
Abstract
Abstract
Background:
Woman who struggle with drug addiction during pregnancy are perhaps the most vulnerable of new mothers. The opioid substitution medications methadone and buprenorphine are both compatible with breastfeeding. The objective of this study is to determine breastfeeding rates among opioid-dependent women giving birth in a Baby-Friendly Hospital.
Methods:
We performed a retrospective chart review of all infants born at Boston Medical Center (Boston, MA) between July 2003 and January 2009 with a diagnosis of neonatal abstinence syndrome. Feeding information was obtained, as well as baseline medical information about the mother–infant pairs. Breastfeeding eligibility was determined by a negative urine toxicology screen on admission, no illicit drug use in the third trimester, and a negative human immunodeficiency virus status.
Results:
Two hundred seventy-six mother–infant pairs were identified. Forty percent of the mothers carried one or more psychiatric diagnoses; 24% were taking two or more psychiatric medications. Sixty-eight percent of the mothers were eligible to breastfeed; of those, 24% breastfed to some extent during their infant's hospitalization. Sixty-percent of those who initiated stopped breastfeeding after an average of 5.88 days (SD 6.51).
Conclusions:
Breastfeeding rates among opioid-dependent women were low, with three-quarters of those eligible electing not to breastfeed. Of the minority of women who did choose to breastfeed, more than half stopped within 1 week.
Introduction
Breastfeeding offers optimal health outcomes for the mother–infant dyad. 6 In 2007, the Agency for Healthcare Research and Quality published a summary reporting that a history of breastfeeding was associated with a reduction in the infants' risk of otitis media, serious lower respiratory tract infections, gastroenteritis, asthma, leukemia, childhood obesity, types 1 and 2 diabetes, and sudden infant death syndrome. 7 For mothers, a lack of breastfeeding was associated with higher rates of breast cancer, ovarian cancer, and type 2 diabetes. 7 This population of mothers on methadone and their infants has unique benefits to gain from breastfeeding due to the emotional, behavioral, and medical complications that often affect them. Breastfeeding has been shown to act as an analgesic for infants and is established to be beneficial for soothing agitated infants, thus potentially improving withdrawal symptoms in infants with NAS. 8 This vulnerable group of women would also seem to benefit from improved attachment to their infants. 9 However, despite current recommendations regarding breastfeeding in this population, some clinicians remain cautious when encouraging breastfeeding in those with a history of methadone use.10,11
In 2001, methadone was added to the table of “usually compatible with breastfeeding” in the American Academy of Pediatrics's statement “Transfer of drugs and other chemicals into human milk.” 12 Recent studies have shown that the transfer of methadone into human milk is minimal.13–17 Concentrations of methadone in breastmilk are unrelated to maternal doses and are particularly low in infant plasma and therefore unlikely to cause any adverse pharmacological effects in the infant.13–16,18,19 In recent years, buprenorphine has been used as an alternative agent to treat opioid-addicted mothers during pregnancy. Preliminary data show that these infants have a less severe form of NAS with similar perinatal outcomes.20–26 Buprenorphine is considered to be compatible with breastfeeding due to its poor oral bioavailability. 27
Some studies suggest that the small amount of methadone in the breastmilk may help minimize withdrawal symptoms and shorten medical treatment and length of hospitalizations in infants with NAS; however, the mechanism is unknown.28–30 There are reports of withdrawal among infants whose mothers were taking methadone and stopped breastfeeding suddenly. 31 Thus there is a conflict between the low levels of methadone found in breastmilk and the reported mitigating effect of breastfeeding on the severity of NAS, leading one to think that other factors related to the breastfeeding itself may be responsible. 17
Despite recent recommendations and research, many questions remain regarding breastfeeding in this population. The objective of this study was to determine rates of breastfeeding eligibility, initiation, and continuation among opioid-dependent women giving birth in a Baby-Friendly Hospital.
Subjects and Methods
We reviewed the charts of all infants born at Boston Medical Center (BMC) (Boston, MA) between July 2003 and January 2009 with a diagnosis of NAS. Additional eligibility criteria included: gestational age ≥35 weeks; infant transferred from the well baby unit or neonatal intensive care unit (NICU) to the pediatric inpatient unit when the mother was discharged from the maternity service; and mother taking either methadone or buprenorphine during her pregnancy as an opioid-substitution medication. Infants with NAS were excluded from the study if they were transferred from BMC to another hospital prior to being medically ready for discharge, or if they required a NICU admission for more than 48 hours or a prolonged hospital stay for reasons other than NAS.
