
Abstract
Abstract
In the 1990s a rising tide of medical, surgical, and instrumental interventions served to make childbirth almost treated like a disease. This report supports a different approach to childbirth. A case and discussions of induction are presented. A national survey of 1,573 pregnant women throughout the United States was collected. Although most U.S. childbearing women are low risk, childbirth is “procedure intensive.” Women reported significant interventions such as regional analgesia (76%), ruptured membranes (65%), forceful pushing (75%), and cesarean sections (32%). The U.S. rate of cesarean sections in 2005 was the fourth highest among 25 countries. The epidural has many negative features. When used in labor it extends the length of time from 5 to 7 h, causes a raised temperature greater than 100.4°C in 15–30% of infants and mothers, and produces a very sleepy baby at birth, irritable and with increased crying for 3 weeks. The three hormones that relieve pain are turned off by the epidural or a cesarean section. Maternal and infant mortality was doubled as a result of cesarean section. After cesarean sections, subsequent pregnancies have types of abnormal attachments of the placenta to the uterus. British physicians recommend normal birth, defined as labor that starts on its own and uses no analgesia, no inductions, no interventions, no epidurals, and no cesarean sections. The doula's presence decreases labor length, significantly decreases cesarean sections, means less use of pain medicine, and gives greater breastfeeding rates.
Changing Women's Status
The human female body was designed to produce an offspring in an uncomplicated and straightforward manner when a woman is healthy and properly supported. In reality, most women in our society are healthy with normal fetuses, and with appropriate care their pregnancy can proceed, and the experience can be positive and life-changing.
At some point in the late 1980s and early 1990s, the situation began to change. We watched in dismay as the rising tide of medical, surgical, and instrumental interventions served to make childbirth treated almost as an illness, rather than a normal function of women's bodies. Now childbirth in many American hospitals and medical schools has been “hijacked” away from a mother-centered birth.
We argue that these trends are having dire consequences on maternal and infant health as well as society as a whole. An increasingly interventionist approach toward birth has led to high rates of unwarranted procedures, but has not produced measurable improvement in healthy outcomes for mothers and babies.
Many medical providers also give women in their care the impression that childbirth can be extremely painful and an out-of-control experience. Based on these fear-laden messages, the mother-to-be learns to distrust the entire process of “natural” childbirth. She begins to view her body as an unreliable incubator that needs to be watched with extreme vigilance, lest she expose her fetus to dangers that can only be resolved through a variety of interventions.
Some common interventions can actually hinder and prolong labor, discourage the mother, and interfere in her ability to maneuver into positions that are more comfortable or conducive to labor.
One such intervention is induction of labor
All too often the following scenario occurs in hospitals in the United States:
Mrs. G., 39, expecting her first baby, arrives at her doctor's office for a checkup at 39 weeks of gestation after an uncomplicated pregnancy, although she had had some difficulty conceiving. She is very pleased with her medical care, and her doctor wants to work with her on her goal to have as normal a birth as possible without drugs. She would like to fully experience the birth.
He suggests that since she is at term and has been eagerly awaiting this baby that they could get things started with some synthetic oxytocin (Pitocin®, Parke-Davis, Pfizer Inc., New York, NY), a method to induce labor chemically. She has been having some twinges of contractions but no cervical changes, and the doctor said that there is no danger to induce labor under these circumstances.
When Mrs. G. received Pitocin, the contractions soon became very painful, and despite the drug, she made “no progress.” No progress means that her cervix was not thinning or dilating and the baby remained high. She was in great pain. No one suggested an epidural because she had said no epidural on her birth plan. Her doula arrived somewhat later, waiting until she was in active labor. In fact, Mrs. G. never went into active labor. But her doula suggested that maybe an epidural would be helpful after 6 painful hours of increasing concentrations of Pitocin, and after staff artificially ruptured her membranes, Mrs. G. agreed and did experience pain relief. The baby descended some, but her cervix never dilated more than 5 cm. Within a few hours it was apparent the cervix was not dilating. After waiting another 12 hours, a” failed induction” was declared, and a cesarean section was performed. Her baby had some respiratory distress and was transferred to the Neonatal Intensive Care Unit (NICU) for 24 hours.
