
Abstract

The Health Policy Frontier Today
We have done those things we ought not to have done,
We have left undone those things we ought to have done,
And there is no health in us.
Important problems remain unaddressed, the most central of which (from my perspective) include (1) the failure to counteract numerous financial distortions that create adverse incentives throughout the healthcare system, (2) the failure to attack the widespread regional differences in the use of health care for similar populations (including learning which of the rates is “best”), (3) the nearly complete omission of ways to improve people's lifestyle choices and their effects on their own health, the health of those in their family, and the costs to the healthcare system from poor health resulting from those choices, and (4) the continued emphasis on acute post-illness treatment rather than focusing on primary and secondary prevention to reduce the underlying illness burdens in our society. 1
This article will focus on the closely intertwined final pair on this list—lifestyle choices and prevention—and discuss the ways healthcare financing can improve patterns of breastfeeding in this broader context.
First, let's take a look at the big picture. In an extraordinary article in 1993, McGinnis and Foege 2 analyzed the “true” causes of death by estimating the excess deaths from multiple diseases arising from various choices people can make about how they live their lives. Their work, using 1990 data, was repeated in 2004 using 2000 data by Mokdad et al. 3
Two remarkable things appear in those works. First, by far the leading killers in our society directly involve our own behavior. The top two on the list—tobacco use and obesity/lack of exercise—account for over one-third of all deaths, and alcohol abuse brings the total to over three out of every eight deaths. While other substance abuse appears further down the list, its importance pales in comparison to the top three true causes of death on this list—tobacco, obesity, and alcohol abuse. The second observation is that obesity will soon overtake tobacco as number 1 on the list. We are in the midst of an obesity epidemic in this country, and we're doing almost nothing meaningful to stop it. When the next update of this research appears (probably using 2010 data), we can confidently estimate that obesity will sit at the top of the list.
The rising relative importance of obesity comes from multiple sources, all of which shed some light on the issues of breastfeeding, on which we focus later in this article. The first is that we have had at least some success on the issue of tobacco, leading (happily) to its slipping in importance as we look into the future. The second is that we face a tidal wave of fat sweeping the land at an increasing rate. It is useful to understand the causes of both the decline in tobacco use and the increasing obesity before we turn to ways to think about breastfeeding as a national policy issue. What can we learn from these two illness-producing (“sickie”) behaviors?
Tobacco and Obesity: A Tale of Two “Sickies”
The issues created by tobacco and obesity have important similarities to the issue of breastfeeding. With tobacco, the issues of secondhand smoke and children's asthma (and other important diseases) remind us that parental behavior can affect the health of their children directly. With obesity, we know that breastfeeding, particularly done for long duration and best when exclusively, reduces the risk of obesity, in addition to providing improved immunity against various diseases, reductions of deaths due to sudden infant death syndrome, necrotizing enterocolitis, and other diseases. So let us begin with an excursion into these two dominant public health issues—tobacco use and obesity to see what we might learn about breastfeeding issues.
Tobacco
The War on Tobacco, while still not won, has shown important progress. Then–Surgeon General Luther Terry convened in 1964 a group that summarized what was known about the perils of tobacco, 4 and that report initiated numerous changes in law, attitudes, and behavior that have led to a remarkable (but still incomplete) reduction in tobacco use.
Figure 1 5 shows the main story: After decades of increasing tobacco use, the trend reversed in 1965, with the downward trend continuing now for almost half a century. Surgeon General Terry probably saved more lives by creating that report than any other physician in world history. We should not forget the changes in policy that buttressed the initial study's effect. Cigarette package labeling became routine. Television advertising for tobacco ceased, and numerous anti-smoking ads appeared. State and local governments banned smoking in public places, and federal law banned smoking on airlines. Tobacco taxes increased in many sectors of the economy, thus raising the price of smoking and helping reduce its use. Pharmaceutical products and support programs emerged (with varying effectiveness) to help people stop smoking. Cumulatively, they led to the changes in behavior portrayed in Figure 1.
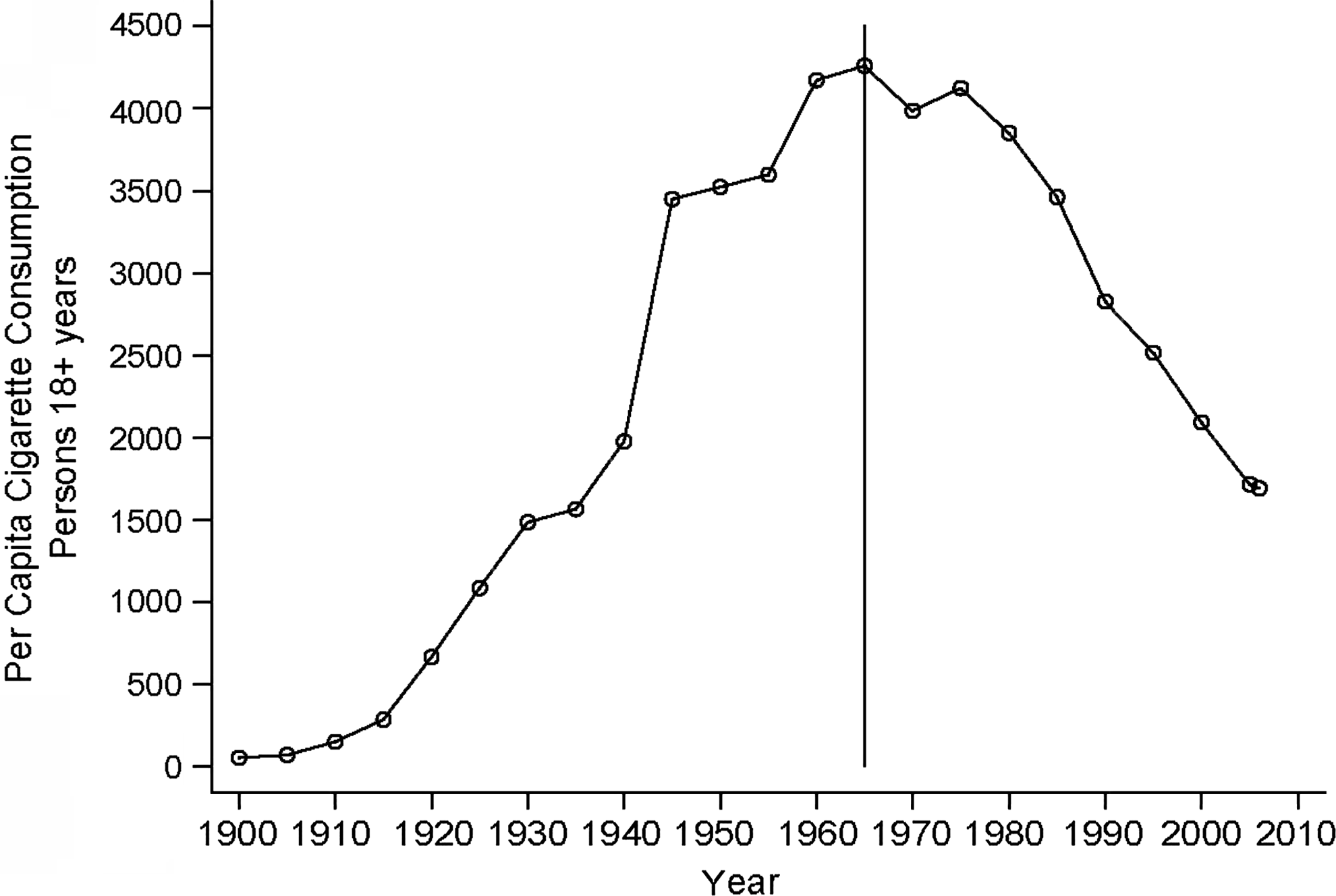
Adult U.S. cigarette consumption per capita. Reproduced from National Center for Health Statistics, 5 Table 60, pp. 275–276.
