
Abstract
Abstract
Despite the fact that exclusive breastfeeding is the gold standard for feeding babies through 6 months of age, there is a notable paucity of information regarding the effect of various chronic maternal illnesses on lactation. With increasingly effective obstetrical and subspecialty management of pregnancy in these women, a growing number of questions about breastfeeding in the context of chronic maternal illnesses will be asked. Here we describe a case of successful exclusive breastfeeding by a woman with long-standing membranous glomerulonephritis.
Introduction
Less is known about maternal-fetal implications of idiopathic MGN. Sebestyen et al. 3 documented the management of a pregnancy complicated by severe nephrotic syndrome in MGN. Katzir et al. 4 reported a case in which a pregnant woman whose MGN had been in remission for 12 months prior to conception developed nephrotic syndrome and uncontrolled hypertension early in the second trimester. Healthy infants were born in each of the above cases. In a retrospective study of nine women who had more than one pregnancy after the diagnosis of MGN, a live infant was born in 27 of 30 pregnancies. 5
With increasingly effective management by obstetricians and nephrologists of renal disease during pregnancy, a growing number of questions about breastfeeding in the context of renal disease will be asked.
There is little published information about the effect of various chronic maternal illnesses on lactation. Here we describe a case of successful exclusive breastfeeding by a woman with MGN.
The policy of Indiana University-Purdue University, Indianapolis, IN, is that case reports are not reviewed by its Institutional Review Board.
Case Report
A 27-year-old primigravida woman with a longstanding history of antinuclear antibody-positive MGN and hypertension visited her nephrologist early in the first trimester of pregnancy. Her medical history included renal biopsies at 17 and 26 years of age. The most recent revealed stable stage II–III membranous glomerulonephritis with some mesangial proliferative features but no evidence of scarring. For the past decade she has had proteinuria between 1 and 2.5 g/24 hours (normal, 0.04–0.23 g/24 hours), but proteinuria increased in the year prior to conception to 4.9 g/24 hours. Four months before conception the woman's serum albumin level was 2.6 g/dL (normal, 3.4–5.0 g/dL). She had a history of well-controlled hypertension for at least 5 years and of hyperlipidemia for 10 years. Medications included losartan (100 mg/day) (for the past 5 years), atorvastatin (10 mg/day) (for the past 10 years), furosemide (20 mg as needed) (infrequently), vitamin C (2–4 g/day), and fish oil (2 g twice a day).
Because of the increase in proteinuria, she consulted a leading national expert in glomerular disease and was considering initiating immunosuppressive therapy. However, once she was aware of her pregnancy, given the risk/benefit profile, immunosuppressive therapy was considered unwarranted at that time. She also discontinued losartan and atorvastatin when she learned she was pregnant.
Her significant family history included coronary artery disease, hypertension, and hyperlipidemia on the maternal side. Her mother died at age 45 years from a myocardial infarction.
Calculated creatinine clearance at the first trimester visit was normal. The most recent serum creatinine levels were 0.5–0.6 mg/dL (normal, 0.6–1.2 mg/dL), and urinalysis showed five to 10 red blood cells/high-powered field (normal, none to two red blood cells/high-powered field).
This woman planned to breastfeed her child. The nephrologist was concerned that the breastmilk would be low in protein because of her chronic low albumin level. It was suggested that her milk might not provide adequate nourishment for her newborn and that supplements might be required. It was also suggested that her milk be tested for protein content.
Shortly after this visit with her nephrologist, she attended a breastfeeding class during which she discussed her concerns for her milk. The lactation consultant teaching the class had not encountered a situation like hers before and puzzled over what would be a good supplement if needed. The pregnant woman recalled: “My plan at that point was to breastfeed, and to cross the bridges of protein content and supplementing if/when we came to them, but I was still very confused as to what might constitute a reason to supplement.”
At the first trimester visit the woman's weight was 62.9 kg, and systolic/diastolic blood pressure was 120/82 mm Hg. She maintained a low-sodium diet; the increased risk for preeclampsia was discussed. She also consulted a specialist in high-risk obstetrics, beginning in the first trimester.
Despite her own extensive internet (and other) research, the pregnant woman remained frustrated with her inability to find good information about her future of breastfeeding. She talked with one of the co-authors (S.E.A.), an International Board Certified Lactation Consultant, who counseled that it was not at all certain that her renal disease would adversely affect her ability to breastfeed. She also attended additional prenatal education classes, including a breastfeeding class taught by a lactation consultant who encouraged her.
At approximately 30 weeks of gestation she developed elevated blood pressure. It was controlled by strict bedrest (rising to 130/90 mm Hg when sitting) over the next 4 weeks. Urine dipstick protein showed 2+ to 3+.
At 34 weeks she was admitted to the hospital for overnight observation because of preterm contractions on a nonstress test during a scheduled clinic visit. Blood pressure was 147/98 mm Hg. Her nephrologist recommended amlodipine (2.5 mg twice a day) with an increase to 5 mg twice a day if necessary for blood pressure greater than 140/90 mm Hg. She went home on this regimen the next day. At 37 weeks a blood pressure reading was 140/90 mm Hg.
