
Abstract
Abstract
Objective:
Maternal obesity has been associated with lower initiation of breastfeeding, but reasons for why this association exists have not been well studied. In this study, we examined associations among prepregnancy obesity, psychological factors during pregnancy, and breastfeeding initiation.
Methods:
Data came from the postpartum component of the Pregnancy, Infection, and Nutrition study, a prospective cohort study. Pregnant women were recruited from the University of North Carolina hospitals between January 2001 and June 2005. This analysis used data from 688 women followed from pregnancy to 3 months postpartum. Multivariable binomial regression was used to determine the association between having a body mass index (BMI) >26 kg/m2 before pregnancy and breastfeeding initiation. We tested for mediation of the association between pregravid BMI and breastfeeding initiation by certain psychological factors during pregnancy (depressive symptoms, perceived stress, anxiety, and self-esteem).
Results:
Women who began pregnancy overweight or obese (BMI >26 kg/m2) had almost four times the risk of not initiating breastfeeding compared with underweight or normal weight women (BMI ≤26 kg/m2) (risk ratio = 3.94 [95% confidence interval 2.17, 7.18]) after adjusting for race, poverty level, education level, and marital status. Depressive symptoms, perceived stress, anxiety, and self-esteem levels during pregnancy were not found to mediate the association between pregravid BMI and breastfeeding initiation.
Conclusions:
Women who started pregnancy either overweight or obese were more likely to not initiate breastfeeding. Contrary to expectations, pregnancy-related psychological factors did not influence this relationship.
Introduction
Few have researched a potential mediatory pathway between pregravid BMI and breastfeeding initiation by psychological factors. Prior research shows that maternal obesity is associated with women's psychological status during the perinatal period (pathway “a” in Fig. 1),10,11 but there is less epidemiologic evidence relating psychological status to breastfeeding initiation (pathway “b” in Fig. 1). We focus on four factors that may be indicative of women's overall mental health status during pregnancy: depressive symptoms, stress, anxiety, and self-esteem. Studies examining the association between prenatal depressive symptoms and breastfeeding initiation have found conflicting results, and the use of different measurement scales makes it difficult to compare these results across studies.12–14 One study that examined anxiety during pregnancy found no relationship to breastfeeding initiation, although higher levels were related to a lower intent to breastfeed, which is known to predict initiation.14–16 To our knowledge, the effects of prenatal perceived stress and self-esteem on breastfeeding initiation have not previously been studied.
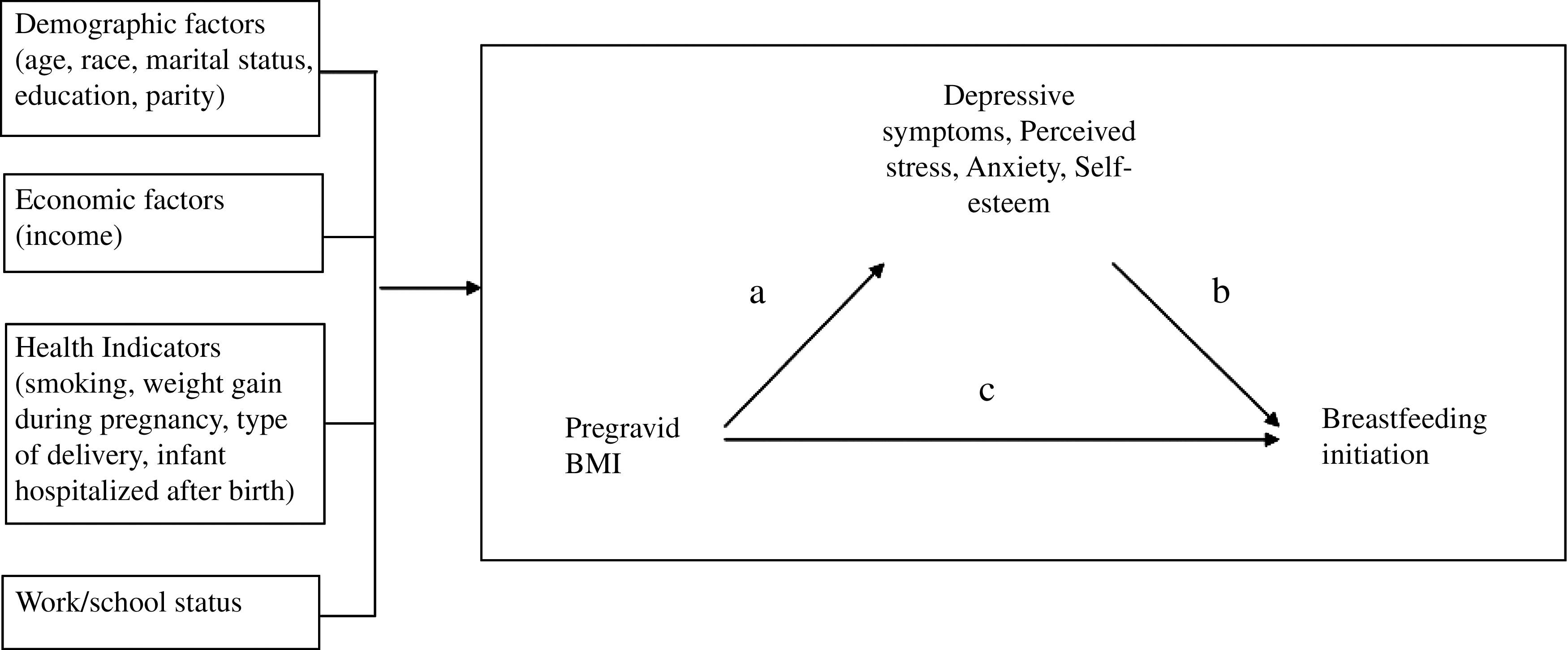
Relationship among pregravid body mass index (BMI), psychological factors, and covariates.