Obesity
Obesity creates a more dismal picture. Recent trends in obesity and participation in vigorous exercise show that the United States is in the midst of an obesity epidemic of (pardon the expression) large proportions. Figure 2, using data from the National Health and Nutritional Examination Survey, 5 shows the time trends in the United States for the percentage overweight (25 kg/m2 < body mass index [BMI] < 30 kg/m2) and obese (30 kg/m2 < BMI < 35 kg/m2). At present, two-thirds of U.S. adults are overweight (BMI > 25 kg/m2), and half of these are obese (BMI > 30 kg/m2). While recent research suggests that other measures (such as waist/height) may have even greater predictive power than BMI, let us not get sidetracked by this issue: The evidence is clear that we have (since about 1975) an increasing proportion of the U.S. population—both adult and adolescent—who are either overweight or obese.
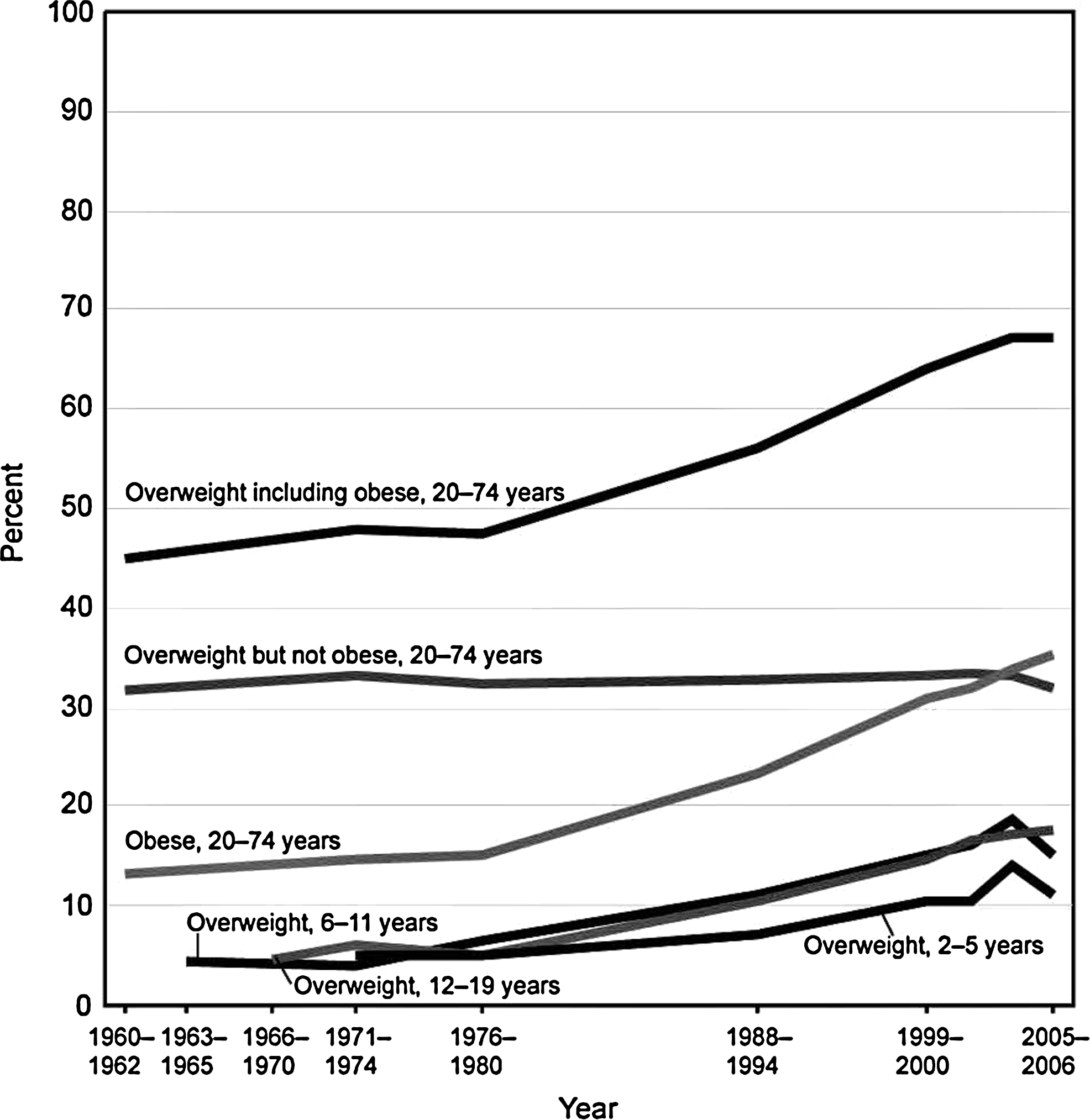
U.S. trends in overweight and obesity. Reproduced from National Health Examination Survey and National Health and Nutrition Examination Survey, National Center for Health Statistics, 5 Fig. 7.