Because blood pressure was mildly elevated, an induced vaginal delivery was scheduled for 37½ weeks. However, by that time, the woman was, by self-report, “much calmer,” with normal blood pressure and a normal, healthy baby, placenta, and umbilical cord on ultrasound. After talking with the obstetrician, she (and her partner) decided to forego the induction.
The woman went into labor spontaneously and was admitted to the hospital at 39 weeks. Weight was 80.9 kg, blood pressure was 120/82 mm Hg, and urine dipstick protein was 3+. Preeclampsia was diagnosed, with blood pressure of 187/119 mm Hg and 2+ pitting edema of her right leg. She was treated with labetalol intravenously, as well as magnesium for 24 hours for seizure prophylaxis.
The baby was born by spontaneous vaginal delivery at 39 weeks of gestation. In consultation with the nephrologist, amlodipine was increased to 5 mg twice a day on the second postpartum day. She was discharged to home on the third postpartum day. Blood pressure was 140/70 mm Hg.
Her infant son's birthweight was 3,800 g (75th–90th percentile). Apgar scores at 1 and 5 minutes were 7 and 9, respectively, and physical examination was normal. He was breastfed exclusively (no other liquids or solids were given). 6
At her 6-week postpartum visit to the obstetrician, her weight was 64.5 kg, and blood pressure was 112/70 mm Hg. Serum albumin was 1.6 g/dL 2 months before delivery and 1.5 g/dL 1 month before delivery. By 3 months after delivery, it was back up to 2.9 g/dL.
The mother described the infant's visits to the pediatrician as “uneventful, with normal growth and development observed at each visit.” The infant's growth chart is shown in Figure 1. She returned to the nephrologist at 3 months postpartum, and when he observed the child, he chuckled and said that clearly the mother's milk “was just fine.” Milk testing was never ordered. (The nephrologist mentioned having tested other mothers' milk for protein content in the past.) The child continued to grow and develop normally.
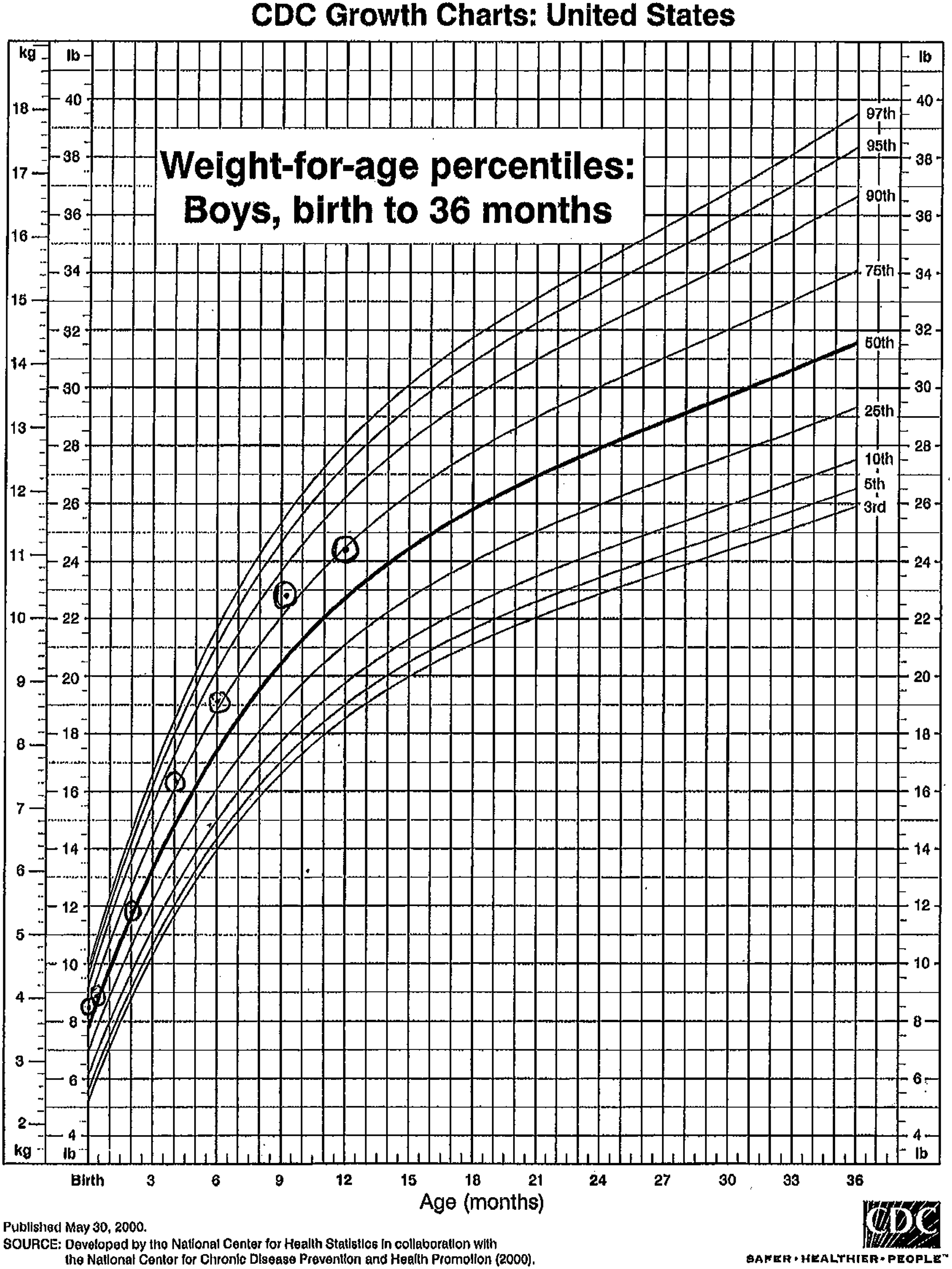
The infant's growth chart.