In this article, we present findings on the associations between pregravid BMI, psychological factors (prenatal depressive symptoms, stress, anxiety, self-esteem), and breastfeeding initiation. We hypothesize that women who are overweight or obese before pregnancy are less likely to initiate breastfeeding. Furthermore, we expect that part of the association between pregravid BMI and breastfeeding initiation is mediated by the presence of higher levels of depressive symptoms, stress, and anxiety and lower levels of self-esteem among overweight and obese women during pregnancy. Levels of these psychological factors during pregnancy may be indicative of a woman's overall mental health status during the prenatal period and are modifiable risk factors for future breastfeeding interventions.
Subjects and Methods
Subjects
Data came from the postpartum component of the Pregnancy, Infection, and Nutrition (PIN) study, a prospective cohort study focusing on weight gain, psychosocial factors, physical activity, diet, and health behaviors during and following pregnancy. 17 Women between 15 to 20 weeks' gestation were recruited at their second prenatal clinic visit at University of North Carolina hospitals between January 2001 and June 2005. Women younger than 16 years of age, non–English-speaking, ≥20 weeks' gestation on their second prenatal visit, and not planning to continue care or deliver at the study site and those carrying multiple gestations were not eligible to participate. Of the 2,006 women who were followed up through pregnancy, 1,169 (58.3%) were eligible for the postpartum component (PINPost) of the study. To be eligible, they must have delivered live-born infants between October 2002 and December 2005 and have lived within a 2-hour radius of the University of North Carolina (in order to facilitate home visits). We excluded 239 women: 24 due to medical constraints, 153 were unreachable, 54 were more than 5 months postpartum by the time they were contacted, and eight for whom study protocols were not in place at the time of their eligibility window. The remaining 930 (79.6% of 1,169) women were phoned at 6 weeks postpartum with a description of the postpartum component; 688 (58.9% of 1,169) women consented and were interviewed in their homes by trained staff at approximately 3 months postpartum. Protocols for this study were approved by the University of North Carolina School of Medicine Institutional Review Board.
Outcome
The dependent variable, breastfeeding initiation, was assessed at 3 months postpartum by the question “Did you ever breastfeed this baby?”
Exposure
Pregravid BMI was calculated from self-reported weight (checked for implausible values) and measured height, collected during screening between 15 to 20 weeks' gestation. For our analysis, pregravid BMI was dichotomized at 26 kg/m2 based on the Institute of Medicine's cutpoints in use at the time participants attended prenatal care. 18 Women >26 kg/m2 before pregnancy were identified as overweight or obese, and those ≤26 kg/m2 were designated as being of normal or underweight BMI (the referent category).