We also have to face the hard truth: Fat kills. A meta-analysis of 57 prospective studies of obesity and mortality summarized the results for over 900,000 lives. 6 It shows a strong relationship between obesity and both all-cause mortality and many specific-cause mortalities. Once a person moves either above or below a BMI range of about 24–26 kg/m2, mortality increases. Low BMI is unhealthy, just as is high BMI, but the problem our nation faces in general is the growing obesity rate, not the other side of the curve. If we bow to political correctness, we will never fully confront the issue: Fat kills. It also adds to many conditions that reduce the quality of life, including inability to carry out activities of daily living, more difficult travel and participation in public events, and participation in active sports, and, yes, it even increases the risk of erectile dysfunction. It also increases the risk of other diseases that can debilitate a person, including most prominently heart disease, diabetes, knee and other joint injuries, and many others.
While one cannot pinpoint any single cause for the growing obesity trend, some notable issues emerge, many involving basic economic concepts, and again with attained education emerging as a key. First, because of mostly technological gains in both plant biology and mechanized farming methods, food has become increasingly cheaper through time. Second, as the general educational level of the population increases, people's time becomes more valuable.
With this increase in the value of time come three important phenomena—jobs become more sedentary (and hence less caloric expenditure), the time to otherwise shed calories becomes more valuable (raising the “price” of exercise), and meal preparation becomes relatively more expensive. As time becomes more valuable, people will naturally turn to prepared foods within the home or eat away from home in restaurants and fast-food establishments. (For a more complete analysis of these issues, see Philipson et al. 7 )
This brings to our attention yet another trend, highlighted by the research of Young and Nestle 8 : Food proportions have become increasing large through time, both in prepared food for the home and especially in restaurants. An interesting online quiz from the National Institutes of Health (NIH) emphasizes the same phenomenon. 9 Both the Young and Nestle 8 analysis and the NIH survey 9 find prepared food proportions at least double the size now as they were 20 years ago. As one can readily observe by watching TV for a few hours, food chains generally compete on the size of their food servings.
This may be part of the cause of growing rates of childhood obesity. We cannot, of course, link childhood obesity to reduced caloric expenditure at work, but the shift of dining away from home to restaurants (and, importantly, snacking between meals) provides at least a plausible link. Families dine out together often now, and children spending weekends at shopping malls will encounter numerous opportunities to snack between meals.
These and other phenomena converge to cause the fat tsunami approaching the U.S. healthcare shoreline. Currently, the direct health expenditures attributable to obesity add $150 billion annually to the U.S. healthcare budget annually, and tobacco-related illnesses add $100 billion in direct medical care costs and an equal amount in lost productivity. 10
One might think, given the importance of these two behavioral phenomena alone, that U.S. investments in biomedical and socioeconomic research would target tobacco and obesity directly with massive research investments, comparable in scale to those on heart disease ($2.9 billion), cancer ($4.8 billion), stroke and other neurologic disorders ($1.5 billion), and acquired immune deficiency syndrome (AIDS) ($3.0 billion).
But it doesn't happen that way. Our NIH budgets, focused by disease category and mostly directed at “basic” biological research, have little identifiable resource allocation on these two issues. In the most recent steady-state data available, 11 the NIH spent $310 million on tobacco-related research and $664 million on obesity research, with the latter spread across 26 units of the NIH. More people die annually in the United States from tobacco use and obesity (about 850,000 per year 3 ) than in the entire history of the AIDS epidemic (545,000), yet the funding for AIDS research in the NIH budget (about $3 billion per year) is 10 times of that for tobacco and five time of that for obesity research.
The same apparent disregard of the value of breastfeeding appears in NIH priorities. While incomplete breastfeeding does not create the same overall risk as AIDS, it creates about 5% of the deaths annually as AIDS (see Importance of Breastfeeding, The costs of incomplete breastfeeding, below). Yet it would be impossible to find NIH programs and research of proportionate scale (i.e., about $150 million annually) on ways to increase breastfeeding rates.
An Excursion into General Education and Healthy Behavior
One phenomenon of importance here is the role of general education and how it affects behavioral and lifestyle choices. As described in more detail in Phelps, 1 we can observe strong relationships between educational attainment and virtually every lifestyle choice that people make. More highly educated people live healthier life styles.
As a prime example, the shift in smoking behavior shown in Figure 1 has not occurred consistently across all segments of the population. One facet of the demographics of smoking cessation provides a particular interest—the role of educational attainment in smoking cessation. Figure 3 shows the time profile by educational level 5 —a pattern we can see repeated in other lifestyle choices.