Mrs. G. was traumatized, felt disconnected from the infant, and felt her body failed her, and all her hopes for this birth were dashed.
Issues About Inductions
In this case, we have no evidence that the induction was undertaken for the doctor's convenience, but whether undertaken for the doctor's or the patient's convenience, if there is no specific indication (such as concern for the baby or illness in the mother), the outcome may be quite different than intended. In fact, a cascade of negative events can occur as follows.
Induction is more painful than spontaneous labor. A woman is usually confined to bed with an intravenous drip and continuous fetal monitoring. It usually requires an epidural to contend with the pain. There is increased oxytocin to augment the contractions. If the cervix is not ripe or ready as likely in this case, the induction “fails,” and a cesarean section becomes necessary. Mrs. G. was terribly discouraged and did not feel the baby was hers. In fact, what has actually failed is the appreciation that this woman was not ready for labor. Mrs. G. experienced a cascade of numerous interventions that frequently accompany induction, whether the induction in the end is successful or not.
If the reasons for the induction are valid, such as severe hypertension in the mother that does not respond to medical management, one lives with the potential cascade, but nevertheless a good outcome is more likely than without the induction. Inductions with or without reason will increase the potential for a cesarean from about 8% for labor that begins on its own in a first birth to as much as 40% after the induction.
A fundamental difference here is that the woman's idea of “normal birth” may be quite different from the physician's idea of “normal birth.” The physician caring for Mrs. G. included inductions and perhaps cesarean sections as part of his definition of a normal birth. This was a very different definition than this mother had for a normal birth.
What is missing here is a clear and balanced discussion of the option of induction and all that might result from that decision. And importantly, in this case, the woman did not even ask for an induction and clearly did not understand the ramifications of such a choice when she started. Many women today are misled when told that an induction is a rather harmless method to initiate their labor. Induction is a chemical way to start labor artificially whether the woman's cervix and uterus are ready or not. So the physician took a risk. This induction by the physician involved an error of judgment.
National Survey: Listening to Mothers 1
In a recent article published in Women's Health Issues in 2008, Sakala and Corry 2 described the results of a survey that followed 1,573 women 18–45 years old who gave birth to a single infant in a U.S. hospital. These observations occurred for the childbearing women and their infants from before pregnancy through postpartum.
Although most childbearing women are healthy and at low risk for complications, U.S. childbirth is procedure intensive. Numerous interventions were experienced by the participants, including continuous fetal monitoring (76%), regional analgesia (76%), ruptured membranes (65%), synthetic oxytocin (57%) to induce or speed up labor, forceful staff-directed pushing (75%), fundal pressure (17%), and bladder catheterization (56%). Other common interventions included cesarean sections (32%) and episiotomy (25%) of vaginal births.
Along with numerous interventions many women reported symptoms of depression (63%) and symptoms of posttraumatic stress (18%), especially related to continuing pain if they had a cesarean. Avoidable interventions expose mothers and babies to risk without benefits.
Although 17% of women whose caregivers tried to induce labor suspected large babies as the reason, the best evidence does not support inducing labor for this reason. Numerous other women experienced attempts to induce labor without a medical indication.
Studies suggest that healthy low-risk women could attain much lower rates of interventions with care supporting physiological childbirth and therefore reduce the harm from unnecessary interventions. Few women benefited from practices that are well suited to facilitate normal birth such as fetal monitoring with a hand-held device alone (3%) and highly rated methods for pain relief by mothers such as tubs (6%) and birthing balls (7%).
Cost of Cesarean Sections
With the number of women (32%) (1,280,000 per year) having cesarean sections, multiplying that by $12,000 per section gives the cost as $15,360,000,000 per year 2 (Fig. 1).
