusted for mediator).
Subjects and Methods
Study setting and enrollment
We recruited women receiving prenatal care at a University of California Davis Medical Center (Sacramento, CA) clinic as part of a longitudinal cohort study examining barriers to early lactation success in a multiethnic population of first-time mothers. Because we wanted the prenatal interview to include all eligible women, irrespective of feeding plans, we did not describe the study to potential participants as a breastfeeding study, but rather as an infant feeding study. We explicitly instructed collaborating clinic personnel to inform all potentially eligible women of the study irrespective of feeding plans. We trained study interviewers to present the study and record responses in a non-biased, non-judgmental manner.
We restricted the study to first-time mothers, as they are the most likely to experience difficulties in establishing breastfeeding. 12 We further targeted mothers expecting a term delivery of a healthy infant and living close enough to the University of California Davis Medical Center to make postpartum home visits feasible. Thus inclusion criteria were: expecting first live-born infant, between 32 and 40 weeks of gestation at time of interview, single fetus, speaks either English or Spanish, and ZIP code in the catchment area (8-mile radius of the University of California Davis Medical Center). Exclusion criteria were: referred to the University of California Davis Medical Center because of medical condition, known absolute contraindication to breastfeeding, <16 years old, or <19 years old and not able to obtain parental consent. The University of California Davis Institutional Review Board approved the study protocol and consent form.
Clinic personnel screened all expectant primiparous women receiving prenatal care at a University of California Davis Medical Center clinic between January 2006 and December 2007 for initial eligibility (expectant primiparae, living within the catchment area, at least 16 years old, and without known absolute contraindication to breastfeeding) and asked at a prenatal appointment if they would be willing to learn more about the infant feeding study. A study interviewer approached potential subjects willing to learn more about the infant feeding study at either the same prenatal appointment or a subsequent one. The interviewer described the study, screened for eligibility based on the inclusion and exclusion criteria described in the preceding paragraph, and, if eligible and consenting, conducted the face-to-face prenatal interview in the participant's preferred language (English or Spanish).
Instruments and data collection
Initially we conducted a pilot study with 87 University of California Davis Medical Center prenatal clinic clients in order to develop a prenatal interview instrument with questions that were easily understood, concise, and associated with infant feeding intentions. We conducted a follow-up interview of pilot study participants at 6–10 weeks postpartum in order to collect data on the early infant feeding experience. We generated the initial set of prenatal interview questions from a combination of a thorough review of the literature, consultation with key informants, and previously refined questionnaires.12–14 We translated and back-translated Spanish interview forms until the wording accurately reflected the English version of the forms.
Interview questions relevant to this analysis include demographic information, modifiable psychosocial measures related to infant feeding, and infant feeding intentions. Demographic variables included ethnicity (self-identified), years of education, health insurance status (public versus private), enrollment in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), and age. Psychosocial questions and response options were: (1) How often have you observed another woman breastfeeding (breastfeeding exposure)? (answers: never, a few times, often); (2) How comfortable are you with the idea of breastfeeding your baby (breastfeeding comfort)? (answers: very uncomfortable, somewhat uncomfortable, somewhat comfortable, and very comfortable); and (3) How comfortable are you with the idea of formula feeding your baby (formula feeding comfort)? (answers: very uncomfortable, somewhat uncomfortable, somewhat comfortable, and very comfortable). In addition, we assessed breastfeeding self-efficacy using the validated 14-item Breastfeeding Self-efficacy Questionnaire, Short Form. 15 The latter scale includes statements regarding breastfeeding technique (i.e., “I can always determine that my baby is getting enough milk”) and intrapersonal thoughts (i.e., “I can always successfully cope with breastfeeding like I have with other challenging tasks”). Response choices for each item are: unsure = 1, somewhat unsure = 2, somewhat sure = 3, and sure = 4. We considered low, moderate, and high breastfeeding self-efficacy to be an average score of <3.0, 3.0–3.5, and >3.5, respectively. These cutoffs represent approximate tertiles in the distribution of breastfeeding self-efficacy scores. In pilot testing of the study instruments, we found exposure to formula feeding to be universal, and thus we did not include this question in the final prenatal interview instrument.