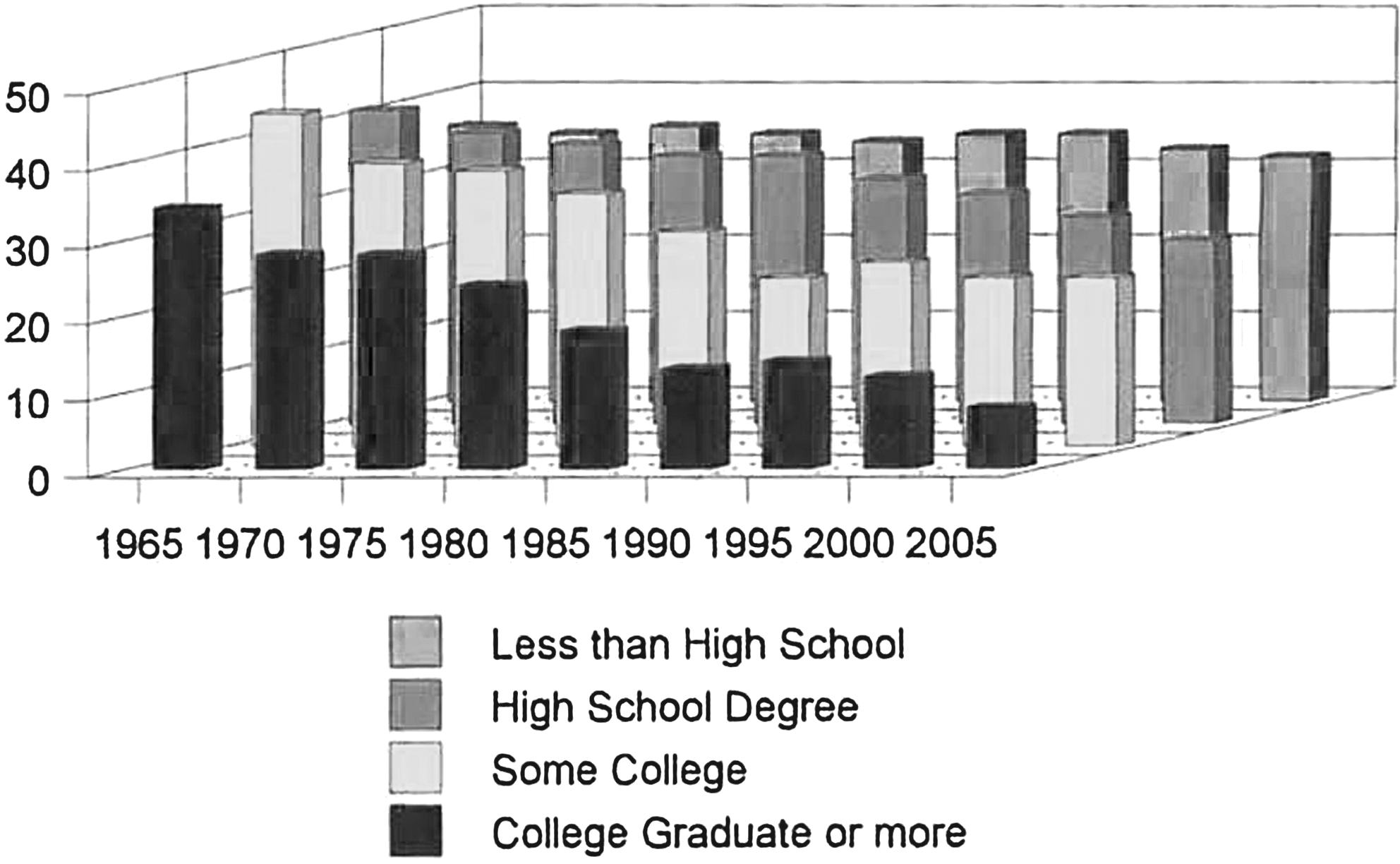
U.S. adult smoking participation over time by educational attainment. Reproduced from National Center for Health Statistics, 5 Table 6, p. 278.
In 1965, while different educational groups had different smoking rates, they were not all that different (35–45% participation rates by education group). Indeed, smoking was portrayed as a symbol of sophistication in movies, in literature, and (of course) in advertising. By 2000, smoking rates remained almost unchanged among those with the lowest educational attainment but had plummeted from 35% in 1965 to 9% in 2005 among those with a college degree or more. Intermediate levels of education show a strong dose–response relationship: The more education, the more people respond to the information about the hazards of smoking.
Obesity rates are also lower and participation rates in recreational exercise higher in more highly educated people. Figure 4 shows obesity rates by educational attainment. 12
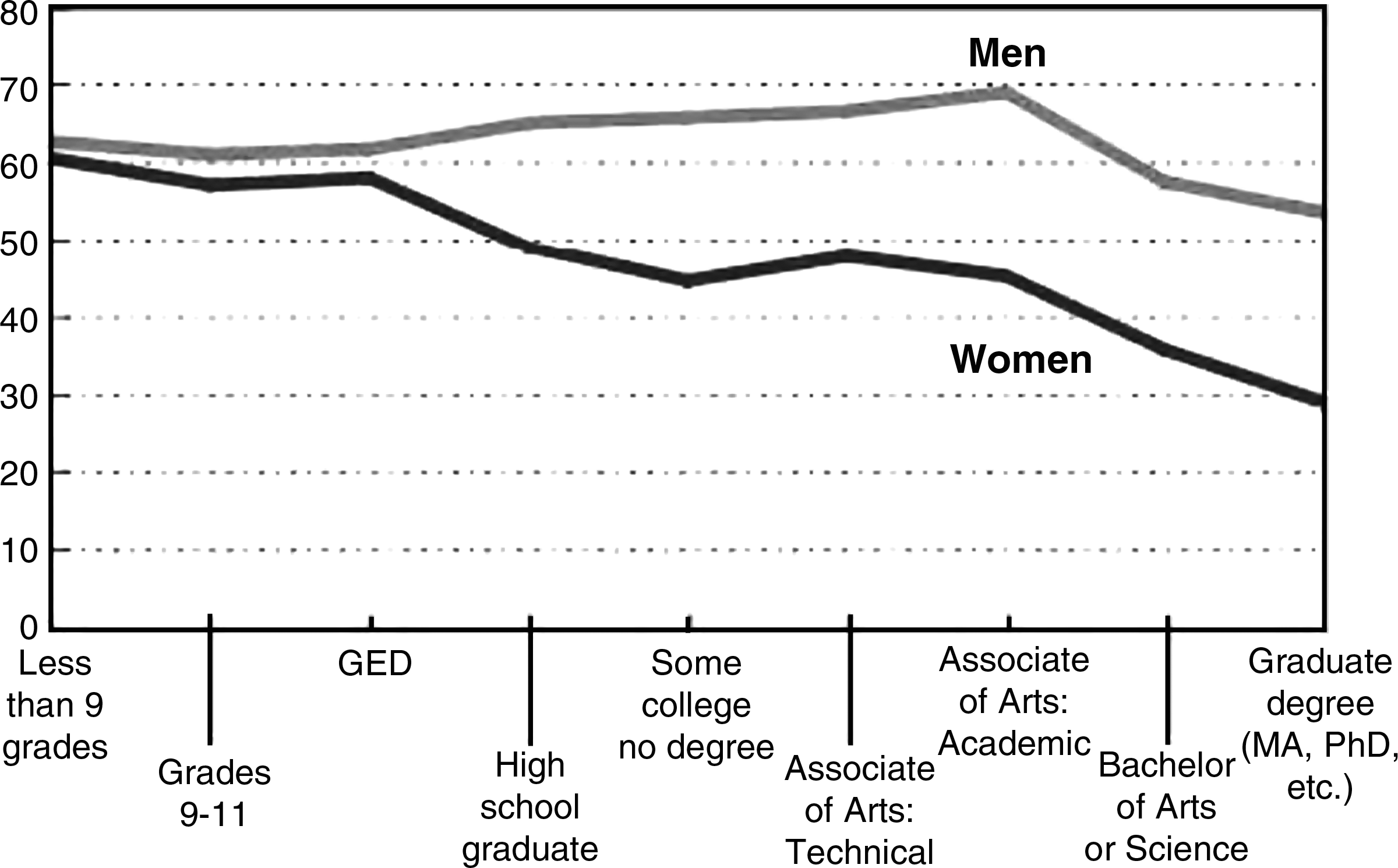
U.S. overweight and obese adults by educational attainment. GED, general equivalency degree. Reproduced from Schoenborn et al., 12 Table 2, p. 12 (www.cdc.gov/nchs/data/ad/ad330.pdf [accessed July 15, 2010]).