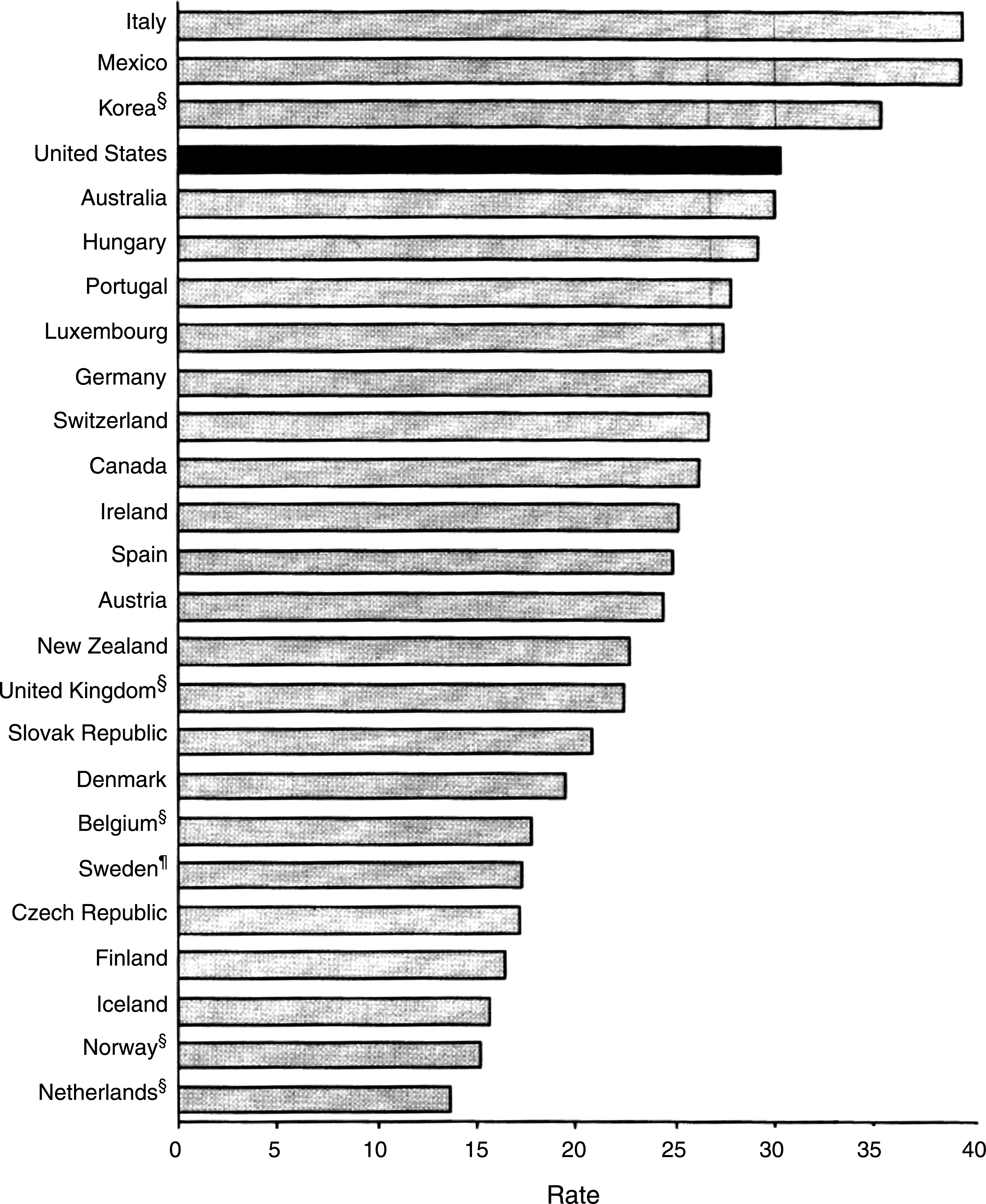
Cesarean deliveries in selected countries in 2005. 2 Rates are per 100 live births. Includes rates from 25 of 30 member countries of the Organization for Economic Co-operation and Development. Recent data on cesarean deliveries were not available from France, Greece, Japan, Poland, and Turkey. §, Based on 2004 data; ¶, based on 2003 data. Source: Prepared by Francis C. Notzon, PhD, National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, Maryland, USA. Reprinted from the MMWR Weekly, September 19, 2008/57(37);1019, Centers for Disease Control and Prevention, Hyattsville, Maryland, USA. Original source: Organisation for Economic Co-operation and Development. OECD Health Data 2008: Statistics and Indicators for 30 Countries. Paris, France: Organisation for Economic Co-operation and Development, 2008. Available at http://www.oecd.org/health/healthdata.