We used the Infant Feeding Intentions Scale to assess our outcome of interest, which was strength of intention to fully breastfeed during the first 6 months postpartum (breastfeeding intention). The Infant Feeding Intentions Scale includes two items that probe the strength of intentions to initiate breastfeeding and three items that assess the strength of intentions to be breastfeeding without the use of other milks or infant formula at 1, 3, or 6 months. Total score ranges from 0 (no intention to breastfeed at all) to 16 (very strong intention to fully breastfeed for 6 months). We have recently described the development and validation of the Infant Feeding Intentions, including the observation of a strong, significant relationship between scale score and actual duration of full breastfeeding (Cox proportional hazards χ2 = 92.5, p < 0.0001). 13 We found the relationship between scale score and planned duration of full breastfeeding to be comparable across ethnic groups. 16 As defined previously, breastfeeding intention can be classified as low, moderate, strong, or very strong based on Infant Feeding Intention Scale score values of 0–7.5, 8–11.5, 12–15.5, or 16, respectively). 13
Data analysis
We collapsed the self-identified ethnicities into four broad categories: African-American, Asian, Hispanic, and non-Hispanic white. We categorized study subjects self-identifying with more than one of the above ethnic categories as “mixed ethnicity” and did not include their data in inter-ethnic analyses (but did include their data in overall summary measures). We categorized education level as ≤12 years (high school diploma or less) versus >12 years (some college) and divided maternal age at the median, ≤25 years versus >25 years. We used health insurance status as a proxy for income level, categorized as public versus privately insured. We found WIC status to be 90% concordant with insurance status; thus we did not analyze this variable separately.
Our hypothesized mediation model is shown in Figure 1 (all paths are in reference to Fig. 1). Although the model in Figure 1 hypothesizes a temporal relationship among demographic variables, psychosocial variables, and breastfeeding intentions, we obtained all of the data for this analysis from a single prenatal interview. We constructed a set of contingency tables to examine the distribution of breastfeeding intention category by demographic (path c, Fig. 1) and psychosocial variable strata (path b, Fig. 1). We then constructed a second set of contingency tables to examine the distribution of psychosocial variable responses by demographic variable strata (path a, Fig. 1). We used the Jonckheere-Terpstra trend test, which is a nonparametric test for ordered differences among classes, to test the null hypothesis that the distribution of the response variable (breastfeeding intention category for the first set of tables and psychosocial variable response level for the second set of tables) did not differ among strata of the independent variable.
We used proportional odds logistic regression analysis to examine the independent effects of breastfeeding comfort, formula feeding comfort, and breastfeeding self-efficacy on breastfeeding intention in a multiple variable model. We constructed the model so that the odds ratio for each psychosocial variable response level represents the odds of being in a higher breastfeeding intention category versus lower breastfeeding intention category, compared to the reference response level for that psychosocial variable. We assumed that breastfeeding exposure is an antecedent to the other three psychosocial variables (breastfeeding comfort, formula feeding comfort, and breastfeeding self-efficacy), and thus we did not include it in the multiple variable model.
We identified psychosocial variables significantly associated with both breastfeeding intention and with one or more demographic variables (i.e., both path a and path b in Fig. 1 were significant for a given psychosocial variable) as mediator candidates and included in multilevel analyses to determine how much they attenuated the association between each demographic variable and breastfeeding intention. We used proportional odds logistic regression to examine these models, which we constructed as described in the preceding paragraph. We used the proportion of treatment effect approach to assess mediation, as described by Freedman et al. 17 Therefore, we calculated the proportion of effect mediated as 1 – (βc′/β c ), where β c′ is the maximum likelihood (log odds ratio) estimate of the effect of the demographic variable in a model with the mediator (i.e., adjusted model, path c′ in Fig. 1), and β c is the maximum likelihood (log odds ratio) estimate of the effect of the demographic variable in a model without the mediator (i.e., unadjusted model, path c in Fig. 1). Note that the odds ratio for demographic and psychosocial variables with a positive association with breastfeeding intention will be significantly greater than 1, and the odds ratio for variables with a negative association with breastfeeding intention will be significantly less than 1. Thus, the stronger the mediation effect of a select psychosocial variable, the more the odds ratio estimate for the demographic variable will shift closer to 1, and the log of the odds ratio estimate for the demographic variable will shift closer to zero (recalling the mathematical property, log 1 = 0).