Subjects were identified with the assistance of the BMC Data Warehouse, which has access to all clinical, laboratory, and administrative data on all admissions at BMC. Initial search criteria included: a discharge diagnosis of NAS; an infant urine toxicology screen in the first 24 hours of life; or a medication order for diluted tincture of opium or phenobarbital during the infant's hospitalization. We then reviewed the medical records of all infants identified by the Data Warehouse to see if they met our inclusion criteria. In addition, we cross-checked the Data Warehouse list with our well baby unit log, which documents infant transfers to the inpatient service for further management of NAS.
Using the electronic medical record, data extraction was conducted by two of the authors (EW, JB). Baseline characteristics were collected on the infants, including birth demographics, medications and medical diagnoses, and length of hospitalization. Maternal records were reviewed in conjunction to obtain baseline information including obstetrical complications, medical diagnoses, and substance abuse treatment during the pregnancy.
A mother was determined to be eligible to breastfeed if she met three criteria: (1) negative urine toxicology screen while on the labor and delivery unit; (2) no evidence of illicit drug use in the third trimester of pregnancy; and (3) negative human immunodeficiency virus status. Infant feeding information was obtained from the 24-hour flow sheet completed for every infant by the nursing staff. Information on the flow sheet included documentation of each infant feeding and the type of feeding given. Breastfeeding for this study was defined as the consumption of any amount of breastmilk within a 24-hour period.
For the 6 years investigated during this study, birth rates at BMC fluctuated between approximately 2,100 and 2,600 per year. This study received Boston University Medical Center Institutional Review Board approval. Counts of observed frequencies were determined for baseline characteristics and breastfeeding rates in our study population. The mean and SD, as well as the median and range, were determined for duration of breastfeeding. Means and SD were also calculated for the infant's length of hospitalization, as well as the methadone and buprenophrine doses the mothers were taking at the time of delivery. The χ2 test was used to evaluate potential differences between the mothers who breastfed and those who were eligible but did not breastfeed.
Results
Two hundred seventy-six mother–infant pairs were identified. The majority, 81% (223 of 276) of the infants, were ≥37 weeks' gestational age, and 78% (215 of 276) had a birth weight ≥2,500 g. Forty-five percent of the mothers gave birth via cesarean section and 65% were positive for the Hepatitis C virus (Table 1). A majority of the mothers carried one or more psychiatric diagnoses, including 42% with depression, 17% with bipolar disorder, and 42% with an anxiety disorder. One-fifth of the mothers were taking a selective serotonin reuptake inhibitor, 23% were taking benzodiazepines, and 28% were taking other psychiatric medications. A breakdown of these medications is provided in Table 2. The majority of these medications are lactation risk category L2 or L3. 27 In no instance was a mother deemed ineligible to breastfeed because of her prescribed psychiatric medications.
SSRI, selective serotonin reuptake inhibitor.
Prozac, Eli Lilly and Co., Indianapolis, IN; Zoloft, Pfizer, New York, NY; Paxil, GlaxoSmithKline, Research Triangle Park, NC; Celexa, Forest Pharmaceuticals, New York; Effexor, Wyeth Pharmaceuticals (now part of Pfizer); Ativan, Wyeth Pharmaceuticals; Klonopin, Roche, Indianapolis; Valium, Roche; Xanax, Pfizer; Welbutrin, GlaxoSmithKline; Risperdal, Janssen Pharmaceutica, Titusville, NJ; Seroquel, AstraZeneca, Wilmington, DE.
By the classification system of Hale 27 : L1, safest (drug has been taken by a large number of breastfeeding mothers without any observed adverse effects in infants; controlled studies in breastfeeding women fail to demonstrate a risk to the infant and the possibility of harm to the breastfeeding infant is remote; or the product is not orally bioavailable in the infant); L2, safer (studies in limited number of breastfeeding women without an increased in adverse effects in the infant and/or the evidence of a demonstrated risk that is likely to follow use of this medication in a breastfeeding woman is remote); L3, moderately safe (there are no controlled studies in breastfeeding women; however, the risk of untoward effects to a breastfed infant is possible; or controlled studies show only minimal non-threatening adverse effects; drugs should be given only if the potential benefit justifies the potential risk to the infant); L4, possibly hazardous (there is positive evidence of risk to a breastfed infant or to breast milk production, but the benefits from use in breastfeeding mothers may be acceptable despite the risk to the infant); L5, contraindicated (studies in breastfeeding mothers have demonstrated that there is significant and documented risk to the infant based on human experience, or it is a medication that has a high risk of causing significant damage to an infant; the risk of using the drug in breastfeeding women clearly outweighs any possible benefit from breastfeeding; the drug is contraindicated in women who are breastfeeding an infant).