Assuming that we reduce the number of sections as similar to other developed countries such as Sweden and the Netherlands, then only 15% of women need the cesarean section, so the cost in health care is $7,680,000,000 per year. The striking finding is that one of the top 5 most common surgical procedures in the United States is cesarean sections. 3
The Negative Effects of the Epidural
An early epidural given before the mother is in active labor with a cervical dilation of 4½–5 cm can prevent the baby's ability to rotate into the right position for birth. Epidurals also increase the first stage of labor by 4½–5 hours. Likewise, the second stage is increased in length by 1¼ hours.
With an increasing length of labor an epidural raises the temperature of the mother and fetus greater than 38°C for at least 10–15% of mothers. With an increasing length of labor, that percentage could go as high as 30–40% of women.
The fever is a problem because it could indicate an infection in the mother and subsequently a concern about the infant. However, most of the time the fever is a result of the epidural. Generally, this causes a sepsis workup on the infant and an NICU admission.
Other evidence-based effects of increased temperature in the infant include:
Low Apgar scores with a temperature over 38°C were found in 11% of infants. An increase in morbidity such as seizures.
The drugs used in the epidural cross the placenta into the infant and have a longer half-life in the infant than in the mother. Epidural infants are less alert in the first hour after birth, have difficulty latching-on, cry, and are more irritable for 1–3 weeks after birth. A recent Swedish study showed that the epidural infant is more stressed after birth even when breastfeeding. 4
A Finnish study noted that 1 week after birth 67% of epidural infants were on partial or full formula compared to 29% of infants in the control group. 5
From 10% to 15% of epidural mothers did not have a good result because only half of the body received the anesthetic. Lacerations are two times more common because of difficulty in delivery in the second stage. Women given epidurals plus low-dose Pitocin have a threefold increase in cesarean sections rate above normal.
Professor Michael Klein, Chairman of Family Practice at the University of British Columbia in Vancouver, BC, Canada, managed 3,000 patients in his department from 1993 to 2003. He related that he observed in nulliparous women the varying use of epidurals with two groups of doctors. One group used epidurals for pain early 70–100% of the time. The other group used the epidural later, if at all, up to 40% of the time. The frequent users had a cesarean section rate of 23.4% and an increased rate of infants with low Apgar scores with a larger number of infants admitted to the NICU for a few days. The other group had a section rate of 14.8% (M. Klein, personal communication).
The Hormone Story
Hormones during labor and birth can affect the outcome of birth and be critical in a very important way. Many professionals do not recognize the importance of their function. These hormones include estrogen and progesterone, oxytocin, beta-endorphin, and mesocorticolimbic dopamine, and epinephrine, norepinephrine, and prolactin. 6
Let's just concentrate on the hormones that have an effect on pain, are critical to an easy delivery, and are significant in the mother–baby relationship. These are oxytocin, beta-endorphins, and mesocorticolimbic dopamine. They affect the fetus, the baby, and the mother. The natural biological production of those hormones is reduced to very low levels at the start and continuation of an epidural and a cesarean section.
Oxytocin is called the cuddle hormone, the hormone of love. It is terribly important around lovemaking, birth, and breastfeeding.