Alcohol abuse occurs less frequently in more highly educated people, as well as a shift from more harmful alcoholic beverages to wines, which can confer health benefits if drunk in moderation. 1
Finally, we can observe strong positive relationships between educational attainment and breastfeeding rates. According to data in Li et al., 13 breastfeeding rates increase with education from high school through college (and higher) degrees both for any breastfeeding and for exclusive breastfeeding at every duration measured. Thus, one way to increase healthy behavior (including breastfeeding) is to improve our K–12 educational system, which is generally acknowledged as falling far behind that of most other developed countries. 14
Importance of Breastfeeding
Benefits of breastfeeding
First, let's summarize the known benefits of breastfeeding in terms of health outcomes and healthcare costs. As is widely understood, breastfeeding reduces the risk of many childhood illnesses, including otitis media, diarrhea and other intestinal disorders, sudden infant death syndrome, necrotizing enterocolitis, allergies, childhood asthma and eczema, Haemophilus influenzae type B, respiratory syncytial virus and other respiratory illnesses, herpes simplex, gastric reflux, and even inguinal hernia and cryptoorchidism (through hormonal transmission). It also appears that breastfeeding increases cognitive and social development. A 2000 publication from the Office on Women's Health, Department of Health and Human Services, summarizes these benefits and relevant literature citations. 15
Given the growing importance of obesity in the United States, it is also important to understand the effects of breastfeeding on obesity. From the literature on breastfeeding, particularly as it relates to adolescent obesity, the best evidence summarizing a large number of studies in a careful meta-analysis shows a consistent dose–response effect on duration of breastfeeding and later risk of the child's obesity. Harder et al. 16 summarize these results by saying, “The risk of overweight was reduced by 4 percent for each month of breastfeeding. This effect lasted up to a duration of breastfeeding of 9 months and was independent of the definition of overweight and age at follow-up.” The odds ratio of being overweight for a child breastfed up to 9 months is two-thirds of that for children not breastfed.
Breastfeeding goals
The Healthy People 2010 objectives for breastfeeding in the early postpartum period, at 6 months, and 12 months are 75%, 50%, and 25%, respectively. A far more ambitious goal comes from the American Academy of Pediatrics task force on breastfeeding, 17 which recommends exclusive breastfeeding for the first 6 months of a child's life and supplemented breastfeeding for 1–2 years.
How does actual behavior correspond to these goals? National data on exclusive breastfeeding are available only from respondents interviewed after 2005 and thus are not available for children born prior to 2003. No method of measuring rates of breastfeeding is “perfect,” 18 but the general data trends all show similar patterns. Breastfeeding initiation has increased through time (with a puzzling dip in the 1980s), but persistence to 3 months, 6 months, and 1 year or more shows a steady fall-off in breastfeeding as the infant grows older. Exclusive breastfeeding always occurs less regularly than supplemented breastfeeding. As a general summary, current breastfeeding rates are near but have not yet surpassed the Healthy People 2010 goals, and the proposed 2020 goals adopt the 2010 goals for breastfeeding with no changes.
Regular survey data from the National Immunization Survey now provide a general indicator of breastfeeding rates, and analysis of these data (e.g., Li et al. 13 ) shows systematic links between various maternal characteristics (race, income, Special Supplemental Nutrition Program for Women, Infants and Children status, educational attainment, etc.) and breastfeeding rates.
The costs of incomplete breastfeeding
A newly published analysis of the costs of incomplete breastfeeding 19 carefully assesses the healthcare costs and the economic loss of early death from incomplete breastfeeding. The authors estimated reductions in illness and death that would occur if we achieved 90% or 80% compliance with the recommendations of the American Academy of Pediatrics on breastfeeding. 14 If we could achieve 90% compliance, annual deaths would fall by an estimated 911 per year (mostly due to reductions in sudden infant death syndrome, necrotizing enterocolitis, and lower respiratory tract infections), healthcare costs (direct and indirect) would fall by $3.4 billion per year (about $850 per birth in the United States), and the cost of foregone lives (using standard economic valuation techniques) would fall by $9.6 billion per year ($2,300 per birth). Achieving “merely” 80% compliance would still capture many of the benefits of 90% compliance.
These data provide important benchmarks on how much money might be available out of the healthcare financing system to improve breastfeeding rates. If activities could be shown to increase rates of breastfeeding, it might be possible to shift funds from paying for acute medical care (hence saving insurance costs and health insurance premiums) to improving childhood health through improved breastfeeding participation and duration by mothers.
Why Is This a Public Policy Issue?
We should begin with the obvious question—why might we think that individual choices about breastfeeding do not lead to the desirable (“optimum”) amount of breastfeeding (which is not 100% compliance, for a variety of reasons)? Several ideas emerge from the world of economics, generally falling in the realm of “externalities.” Externalities occur when one person's behavior makes others incur extra costs (or provides extra benefits) that individual decision-makers do not take into account when they make their own decisions. Air pollution, traffic congestion, and noise pollution at the beach are classic examples. In health care, three others emerge prominently.
Infectious diseases and herd immunity
One child's immunity reduces the chances of other children becoming sick. Thus “herd immunity” provides a classic “public good” reason for subsidizing prevention that reduces the incidence of infectious diseases. Breastfeeding has known benefits by increasing natural immunity of breastfed children against various infectious diseases, even without proper childhood vaccinations, but also in addition to vaccine programs because naturally conferred immunity has a broader set of diseases covered than does any artificial vaccination program.