When the mother thought she might need antihypertensive medications, she brought the book Medication and Mother's Milk 7 to her appointment with the nephrologist. The nephrologist has been using the categories and recommendations in that book in his decision-making.
The woman's health was stable; at 3 months postpartum her renal studies were somewhat improved compared to before pregnancy: “Breastfeeding seems to agree with me.” She continued to eat a low-sodium diet; her medications now included vitamin C, a prenatal vitamin, fish oil, supplemental lecithin, and oral contraceptive pills. After the difficulties of her pregnancy, the woman and her partner wanted the added protection of oral contraceptive pills, in addition to the protection afforded by lactational amenorrhea. Her nephrologist said that she could remain off renal medications for at least the infant's first year, and possibly long beyond that. Her weight was 62.9 kg, and her blood pressure had normalized at 117/70 mm Hg. Serum creatinine was 0.8 mg/dL (normal, 0.6–1.2 mg/dL). Serum albumin remained low (she had been nephrotic at delivery).
The mother was pleased to report that she had achieved her exclusive breastmilk feeding and breastfeeding duration goals despite the uncertainties of her medical condition. At 1 year of age, the infant's weight was 11.1 kg (75th percentile), and length was 78.2 cm (75th–90th percentile). He is now more than 15 months old and still breastfeeding.
Discussion
Glomerulonephritis and other renal diseases are associated with increased risk to a pregnant woman and fetus1–4,8; however, with nephrologists' and obstetricians' increasingly effective management of renal disease during pregnancy, 9 these clinicians and pediatricians and others will likely be asked a growing number of questions about breastfeeding in the context of chronic maternal renal conditions. An epidemiologic study of pregnant women in the State of Washington estimated that 0.03% had underlying renal disease.9,10 This rate means that, on average, if there are 4,265,000 deliveries per year in the United States (for the year 2006, according to the Centers for Disease Control and Prevention), 11 more than 1,200 such pregnant women will deliver each year.
Beyond the textbooks and related literature for lactation specialists and perinatologists,12–14 little has been published for other healthcare professionals and the lay public about breastfeeding in the context of chronic, noninfectious maternal illness. A recent article about lactation in Crohn's disease is an exception. 15 For women with glomerular disease, the breastfeeding textbook recommends as follows:
The option to breastfeed is a matter of the risk/benefit ratio. It involves not only the medical status of the mother but also that of the infant and the drugs that must be used to keep the mother stable. The obstetrician, nephrologist, and neonatologist must determine the appropriateness of breastfeeding on a case-by-case basis. 12
This mother's illness did not adversely affect her ability to breastfeed successfully. As she and her partner now contemplate the possibility of having a second baby, she expressed dissatisfaction with the degree of uncertainty associated with her medical condition: “The lack of information/understanding about how my disease plays a role from conception to birth to breastfeeding (and, of course, in my own quality of life in the coming decades) is so very frustrating and, I think, at times alarming to medical professionals.” She recalls that the nephrologists who visited her on the postpartum ward told her that they “usually recommend against pregnancy in kidney patients,” but that in her case everything had turned out all right; her blood pressure was stabilizing, and she could go home. On the question of breastfeeding they referred her to her private nephrologist for follow-up.
Just as teamwork between nephrologists and obstetricians is needed for best management of chronic renal disease in pregnancy, collaboration and communication between healthcare providers (for women and children, and across the prenatal and postpartum periods) are required to best promote, protect, and support breastfeeding. 16 In this case, teamwork was especially important given the involvement of many different providers with different specialties, the multiple medications and the need to assess their compatibility with breastfeeding, and the patient's self-advocacy. To this end, we report this case of successful breastfeeding with a history of MGN, hypertension, and hypoalbuminemia.
Footnotes
Disclosure Statement
No competing financial interests exist.