We used SAS version 9.1 (2002–2003, SAS Institute Inc., Cary, NC) for all data analysis.
Results
Sample characteristics
Over the 24 months of study enrollment, 991 women attending a University of California Davis Medical Center prenatal clinic met initial eligibility criteria (expectant primipara, lives within catchment area, >16 years old, and no known absolute contraindication to breastfeeding) and were asked to participate in a screening interview. Of these, three women refused the screening interview, 220 did not meet the screening interview eligibility criteria, 236 met all eligibility criteria but declined to participate, and 532 women met all eligibility criteria and consented to participate in the study (69% of those eligible). Acceptance rates varied significantly by ethnic category (p = 0.0003). Listed from highest to lowest, acceptance rates were as follows: Spanish-speaking Hispanic, 81%; African-American, 73%; white, non-Hispanic, 72%; mixed ethnicity, 70%; English-speaking Hispanic, 70%; and Asian, 52%. Acceptance rates were not significantly different by education level (p = 0.22): less than high school diploma, 77%; high school diploma, 67%; some college, 68%; and college graduate, 70%. Reasons for refusal were: too busy, 51%; not interested, 25%; study too intrusive, 18%; doesn't want to be interviewed about breastfeeding, 3%; and miscellaneous, 2%.
The multiethnic sample was 41% white, non-Hispanic women, 27% Hispanic women, 14% African-American women, 12% Asian women, and 6% women who self-identified from more than one major ethnic group. We conducted 9.6% (n = 62) of interviews in Spanish. Subjects ranged in age from 16 to 41 years. Seventeen percent of subjects did not graduate from high school (12% of subjects 19 years of age or older), 23% were high school graduates, 25% attended at least 1 year of college but were not college graduates, and 35% had at least a 4-year college degree. Overall, 49% of study subjects did not have private health insurance. These data are summarized in the first column of Table 1.
Number (%) of total sample (i.e., down the column).
Number (%) within each breastfeeding intention category for each stratum (i.e., across the row); based on Infant Feeding Intentions Scale score. 13
Z = z-score for the Jonckheere-Terpstra nonparametric trend test, two-tailed.
With African-American and mixed ethnicities excluded, Z = −1.3; p = 0.22.
Infant feeding intentions by demographic and psychosocial variables
Most study subjects intended to at least try breastfeeding. With regard to breastfeeding intention category, 9%, 18%, 32%, and 42% of study subjects were in the low, moderate, strong, and very strong range, respectively. Table 1 presents breastfeeding intention by demographic and psychosocial variables. In unadjusted analyses, all four demographic variables (ethnicity, education level, health insurance status, and age) were strongly associated with breastfeeding intention (value for trend tests, p < 0.0005 for all). Among the four major ethnic groups, there was no longer a significant trend in breastfeeding intention by ethnicity after excluding African-American women from the analysis (value for trend test, p = 0.22). Thus, in further ethnic group analyses we compared African-American women to all other ethnic groups combined. As with the demographic variables, in unadjusted analyses all four psychosocial variables were strongly associated with breastfeeding intention (value for trend tests, p < 0.0005 for all).
As hypothesized, breastfeeding exposure was strongly associated with all of the other three psychosocial variables. Jonckheere-Terpstra trend test two-tailed Z-scores were 4.6, −4.2, and 5.9 for the associations between breastfeeding exposure and breastfeeding comfort, formula feeding comfort, and breastfeeding self-efficacy, respectively (p < 0.0001 for all). For each 1-unit increase in breastfeeding exposure the unadjusted odds (95% confidence interval) of stronger breastfeeding intention were 1.6 (1.2–2.0) times greater, but this relationship was completely attenuated in a model adjusted for the other three psychosocial variables (adjusted proportional odds ratio [95% confidence interval], 0.8 [0.5–1.4]).
Considered simultaneously in a proportional odds logistic regression model, breastfeeding comfort, formula feeding comfort, and breastfeeding self-efficacy were all independently associated with breastfeeding intention (Fig. 2); however, the magnitude of the adjusted odds ratios for formula feeding comfort was by far the largest. The odds of stronger breastfeeding intention increased by approximately 300% with each 1-level decrease in formula feeding comfort (Fig. 2).