Financial externalities
Individuals do not bear the full costs of their choices. Health insurance buffers us from the costs of illness and injury. Employer-provided and social insurance programs (Medicare, Medicaid, TriCare, Veterans Administration health care, State Children's Health Insurance Program, etc.) buffer us from the full costs of actually purchasing health insurance. And, with employer-paid insurance, the tax-exempt status of employer premium contributions further hides the true cost of insurance from decision-makers. All of these mechanisms push in the same direction—insufficient attention to preventive care and proper lifestyle choices for individuals. The same hold true for breastfeeding, with other important complications to be discussed below.
The special issue of obesity
With one of the major economic and social issues of our time centering on the costs of health care, one can only look at the growing rates of obesity in our country as the potential for a financial catastrophe. In June 2010, the head of the U.S. Federal Reserve Board spoke to Congress about the looming federal deficit, specifically including concerns about growing healthcare obligations from Medicare and Medicaid. Increasing obesity adds to these risks. To the extent that increased breastfeeding has significant potential for reducing future obesity rates, the value of public intervention to enhance breastfeeding rates increases. Specifically, because obesity adds to healthcare costs but insurance premiums (both private and public plans) do not charge extra for obesity, obese people do not bear the full costs of their extra health care in general, thus making obesity prevention a natural issue for public policy intervention.
How Might We Increase Breastfeeding Rates?
This brings us to the crux of the matter: How do we span the chasm between current behavior and a healthier pattern of breastfeeding in our country? As a preliminary observation, ultimate success will eventually hinge on achieving greatly improved rates of duration of breastfeeding, not initiation itself. Rates of initiation of breastfeeding in the hospital are high, but continuation past 3 months, and more desirably 6 months or more, occurs much less often. Efforts to increase initiation rates alone will fail if we do not achieve much higher rates of continued breastfeeding far past the early weeks of initiation—6 months or more, most desirably, according to breastfeeding experts.
No magic wand exists that we can wave over the landscape and transform human behavior. It will require multiple interventions—including some not yet imagined—extending over decades. The tool kit includes education (both general and specific), changes in incentives facing mothers, healthcare providers of many sorts, and insurers, and shifts in population attitudes towards breastfeeding. Let us address these in turn.
Education
Specific education
We have a clear picture from the history of tobacco use that specific information about the perils of tobacco altered people's behavior. It began with warning labels on tobacco products, extended to prohibitions on advertising for tobacco on television, an extensive countersmoking campaign with ongoing support from both government and private sources (most notably the Advertising Council), federal bans on smoking in airlines, numerous state and local laws gradually eliminating smoking in public settings, and finally even private organizations banning smoking in ways extending beyond those required by public law.
General education
As we have seen in An Excursion into General Education and Healthy Behavior, in the cases of tobacco use, obesity, and alcohol abuse, general education can have profound effects on people's choices about lifestyles that affect the health of themselves and those around them. The same occurs with breastfeeding, as reported by Li et al. 13 The largest effects come from completion of college education: College graduates breastfeed at about twice the rate of high school graduates at any duration of breastfeeding.
This link in many ways comes as more of a surprise than the link between educational attainment and other healthy behaviors. In general, education raises the value of time, and as we all know, breastfeeding requires a commitment of time beyond that of bottle feeding. So somehow other factors associated with education—better ability to assimilate specific information, a longer time horizon, and different sets of peer support and pressure, among others—somehow overcome the time-cost burden of those more highly educated.
Correcting financial distortions created by health insurance
For better or for worse, our health insurance system contains a systematic tilt towards acute treatment of disease rather than prevention. These distorted incentives occur at all levels of the healthcare financing system, from those facing individual patients and providers to those facing health insurers themselves. Let us explore these issues in more detail.
Individual choices
Health insurance pays for much of the cost of medical care, thus creating incentives to use more than when uninsured. It accomplishes this by subsidizing the price of medical care at the point of use, but it does so asymmetrically. Preventive medical interventions are often not covered, particularly those involving lifestyle choices such as tobacco use, caloric intake and exercise, alcohol abuse, unprotected sexual activity, and breastfeeding. As the consequences of getting sick are reduced by insurance coverage, people naturally invest less effort and time to prevent events that insurance covers. Of course, few if any people really enjoy getting sick (or having sick children), but the tendency to let preventive measures “slide” is enhanced when health insurance covers most of the medical costs of illnesses, particularly when those activities (smoking, eating, and sexual activity) provide intrinsic pleasure.
One can envision multiple ways to offset these incentive problems, including (most obviously) counseling and coaching provided by either healthcare providers or social network groups (“clubs”—think of Weight Watchers or Alcoholics Anonymous) or direct financial incentives to mothers:
Individual incentives. Imagine for a moment (without considering how to finance or administer such a program) the existence of a reward program that paid mothers a significant amount of money to complete (say) 3 months or 6 months of breastfeeding, with higher rewards for exclusive breastfeeding than for supplemented feeding (because the health benefits of exclusive breastfeeding exceed those of supplemented feeding). The economic value of such programs comes from the possibility of reducing medical care expenditures by up to $3.4 billion per year in the United States, not to mention saving the nearly $10 billion per year in the costs of early deaths. 18
Counselors, support groups, advisors. Health insurance suggests another mechanism to increase breastfeeding rates: Creation of insurance payments to counselors, coaches, and others to compensate them for the time and costs of providing breastfeeding support services. Currently a pediatrician might be able to bill modestly for such services as part of a routine office visit, but such mechanisms are not available to other potential providers of advice, education, and counseling, including (to name but a few possibilities) visiting nurse services, certified lactation counselors, support groups (akin to Alcoholics Anonymous—perhaps we could call them Bottle Feeders Anonymous), or even commercial endeavors akin to weight reduction programs (e.g., Weight Watchers) or exercise programs that now commonly charge for participation.
Each of these paths involves expenditure of resources by some entity—private or government—either to reward mothers who breastfeed regularly or to invest in resources in programs that counsel and support breastfeeding (or both—these are not mutually exclusive endeavors). How might society pay for such activities?
Insurer and employer incentives
In addition to gains and costs (incentives) for individual persons, lifestyle behavior and medical care choices create costs and benefits for health insurers and employers, most notably reduced insurance payments and reduced sick-day and disability insurance paid by others. In an ideal world, insurers and employers would account for this, e.g., by rewarding insurance enrollees and employees (respectively) to undertake preventive activities up to the point where the incremental incentive payments just balanced the incremental savings or by investing in counseling and coaching programs (offered by healthcare providers or others) to encourage the desired activity (in the current case, breastfeeding).