Psychological variables
Depressive symptoms during pregnancy were assessed using the Center for Epidemiologic Studies-Depression scale (CES-D). 19 Participants were given questionnaires to return by mail at the first and second prenatal visits; 640 (93% of 688) completed the CES-D component of the questionnaire given between 15 to 20 weeks' gestation, and 598 (87% of 688) completed the CES-D given between 24 to 29 weeks' gestation. The 20-item scale had Likert response categories that assessed the participant's feelings and activities in the previous week. A composite score was calculated and dichotomized at 17 for both time points measured; scores ≥17 indicated the presence of a higher level of depressive symptoms. Although a cutpoint of 16 or higher is generally used to represent higher depressive symptoms, we used a slightly higher score to better distinguish between depressive and pregnancy symptoms, which are often similar. 20 We compared our use of a higher cutpoint with a method proposed by Hoffman and Hatch 21 where items that overlap with pregnancy are removed and scores rescaled so that a cutpoint of 16 can be used. Both methods produced highly correlated scores, and the majority of women were categorized into the same depressive symptoms category (p < 0.0001). Internal consistency as indicated by Cronbach's α ranged from 0.83 to 0.92. 22
The Perceived Stress Scale 23 measured the degree to which respondents found situations to be stressful. Six hundred eighty-seven women completed the 14-item scale administered over the phone at 17–22 gestational weeks, and 652 (94.8%) completed a modified 10-item scale during a phone interview conducted between 27 and 30 gestational weeks. Questions were on a Likert scale, and higher overall scores indicated higher levels of perceived stress. After summing across items for each time period, the variables were categorized into three levels: 0 to <17 (low stress; referent), 17 to <23 (moderate), and ≥23 (high) for the 14-item scale versus 0 to <11 (low stress; referent), 11 to <17 (moderate), and ≥17 (high) for the 10-item scale. Cronbach's α was 0.83 in three nonpregnant samples tested by Cohen et al. 24
The State-Trait Anxiety Inventory was used to assess state and trait anxiety during pregnancy. 25 For this analysis, we used the state anxiety measurement because it assessed “immediate” feelings of anxiety, which better represented how women felt during pregnancy than the trait-anxiety scale, a stable measure of anxiety. The state-anxiety scale had 20 questions on a 4-point Likert scale. Six hundred thirty-six (92.4%) participants completed the mail-in questionnaire given at screening (15–20 weeks), whereas 593 (86.2%) completed the questionnaire provided at the second prenatal visit (24–29 weeks). The variables were categorized into three levels: 0 to <29 (low anxiety; referent), 29 to <39 (moderate), and ≥39 (high). Cronbach's α ranged from 0.90 to 0.94 for the state scale. 25
The Self-esteem Scale 26 was completed by 635 women (92.3%) during a phone interview between 15 and 20 gestational weeks. This variable was measured only once because we did not believe self-esteem was likely to change considerably during the course of the pregnancy. Ten questions on a 6-point Likert scale were used to determine the respondent's sense of self-worth and positive or negative orientation towards oneself. The variables were categorized into three levels that indicated low, moderate, and high self-esteem: 0 to <50, 50 to <56, and ≥56 (referent), respectively. Test–retest correlations have been shown to be in the 0.82–0.88 range, and Cronbach's α ranged from 0.77 to 0.88. 27
Both measurements for the CES-D, perceived stress, and state anxiety were separately assessed as mediators to determine which time point had a greater effect on the pregravid BMI–breastfeeding initiation relationship.
Covariates
We collected data on several covariates through self-reported questionnaires, telephone interviews, and medical chart abstraction. The covariates reported here were examined for effect measure modification and confounding. They were selected based on construction of a directed acyclic graph, created after a review of the literature, that depicted the relationships among the exposure (pregravid BMI), outcome (breastfeeding initiation), and covariates. 28 Participants reported their race, age, parity, education, marital status, family income, household size, smoking status in the first two trimesters, and work/school status following the birth of the baby. Information on family income and household size was used to create a variable representing percentage of the 2001 poverty index according to the U.S. Bureau of the Census. 29 We also collected information on weight gain during pregnancy, preterm birth, type of delivery (vaginal or cesarean), and whether the infant was hospitalized following delivery.
Statistical methods
Descriptive statistics were generated for the variables of interest. Student's t test and χ2 tests were used to examine associations between study variables and breastfeeding initiation. Variables were assessed as both effect measure modifiers and confounders. Modification was tested using a likelihood ratio test to compare models with and without an interaction term between the potential modifier and pregravid BMI (a priori significance criterion of p < 0.15). If variables failed to meet the criteria for modification, they were tested for confounding. Covariates were kept as confounders in the final model if they changed the β coefficient of the exposure by >10%. Binomial regression produced risk ratio (RR) values of the association between pregravid BMI and breastfeeding initiation.
Mediation was tested using a series of regression analyses. 30 To be considered a mediator, the exposure must be associated with the outcome (pathway “c” in Fig. 1; Model 1), the mediator must be predicted by the exposure (pathway “a” in Fig. 1; Model 2), the outcome must be predicted by the mediator while adjusting for the exposure (pathway “b” in Fig. 1; Model 4), and the effect estimate of the exposure must be reduced while adjusting for the mediator (Model 4). An additional step (Model 3) was added to explore the association between the psychological factors and breastfeeding initiation. The Sobel test for mediation determined whether the indirect effect of the exposure on outcome via the mediator was significantly different from zero. 31 Each psychological factor was tested in separate mediation analyses. All statistical analyses were conducted using Stata software (version 9.2; Stata Corp., College Station, TX).