Proportional odds regression model estimating the odds of being in a stronger, versus weaker, breastfeeding intentions category compared to the reference group for each of three psychosocial variables. Test of proportional odds assumption, p = 0.96; all odds ratios adjusted for other variables in the model (but no other variables); crude odds ratios averaged 11%, 15%, and 78% higher for breastfeeding comfort, formula feeding comfort, and breastfeeding self-efficacy, respectively.
Psychosocial variable mediation of demographic disparities in infant feeding intentions
Table 2 displays the relationships between demographic and psychosocial variables. There were no significant trends in the relationships between demographic variables and level of breastfeeding exposure or breastfeeding comfort. Breastfeeding self-efficacy was actually stronger among the demographic groups most at risk for weak breastfeeding intentions: women who had public health insurance or were younger or less educated. Thus, breastfeeding self-efficacy, even though associated with both demographic variables and breastfeeding intentions, was not a candidate for mediation analysis.
Values for p were calculated with the Jonckheere-Terpstra nonparametric trend test, two-tailed. NS, not significant.
Formula feeding comfort was the only psychosocial variable that fit the criteria for mediation. In addition to lower formula feeding comfort being significantly associated with stronger breastfeeding intention (path b significant in Fig. 1 [see Table 1]), formula feeding comfort was higher among women who were African-American, less educated, and younger (path a significant in Fig. 1 [see Table 2]). In a proportional odds logistic regression model including all three demographic covariates, African-American ethnicity remained significantly associated with a higher level of formula feeding comfort (adjusted odds ratio [95% confidence interval], 2.1 [1.3–3.4]), whereas education level was marginally associated (1.5 [1.0–2.2]), and maternal age was no longer significant (1.0 [0.7–1.4]). To examine the extent to which formula feeding comfort mediated the relationship between African-American ethnicity and breastfeeding intentions, we constructed a series of models as shown in Table 3. After adjusting for maternal education level, the log odds of stronger breastfeeding intentions for African-American (versus other ethnicity) increased by 22% toward nonsignificance: 1–(−0.333/−0.427) = 0.22. After also adjusting for formula feeding comfort level, the log odds of stronger breastfeeding intentions for African-American (versus other ethnicity) increased an additional 37% toward nonsignificance: 1–(−0.209/−0.333) = 0.37. As summarized in Table 3, the strong relationship between African-American ethnicity and breastfeeding intentions observed in the unadjusted model (adjusted odds ratio [95% confidence interval], 0.37 [0.24–0.58], path c in Fig. 1) was only marginally significant after adjusting for education level and formula feeding comfort (0.62 [0.38–1.00], path c′ in Fig. 1).
Proportional odds logistic regression, modeled to estimate the effect of being in a stronger breastfeeding intention category as assessed by the Infant Feeding Intentions Scale. 13 Test of proportional odds assumption values of p = 0.48, 0.09, and 0.75 for models 1, 2, and 3, respectively.
Percentage change calculated as (1 − [maximum likelihood estimate for adjusted model/maximum likelihood estimate for preceding model]).
Discussion
There are two findings of major importance in this study. First, comfort with the idea of formula feeding, as assessed by the formula feeding comfort variable, had a much greater effect than comfort with the idea of breastfeeding (breastfeeding comfort) in predicting strength of breastfeeding intention. Second, formula feeding comfort was the only psychosocial variable that significantly differed between African-Americans and non–African-Americans, and this difference explained a large portion (37%) of the ethnic difference in breastfeeding intention.