But, insurers and employers often have greatly reduced incentives to undertake such efforts because of worker mobility. Employer efforts spent on prevention and lifestyle improvement go for naught if the worker has moved to a new employer by the time the intervention takes effect. Insurers (particularly those insuring through workplace groups) have even weaker incentives to subsidize prevention and lifestyle improvement because they lose benefits not only as workers shift jobs but also as they shift insurance plans within the same job.
Both of these represent a classic problem in non-cooperative game theory. Because much of the benefit from any outlay for prevention accrues to some other entity, the optimal solution for each participant in this economic “game” is not to spend money on prevention. Thus both employers and insurers will underinvest in prevention in any competitive economic equilibrium. We also know that the further in the future any benefits occur, the less likely will employers or insurers invest in prevention.
The problem is confounded even more for employers if the benefits arrive through improved health of spouses and children of employers, from whom the employer receives no productivity gains. Indeed, time taken off by breastfeeding working mothers (either through maternity leave or “down time” during the day for breastfeeding or milk expression) will, if anything, reduce employee productivity. This is why (for example) firms commonly provide stronger insurance benefits for their employees than for the families of employees. They capture some of the improved health of the worker through improved job productivity, but they will capture little (if any) of the value of health benefits accruing (for example) to children of workers.
Fixing the problems
Two ways (at least) exist to fix the problem of insurer incentives (only some of which apply to employers through workplace health programs), both with tried-and-true histories in the United States and with some important examples of success in areas such as tobacco use and alcohol abuse.
Regulation
The first approach has a long history of application in the United States—mandate by regulation. We do this in numerous workplace rules (for employers) and numerous health insurance benefit choices (for insurers), including requirements for coverage of various kinds of diagnostic tests, infertility treatment, and the like. Such rules have strong political appeal because they keep the expenditure “off budget,” hence not increasing the apparent size and influence of the government on private sector behavior. But, they also mask the true cost of the program from the body politic.
Federal and state governments have a long history of mandating that private health insurance cover various types of care, including not only traditional medical services but also mental health treatments, and more recently infertility treatments, minimum standards on hospital stays for childbirths, and many others.
In a recent example of mandated behavior, the Affordable Care Act of 2010 mandated (by amending the Fair Labor Standards Act) that large employers be required to allow (unpaid) time off for nursing mothers, as well as requirements for providing them with private setting for breastfeeding (that were not public use bathrooms). Small employers facing “undue economic hardship” are exempted from these requirements.
Coverage of breast pumps by health insurance has little uniformity, leaving many mothers uncertain as to coverage, limits of payment, requirements for prescriptions (as if breastfeeding were a disease to be treated), or time delays to process requests. One simple change in healthcare financing that would enhance breastfeeding rates would mandate coverage of breast pump costs universally across all health plans, both private and governmental. While some plans provide such coverage now, it often comes only upon special requests or appeal.
Tax/subsidy schemes
Economists always think about incentives and prices, with the primary mechanism for altering incentives coming from levying taxes (as with alcoholic beverages and recent increases in federal tobacco taxes). We often subsidize behavior deemed as desirable, most notably by using the federal tax system via deductions from taxable income (e.g., for home mortgage interest), tax credits (e.g., for renewable energy investments), or exclusion of otherwise taxable income from the income tax base (most notably, employer-paid insurance premiums). The tax exemption of charitable enterprises in our country [via Internal Revenue Service section 501(c)(3)] confers economic advantages to organizations carrying out activities deemed socially desirable by the Internal Revenue Service (education, religious organizations, some but not all healthcare providers, etc.).
One can envision a tax/subsidy scheme involving preventive health care in general and breastfeeding in particular. For example, suppose analysis showed that (optimally) we should spend 1% of all healthcare dollars on obesity prevention, and insurers currently captured (and hence found it sensible to spend) only 10% of that via reduced health coverage outlays. Then social well-being could be improved by levying a tax on health insurers of (say) 0.9% of premium dollars and returning those funds to insurers based on their proven efforts in supporting the desired preventive activity.
The same idea could be used for breastfeeding-enhancement programs. For example, a tax of 0.1% of all health insurance premiums (including all federal and state programs) would create revenues of (in very rounded terms) $2 billion annually, notably less than the $3.4 billion spent on treating the illnesses deriving from incomplete breastfeeding rates, but still an enormous resource to promote breastfeeding. If effective programs could meaningfully use such resources (both private incentive payments to mothers and programmatic support) to increase breastfeeding rates—and hence to offset otherwise-spent medical care costs—it might be possible to divert funds of this sort from acute healthcare payments towards prevention of disease. One might also think about taxing commercially provided supplemental formula sales, but that would of course raise the cost of a vital resource to many families and hence is probably politically impossible, whatever its intrinsic desirability.
Implementation issues—measuring breastfeeding rates for rewards and payments
Creating significant incentives for mothers to complete an extended breastfeeding program has multiple levels of complication. These include the fundamental issue that in order to reward people for doing something, we must have ways to ascertain whether they have actually accomplished the goal, knowing full well that if the reward is sufficiently high, people will lie and cheat to gain the reward. Thus any financial incentive program must develop a relatively foolproof, and hopefully minimally invasive, way of determining maternal compliance with a breastfeeding program. The same issues hold whether a program aims at individual mothers or group programs offering support, counseling, etc. (to the extent that they reward successful outcomes of breastfeeding rather than merely offering services). Mechanisms to achieve this lie far beyond the capabilities of economists, but we can say for sure from that discipline's perspective that inadequate measurement will doom any incentive-based program.
Although commonly used in studies of breastfeeding rates, 15 self-reports by mothers will likely be unreliable, with considerable social pressure for the mothers to give the “right” reports, and this will become greatly exacerbated if a significant financial reward is attached to a report of high compliance.
What if we had healthcare providers—pediatricians, visiting nurse services, certified lactation counselors, social workers, and the like—allowed to certify compliance with a breastfeeding program? First, of course, the same question arises as to what evidence they would use to support their report. Testimony from mothers would still be unreliable. Second, particularly for low-income families, enormous pressure would descend upon “certifiers” to aver mothers' success in order to bring cash payments to the mothers and children. The larger the financial incentive involved, the worse this problem becomes. Finally, we could expect a market response to such a system with highly advertised “lax” certifiers offering their services to a willing public. The frequency of public advertising for “medical marijuana” certification in California and elsewhere attests to the ability of the market readily and happily to provide such services.