Let's look at the effect of oxytocin on the mother's emotions and mind. Uvnas-Moberg, colleagues, and others have studied the difference between breastfeeding and bottle feeding mothers in the amount of oxytocin in their blood. 7
In addition to higher levels of oxytocin than in non-nursing mothers, breastfeeding mothers feel less aggressive, less anxious, less suspicious and guilty, less angry or hostile under stressful situations, and generally more positive.
They feel less tense and have less somatic complaints and less muscular tension. Oxytocin-rich mothers reported they felt more attuned to their babies' needs, more relaxed, more comfortable with social contact, and most content to sit for hours feeding, fussing over, focusing on, and studying their infants. Oxytocin causes the final powerful uterine contractions that enable the mother to birth her baby quickly and easily.
Beta-endorphin is one of a group of naturally occurring opiates, and it is secreted by the pituitary. It is secreted under conditions of pain and stress. It acts to restore homeostasis. As the level of beta-endorphin rises, it causes an increase tolerance to pain and induces feelings of pleasure and dependency. It also activates the powerful mesocorticolimblc dopamine to assist it, and together they are as powerful as a very large dose of morphine. However, the natural production of these hormones in the human body does not have any of the negative side effects of the synthetically injected drugs.
We must keep in mind the powerful effects of epidurals and cesarean sections that completely interfere with the three natural hormones that deal with pain.
Maternal Morbidity and Mortality Related to Cesarean Sections
After a cesarean section there is an increase in subsequent pregnancies of all types of abnormal attachments of the placenta to the wall of the uterus, such as placenta previa, where the placenta attaches to the cesarean scar over the cervix, or placenta abruption, which is a separation of the placenta from the uterine wall. Other problems include ectopic pregnancies, infertility, miscarriages, and unexplained stillbirth. Surgical adhesions leading to bowel obstruction may occur even many years after the surgery. 6
Surgical morbidities are found in excess in cesarean sections. These include wound infection, infection of the blood, lungs, clots in the veins of the legs, and blood loss. Injury to the bladder is four times more common in elective cesarean sections when a woman has a previous scar on her uterus. U.S. figures for maternal mortality rates: The risk of the mother dying after elective (non-emergency) cesarean is 5.85 per 100,000 versus 2.06 per 100,000 vaginal deliveries. 6
Newborn Mortality and Morbidity
Large population surveys have found babies delivered by cesarean to be two to five times more likely to need intensive care nursery compared to vaginal deliveries. 9 Many of these babies are preterm. Breathing difficulties in cesarean section-delivered babies are 6% compared to 3% in vaginally delivered babies. Persistent pulmonary hypertension is 4% in 1,000 elective sections compared to 0.8 in 1,000 vaginal deliveries. There is higher infant death in cesarean section-delivered babies (1.7 per 1,000) versus (0.68 per 1,000) vaginal. Babies born vaginally benefit from taking in the mother's intestinal flora and having all their bodily organ, immune, and hormone systems activated through a normal labor.
How to Facilitate Normal Birth
When a woman during labor is supported emotionally and physically and the birth is allowed to proceed normally without unnecessary medical interventions or physical interruptions the experience can be transformative for the mother and healthy for both the baby and mother.
Making normal birth a reality was developed by the Maternity Care Working Party in the United Kingdom, an independent, multidisciplinary body that campaigns for improvement in maternity care. 10 The document is endorsed by the United Kingdom's Royal College of Obstetricians and Gynaecologists, the Royal College of Midwives, the National Childbirth Trust, and other organizations. It calls for the healthcare system in the United Kingdom to collect statistics on the normal birth/delivery.
They define normal birth in the following way: without induction, without the use of instruments, not by cesarean section, and without general, spinal, or epidural anesthetic before or during delivery. They aim to increase normal birth rates towards a realistic objective of 60% by 2010. It is 48% currently.