Consistent with national surveillance data, 3 non–African-American ethnicity, college education, private health insurance, and older maternal age were all significantly associated with stronger breastfeeding intention in unadjusted analyses. All four psychosocial variables (breastfeeding exposure, breastfeeding self-efficacy, breastfeeding comfort, and formula feeding comfort) were also significantly associated with breastfeeding intention in unadjusted analyses. In a multiple variable model, breastfeeding comfort, breastfeeding self-efficacy, and formula feeding comfort completely mediated the effect of breastfeeding exposure on breastfeeding intention, reflecting the fact that all three of these psychosocial measures were associated with level of exposure to others' breastfeeding. This finding supports the value of promoting breastfeeding as the normal way to feed infants, as recommended in the Department of Health and Human Services “Blueprint for Action on Breastfeeding.” 18
Although others have reported significant associations between breastfeeding psychosocial measures and breastfeeding intention,7,8,11,19–23 we believe this is the first study to examine the relative magnitude of the effects of comfort with the idea of breastfeeding versus comfort with the idea of formula feeding on breastfeeding intention. In a model with both of these covariates, the effect sizes for formula feeding comfort were two- to sixfold greater than for breastfeeding comfort in predicting strength of breastfeeding intentions. Furthermore, of the four psychosocial variables examined, only formula feeding comfort attenuated the disparity in breastfeeding intentions between African-American and non–African-American women. This finding is consistent with the finding by Forste et al., 4 that the primary reason indicated by black women for not breastfeeding was that they “preferred to bottle-feed.” Additional research is needed to improve our understanding of what makes women comfortable with the idea of formula feeding, so that this information may be incorporated into breastfeeding promotion campaigns. It is possible that community and individual-level efforts that mention potential risks of formula feeding may also be an effective strategy in narrowing the disparity in breastfeeding rates between African-American women and other U.S. women. At the same time, it is equally important to address barriers to exclusive breastfeeding that may underlie women's comfort level with the idea of formula feeding.
Other demographic (age, education, income) disparities in breastfeeding intentions were not explained by the four psychosocial variables examined.
Limitations
We used a cross-sectional design, entirely based on the data collected from the prenatal interview, to examine the hypothesis of this article. The associations found with the primary outcome measure, strength of breastfeeding intentions, do not necessarily guarantee that there are similar associations with actual breastfeeding behavior. It is also possible that “social desirability” led some participants to inflate their breastfeeding intentions. In previous validation research, however, we demonstrated that the Infant Feeding Intentions Scale was highly predictive of actual behavior during the first 6 months postpartum among a multiethnic sample of low-income, first-time mothers. 13
These results are also limited in their generalizability. The quantitative nature of the study design provides insights into the relative importance of comfort with the idea of breastfeeding versus formula feeding, but more in-depth qualitative research is needed in order to understand what these terms mean to women and what factors contribute to their comfort with both of these feeding choices. In addition, the women who participated in the study resided in northern California, a region with high breastfeeding rates. 24 The small numbers of women “very comfortable” with the idea of formula feeding and “very uncomfortable” with the idea of “breastfeeding” in this sample resulted in large confidence intervals around the odds ratios for these responses and thus must be interpreted with caution. The relationships observed among demographic, psychosocial, and infant feeding intention measures may not be the same in other regions of the United States. For example, we did not find an association between maternal education level and either breastfeeding exposure or breastfeeding comfort, but this may not be the case in areas of the United States with lower breastfeeding rates, such as the South. 24 Further study of these relationships in other areas of the United States is warranted.
Conclusions
Maternal infant feeding decisions are likely the result of a complex interplay of variables and are thought to be strongly influenced by cultural norms and experiences prior to pregnancy. 10 Identifying modifiable factors that may influence infant feeding intentions is an important step in the development of effective breastfeeding promotion efforts, whether community-wide or targeted to the individual woman before or during pregnancy. Level of comfort with the idea of formula feeding may be one of these factors. Breastfeeding exposure, breastfeeding self-efficacy, breastfeeding comfort, and formula feeding comfort were all significantly associated with breastfeeding intentions and therefore may be important to consider in breastfeeding promotion efforts; however, formula feeding comfort was both the strongest predictor of feeding intentions and the only measure found to mediate the disparity in breastfeeding intentions between African-American and non–African-American women. These results suggest that it is at least as important to consider attitudes towards formula feeding as it is to consider attitudes towards breastfeeding, when seeking to understand maternal breastfeeding intentions.
Footnotes
Acknowledgments
We thank all of the study participants and thank the University of California at Davis Medical Center prenatal clinic staff for their cooperation. We also acknowledge the skillful, dedicated assistance of the Prenatal Team leaders (Leslie Lane, Zeina Maalouf, Barbora Rejmanek, and Bineti Vitta) and 22 undergraduate student interviewers comprising the Prenatal Interview Team. This research was supported by grant R40 MC 04294 from the Maternal and Child Health Bureau (Title V, Social Security Act), Health Resources and Services Administration, U.S. Department of Health and Human Services.
Disclosure Statement
No competing financial interests exist.