Results
The cohort was composed primarily of women who were white (76.5%), married (80.4%), an average of 29 years old, had a college degree (65.5%), and were living above the poverty line (61.1%) (Table 1). Most women had a BMI of ≤26 kg/m2 before pregnancy (68.1%) and gained above Institute of Medicine–recommended weight gain guidelines during pregnancy (63.7%). Compared with women who started pregnancy underweight or normal weight, women who started their pregnancy overweight or obese were more likely to be non-white, less educated, unmarried, living below the poverty line, multiparous, and have gained weight excessively during pregnancy. Of the women who did not breastfeed, most were overweight or obese before pregnancy (72.1%) and multiparous (72.6%) and did not have a college degree (78.7%), and nearly half lived below the poverty line (47.5%).
By Pearson's χ2 test, p < 0.05 unless otherwise stated.
By Student's t test, p < 0.01.
Mean scores for depressive symptoms at 15–20 weeks and perceived stress at 17–22 weeks were significantly higher for those who did not breastfeed compared with those who breastfed (p < 0.05; Table 2). Compared with breastfeeders, non-breastfeeders had a greater proportion of women in the higher depressive symptoms category at 15–20 weeks but not at 24–29 weeks of gestation (p < 0.01); however, there was no difference in stress, anxiety, or self-esteem levels between breastfeeders and non-breastfeeders at either assessment point. Those with a BMI >26 kg/m2 prior to pregnancy had lower levels of self-esteem and higher levels of depressive symptoms, stress, and anxiety at both measurement times than those ≤26 kg/m2 before pregnancy.
Not all of the 688 women who completed the 3-month interview completed the assessments for depressive symptoms, stress, anxiety, and self-esteem during pregnancy.
Mean ± SD values (% of overall n).
Student's t test p value conducted to compare means of those who breastfed versus did not breastfeed and those with BMI ≤26 kg/m2 versus BMI >26 kg/m2 (all such values).
Pearson's χ2 test p value comparing proportions between those who breastfed versus did not breastfeed and those with BMI ≤26 kg/m2 versus BMI >26 kg/m2 (all such values).
The majority of women who completed both CES-D assessments at 15–20 and 24–29 weeks of gestation (n = 581) remained at a low level of depressive symptoms (72.1%); 9.3% increased to high levels, and 6.2% decreased from high to low levels. Of the 652 women who completed both perceived stress measurements, 17.8% increased to a higher stress level during pregnancy, wheres a quarter of women (24.8%) remained at a low level of stress. Almost one-third (31.2%) of women who completed both anxiety measurements (n = 573) decreased to lower levels of anxiety as pregnancy progressed, whereas 14.8% increased. A greater proportion of non-white participants reported higher levels of depressive symptoms, stress, and anxiety at both measurements during pregnancy (p < 0.05). Proportions of high and low self-esteem were not different between white and non-white participants.
Crude RR estimates showed a strong association between being overweight or obese before pregnancy and not breastfeeding (RR = 5.52 [95% confidence interval 3.23, 9.45]). This association was modified by age such that as age increased, women entering pregnancy overweight or obese were less likely to breastfeed than those of normal weight or underweight before pregnancy. After confounders were included in the model, however, age was no longer a significant effect measure modifier. The crude association between pregravid BMI and breastfeeding was attenuated but remained strong after adjusting for race, education, marital status, and poverty status; women who started pregnancy overweight or obese were much more likely to not initiate breastfeeding compared with women of lower BMI (RR = 3.94 [95% confidence interval 2.17, 7.18]).
We then tested the hypothesis that the pathway between pregravid BMI and breastfeeding initiation was partially mediated by depressive symptoms, stress, anxiety, and self-esteem. Results from crude regression analyses are shown in Table 3, categorized by psychological factor. Model 1, the crude association between pregravid BMI and breastfeeding initiation, is the same for each psychological factor and is noted as a footnote in Table 3. Perceived stress and state anxiety were not related to breastfeeding initiation at either of the measured time points and therefore did not fit the definition of a mediator variable. 30 Self-esteem and depressive symptoms at 15–20 weeks (but not 24–29 weeks) were significantly related to both pregravid BMI and breastfeeding initiation (Models 2 and 3). In Model 4, depressive symptoms at 15–20 weeks slightly reduced the effect of pregravid BMI on breastfeeding initiation (8% change in estimate) and was considered to be a weak mediator in crude analyses. Self-esteem increased the magnitude of the relationship between the exposure on outcome, possibly acting as a suppressor variable as explained by McKinnon et al. 32 However, the Sobel test found no significant reduction in the effect of the pregravid BMI on breastfeeding initiation via any of the hypothesized mediators (data not shown). In addition, once we accounted for race, education, marital status, and poverty status, pregravid BMI no longer predicted the psychological factors. Furthermore, depressive symptoms and self-esteem were not associated with breastfeeding initiation in the adjusted models.