They also offer a choice of place of birth, including home birth, a midwife-led birth center, and a maternity unit with midwifery and medical facilities, and the chance for women to get to know their midwife prior to labor.
Valuable Effects of Doula Care on Labor, Birth, and Postpartum
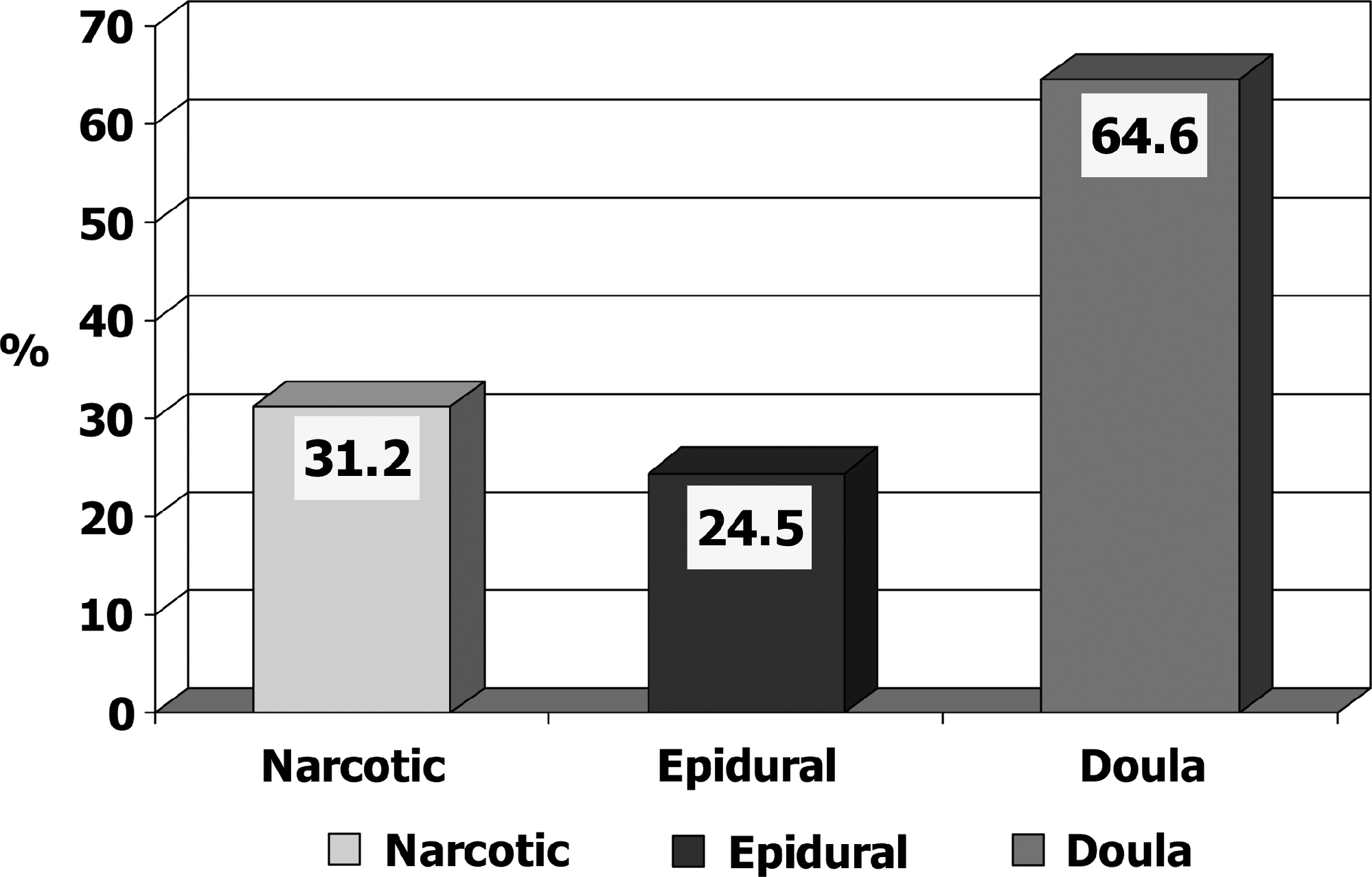
Since 1975 we have been studying the role of a support person for women during labor. The studies demonstrated that labor was shortened by 25% with the presence of a doula who was with the mother continuously. The cesarean section rate was reduced by 45%, pain medication to the mother was reduced by 30%, use of forceps by 40%, and epidural use by 30–60% (Fig. 2). 11 Six weeks later studies of the doula-supported mothers noted breastfeeding increased compared to controls, anxiety and depression was reduced, and the doula mothers were more responsive to their babies than the controls (Table 1). 12 Altogether 15 randomized trials done throughout the world have demonstrated similar results. 13

Data are from Wolman et al. 12
Highly significant difference.