Ninety-two percent (254 of 276) of mothers were taking methadone as an opioid substitute (average daily dose, 84.2 mg); 8% were taking buprenorphine (average daily dose, 12.6 mg) (Table 2). The mean length of hospitalization for the infants was 22.8 days (SD 10.9) with a median of 20 days (range, 4–67 days).
As noted in Figure 1, 32% of the opioid-dependent mothers were ineligible to breastfeed for the following reasons: positive urine toxicology screen on labor and delivery (n = 49); illicit drug use in the third trimester (n = 37); or positive human immunodeficiency virus status (n = 3). Seventy-six percent of the 187 women who were eligible to breastfeed chose not to breastfeed their infants. There were no differences in rates of depression, anxiety, bipolar disorder, hepatitis C, psychiatric medication use, or dose of opioid substitute between the breastfeeders and the non-breastfeeders in our univariate analysis (p > 0.05 for all) (Table 3); thus a multivariate analysis was not performed. Of the 24% of women who did initiate breastfeeding shortly after delivery, 40% were still breastfeeding when their infants were discharged home from the hospital. The remaining 60% of the mothers stopped breastfeeding after an average of 5.9 days (SD 6.51) in the hospital.
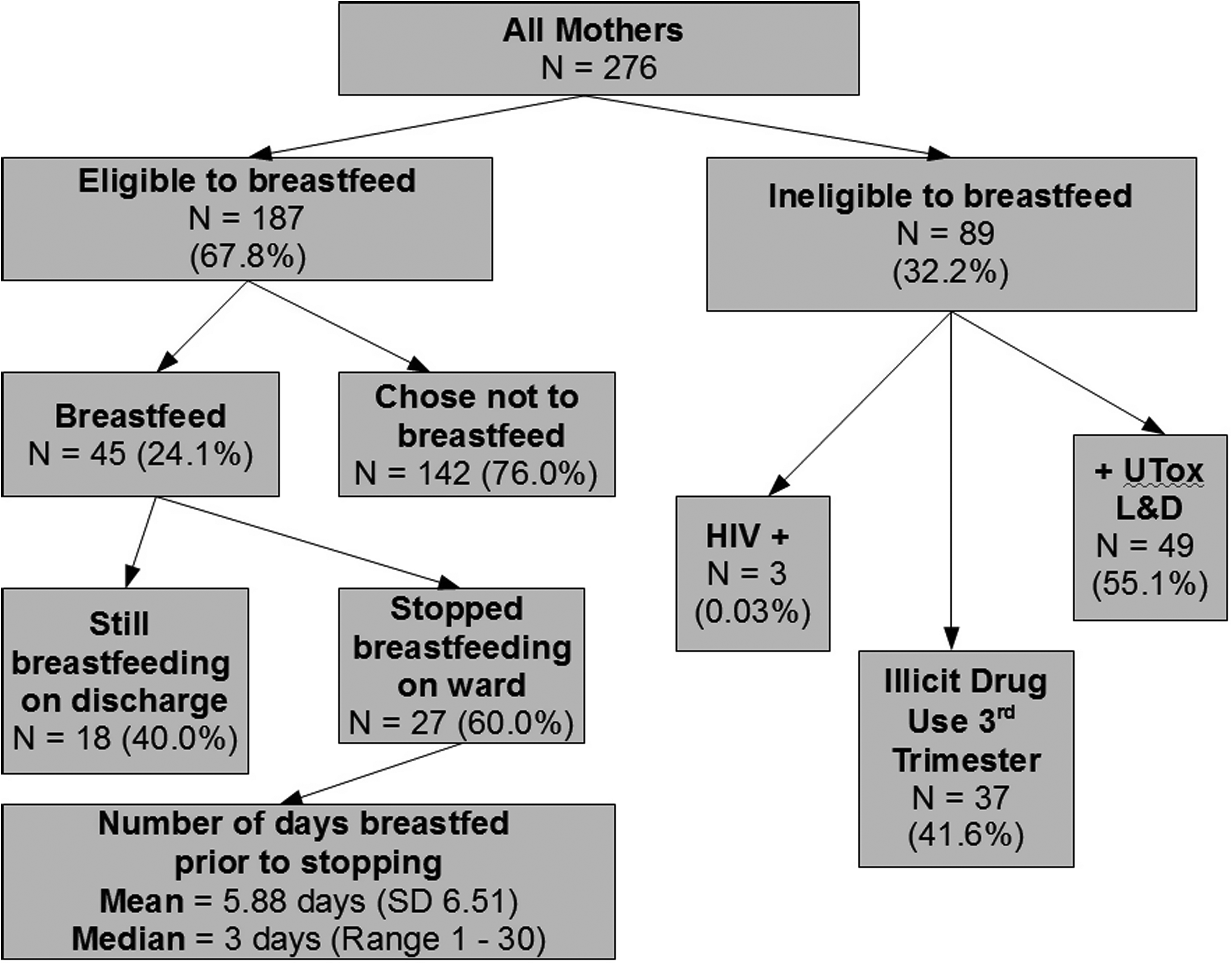
Breastfeeding eligibility, initiation, and continuation rates. HIV, human immunodeficiency virus; UTox L&D, urine toxicology screen in Labor and Delivery unit.