Do biological mechanisms exist that would give an accurate cumulative measure of breastfeeding duration and frequency? In some cases, our bodies provide a neat summary measure of what has happened over recent time. With caloric intake, weight changes provide a good measure of excess caloric intake over use. With blood sugar, one can capture “snapshots” of levels using either urine or blood samples, but (conveniently) hemoglobin A1c measures summarize recent blood sugar levels well over the average life span of red blood cells (about 120 days), and the laboratory value for hemoglobin A1c has been a standard measure for diabetic control and incipient diabetes since 1976. Does such a measure exist for breastfeeding? Again, this lies beyond the scope of economic analysis, but if such measures exist, they would greatly simplify the successful administration of any individual-performance reward system or group support program.
Public opinion, movies, TV, and mass media
Laws regarding public breastfeeding
A significant deterrent to continued breastfeeding even by the most avid mother is the question of feeding in public. In our increasingly mobile society, particularly for women who work or have other activities that take them around and about in their communities often, breastfeeding in the privacy of one's own home has become an impractical option. Yet until recently, many states had laws prohibiting public breastfeeding, often characterizing it as “indecent exposure” in the same way that the infamous “wardrobe accident” of a recent Super Bowl was characterized. Although state law varies considerably from state to state, most states now specifically either authorize breastfeeding in public or specifically exempt the act from definitions of nudity, indecency, and indecent exposure. Federal law (as of the Right to Breastfeed Act of 1999) specifically protects a woman's right to breastfeed on federal property where she otherwise is permitted.
Several Members of Congress have sought inclusion of breastfeeding as a protected right under the U.S. Civil Rights Act. Such legislation would both put a powerful legal apparatus behind the protection of mothers' rights to breastfeed and would also help to alter public opinion in general.
Public attitudes and media portrayals
Any analysis of past large-scale changes in human behavior will recognize that the shift never comes fully until public attitudes change about the activity in question. Smoking did not change merely because of higher prices, warning labels, or public smoking bans. In significant part, these changes arose because public attitudes towards smoking changed. Rather than a symbol of sophistication (as had been common in Hollywood movies, books, and elsewhere), it became uncouth, particularly among those with more education. Indeed, one could argue that these changes in public attitudes supported and created the smoking ban legislation, for example. The Advertising Council has had a long and important role in creating artful and powerful advertisements about the risks of smoking (in parallel with bans on TV advertising of tobacco products) and illicit drug use.
The changes in drunk driving laws and behavior came with a similar shift in public sentiment. Many people viewed drunk driving as something more funny than dangerous, and standard movie fare was the happy drunk, weaving his way around the community, notably including “lovable drunk” characters by comedians Joe E. Lewis and Dean Martin (who also had the personalized license plate DRUNKY on his car).
Alcohol producers participate in this change currently with the “responsible drinking” campaigns now seen regularly on television ads for alcoholic beverages. These ads began in England through the Portman Group (an association of leading alcoholic beverage producers in the United Kingdom) and the Century Council in the United States, founded in 1991.
As a thought experiment, consider how society might react to the regular presence of a woman breastfeeding her infant in public on a popular TV series (the prototypical Crime Scene Investigation, Cold Case, etc., types of series, for example) as part of the character's daily life (complete with all of the joys and problems thereof). Would the public respond favorably, or threaten to boycott the sponsors? How would network executives react? Indeed, would the Federal Communications Commission allow such a role to take place regularly on daytime or prime time television? Until breastfeeding becomes “normalized” to the point that it would not be an issue with over-the-air prime time television, women will feel pressure to avoid breastfeeding in public, and hence overall participation rates will remain low.
Summary
Breastfeeding rates, while growing, remain somewhat below targets for Healthy People 2010 but lag far behind recommendations from the American Academy of Pediatrics that every baby would benefit from 6 months of exclusive breastfeeding. The costs of not achieving high breastfeeding rates are very high; recent estimates put the gains from 90% compliance with the American Academy of Pediatrics recommendation at 911 lives saved annually and over $3 billion in reduced healthcare costs annually (amounting to about $850 per birth just for the saved health costs).
Our society has seen large changes in other important health-related behaviors, including greatly reduced use of tobacco (following the Surgeon General's report in 1964), dramatic reductions in drunk driving deaths since the founding of Mothers Against Drunk Driving in 1980, and a rapidly growing rate of obesity (begining about 1975). In each case, one can find relationships between healthy behaviors and the level of educational attainment of individuals: More education produces healthier behaviors.
Specific education has an important role in these changes as well, repeated through decades of time, in many media, formats, and languages. These two types of education interact: More highly educated people in general seem to respond more to new information about health risks and gains from various behavioral choices.
Incentives and prices have important roles to play in changing people's behavior as well. In the tobacco consumption changes, large increases in tobacco taxes have not only helped shift overall consumption rates but provided funds to support anti-smoking informational ads. Lower prices for food and higher costs of time (e.g., for food preparation) have led to important shifts in the eating patterns of U.S. families, contributing in part to the obesity epidemic. The effects of this shift in eating venue have been exacerbated by the regular increase in portion size of restaurant servings of many types of food as well as in the size of prepackaged foods.
Incentives could play a larger role in promoting breastfeeding as well, with possible programs ranging from direct incentive payments to mothers to support for education, counseling, and coaching programs. Any such programs require a diversion of resources from elsewhere in our economy (e.g., taxation of health insurance premiums or general income or sales tax increases).
Finally, achieving high rates of breastfeeding initiation and high-duration feeding (preferably exclusively for the first 6 months) will require shifts in public attitudes about breastfeeding in general and public breastfeeding in particular. Sometimes such changes lead legal and other changes (arguably, Mothers Against Drunk Driving's involvement in drunk driving was the leading indicator in those changes), and sometimes information and its sequelae create the change in attitudes (as seems the case in smoking). Portrayals of these activities in movies, TV shows, and mass media can affect public attitudes and perceptions. How to bring all of this about remains the central challenge to those seeking increased breastfeeding rates in this country and around the world.
Footnotes
Disclosure Statement
No competing financial interests exist.