In order to test the effectiveness of a lay doula trained only for 4 hours with the mother, low-risk, poor, first-time mothers attending a clinic were randomized. One group had a close female friend or relative as the doula; the other group was the control. The lay doula group had significantly shorter labors and greater cervical dilatation at the time of epidural analgesia. The cesarean section rate was 10.6% in the doula group versus 15.5% in the control (p < 0.09). Although not statistically significant, there was a trend towards lower rates of cesarean surgery in the doula group.
One of the most important themes of all the studies has pointed out the power of emotional and physical support at one of the most vulnerable times in a woman's life. This effect lasts beyond the birth and is illustrated in the mother's behavior, her feelings about herself, her infant, and her partner 14 (Table 2 and Fig. 3).
Breastfeeding initiation rates in the Houston study by McGrath et al. 14
Data are from McGrath et al. 14
Of the women who were assigned to an epidural 12.5% did not accept it.
Compared to the control group, the doula mothers 6 weeks later who were cared for by lay doulas trained for only 4 hours were more likely to describe labor as very easy and reported that labor was much better than they imagined and that their birth experiences were very good. They described their babies as very easy and believed their babies cried less often. They were more likely to pick up their babies when they cried and to report that they were able to sense their babies' needs. They noted that the transition to motherhood had been very easy 15 (Table 3).
Data are from Campbell et al. 15
Conclusions
To correct these high cesarean rates in the United States, we highly recommend the following:
Use the British example to allow labor to start on its own. Avoid any unnecessary interventions such as inductions and epidurals. Every mother should have a doula to reduce all the complications of labor. Because of all the problems with epidurals, we recommend that their usage be significantly reduced. Mothers should use a variety of known pain-relieving nonmedical methods, including hypnosis training, massage, warm baths, etc. Allow the natural hormones, especially the three pain-reducing hormones, oxytocin, beta-endorphin, and mesocorticolimbic dopamine, to do their job and get the mother through labor with greater satisfaction.
It will be important for the care providers, nurses, doctors, midwives, and doulas to have a joyful, respectful, and humane attitude toward this new family, and this will undoubtedly create an emotional holding environment for the new bond to grow between the parents and their infant.
Winnicott
16
describes it in this way:
There is a most curious thing happening: the mother who is perhaps physically exhausted, and perhaps incontinent, and who is dependent on the nurse and the doctor for skilled attention in many and various ways, is at the same time the one person who can properly introduce the world to the baby in a way that makes sense to the baby. She knows how to do this, not through any training and not through being clever, but just because she is the natural mother. But her natural instincts cannot evolve if she is scared, or if she does not see her baby when it is born, or if the baby is brought to her only at stated times thought by the authorities to be suitable for feeding purposes. It does not work that way. The mother's milk does not flow like an excretion: it is a response to a stimulus, and the stimulus is the sight and smell and feel of her baby, and the sound of the baby's cry that indicates need. It is all one thing, the mother's care of her baby, and the periodic feeling that develops as if it were a means of communication between the two—a song without words.
Footnotes
Disclosure Statement
No competing financial interests exist.