Of the group of 45 women who breastfed, 20% were taking buprenorphine, and 80% were taking methadone. Of the 8% (n = 22) women in the study taking buprenorphine, 90% were eligible to breastfeed; 45% of those women chose to breastfeed their infants. Fifty-two percent of the 254 women taking methadone met eligibility criteria to breastfeed; 27% of those women initiated breastfeeding. This observed difference in breastfeeding rates between those taking methadone and buprenorphine was not statistically significant (p = 0.74).
Discussion
We found that although a majority of opioid-dependent mothers met eligibility criteria to breastfeed, breastfeeding initiation and continuation rates were low. Three-quarters of the women eligible to breastfeed chose not to despite giving birth in a Baby-Friendly Hospital environment that was supportive of breastfeeding with knowledgeable clinical staff, availability of one-on-one help from lactation consultants and breastfeeding peer counselors, and readily available breast pumps. We believe that the low breastfeeding rates reflect the significant challenges these women face. The work of recovery requires frequent support group meetings, individual therapy sessions, and daily trips to the addiction program site for medication and required drug testing. In addition to time constraints, many of these mothers have limited financial resources, struggling to cover the costs of travel, parking, and child care needed to allow them to go to the hospital daily to care for their new infant.
The literature offers a variety of other reasons why these women may choose not to breastfeed, including family and social factors, and multiple medical and psychiatric co-morbidities. For instance, a lack of education regarding the established safety of breastfeeding in the presence of hepatitis C infection may discourage them.32,33 However, we do not feel this was an issue at our hospital given our level of staff experience about the disease. The literature also reports issues of low self-esteem, guilt, and low tolerance for discomfort such as sore nipples among these women. 30 Our study did reveal high rates of psychiatric illness, requiring up to 30% of the mothers to be placed on one or more psychiatric medications. The use of psychotropic medications in lactating women must balance the risk of possible harmful effects on the infant with the woman's severity of mental illness and the established benefits of breastfeeding.34,35 In general, the benefits of breastfeeding outweigh the relatively small risk of the psychotropic medications. 36 In addition to maternal psychiatric issues, there are medical difficulties with the infant as well. Drug-exposed infants often have irritability, hypertonicity, nasal stuffiness, feeding problems, and failure to thrive, which makes breastfeeding significantly more difficult without intensive support. The majority of these infants need supplemental calories for adequate growth, and some require nasal-gastric tube feedings for some period of time due to poor oral feeding.
As a regional safety net hospital, BMC is in a unique position. BMC provides care for a large number of mothers with drug addiction problems and infants with NAS and has a high breastfeeding initiation rate. Because of the difficulties and provider confusion surrounding breastfeeding in this population, a multidisciplinary task force was created that resulted in the Breastfeeding and Illicit Drug Use Guidelines in July 2008 (see Appendix). These new guidelines provide consistency and emphasize the importance of putting the mother's drug recovery first and foremost. In addition, those mothers who are eligible and willing to breastfeed receive all possible supports.
One of the limitations of this study is that it is a retrospective chart review; definite reasons as to why these women chose not to breastfeed and why they stopped breastfeeding were unable to be fully explored. The smoking status of the mothers was not obtained, which may have been a contributing factor in their decision. In addition, over the 6-year study period, there were slight variations in hospital guidelines concerning NAS and breastfeeding and changes in the NAS treatment protocol. Also, given that the BMC buprenorphine program only started in 2006, the number of women taking buprenorphine included in this study was small.
Conclusions
The hospital staff of a Baby-Friendly Hospital spend a significant amount of time and energy assisting mothers of infants with NAS to breastfeed; despite these efforts, breastfeeding initiation and continuation rates among opioid dependent women are low. The reasons for these low rates are unknown. Psychiatric illness and psychotropic medication use are high, but neither was associated with breastfeeding status in our patient population.
Footnotes
Acknowledgments
The authors would like to thank the medical, nursing, and lactation staff in the Boston Medical Center Birth Place and pediatrics ward.
Disclosure Statement
No competing financial interests exist.