The sample size was restricted to those women who completed all the above-listed questionnaires and for whom we had information on pregravid BMI (n = 546).
Restricting the sample size to 546 resulted in a crude risk ratio (RR) of 5.98 (95% confidence interval 3.14, 11.38) for the association between pregravid BMI and breastfeeding initiation; this was considered Model 1.
Models 3 and 4 used binomial regression analysis to determine RR values unless otherwise stated; breastfeeding initiation was the dependent variable (not initiating breastfeeding was the index category).
Linear regression analysis was used because the mediator was continuous.
Discussion
Our analysis provides support for an adverse association between pregravid BMI and breastfeeding initiation; similar to previous studies,4–7 we found that women who entered pregnancy overweight or obese were much more likely to not breastfeed compared with normal or underweight women. We further explored whether this association could be explained in part by psychological factors present during pregnancy. Although we did not find evidence of mediation by depressive symptoms, stress, anxiety, and self-esteem during pregnancy, our analysis contributes to the growing body of literature aiming to understand why overweight and obese women are less likely to breastfeed.
There are several possible reasons why we did not find evidence of mediation by the psychological factors. Of the psychological variables tested, only depressive symptoms at 15–20 weeks of gestation and self-esteem predicted the outcome, breastfeeding initiation. The lack of association may be a consequence of the recruitment pool. Of the 1,169 women who were eligible to participate in the postpartum component, 480 were excluded or refused. We compared these 480 women with the 688 who attended the 3-month visit and found that those who refused to participate or were excluded had significantly higher levels of depressive symptoms and anxiety (data not shown). There was no difference in self-esteem or stress between the two groups. Thus, it is possible that we did not see a mediating effect of psychological factors on the pregravid BMI–breastfeeding initiation relationship because the women who chose to participate in PINPost had better overall mental health status during pregnancy than those who were excluded or refused, reducing the likelihood of finding an association. In addition, our measurement tools could not clinically diagnose depression or anxiety. It may be that a more sensitive measurement tool is needed before we can see an effect on breastfeeding initiation. It is also possible that other factors more strongly influence the relationship between maternal overweight/obesity and breastfeeding initiation than psychological factors. For example, biological effects of overweight/obesity, such as increased risk of pregnancy complications and adverse birth outcomes, may be more important in explaining why overweight or obese women are less likely to breastfeed. 8
Although we found that depressive symptoms, perceived stress, anxiety, and self-esteem did not mediate the association between pregravid BMI and initiation of breastfeeding, it was important to explore their role given their potential as targets in breastfeeding interventions. Moreover, this is one of a few studies to examine how psychological factors in pregnancy can influence breastfeeding initiation. Previous studies have focused primarily on the postpartum period and the relationship between psychological factors and breastfeeding duration, excluding women who chose not to breastfeed. However, we wanted to look specifically at the effect of pregravid BMI on breastfeeders versus non-breastfeeders. Our results provide further support for the findings by Fairlie et al. 14 that perinatal anxiety levels are not associated with breastfeeding initiation. We did find that higher levels of depressive symptoms between 15 and 20 weeks of gestation significantly increased the risk of not breastfeeding, but this association attenuated and became nonsignificant after adjusting for confounders. To our knowledge, this is the first quantitative study to examine the effects of stress and self-esteem on breastfeeding initiation.
A further strength of this study includes its prospective cohort study design. This enabled measurement of the exposure and mediators prior to the outcome and thus allowed for the assessment of risk. In addition, previous work has failed to examine as many potential modifiers and confounders as comprehensively as we were able to do in the PINPost study.
While the PINPost study has been able to examine numerous risk factors related to maternal and child health status, the generalizability of the findings are limited by the fact that most women were Caucasian, of a higher socioeconomic status, and received prenatal care during pregnancy. Our population is different from the general population of women who give birth in that 91% initiated breastfeeding, which is much higher than the national average of 73.8%. 3 We also have a much lower prevalence of overweight/obese women (31.9%) compared with the average for women of childbearing age in the United States (59.5%). 33 Furthermore, we did not have sufficient power to analyze racial or ethnic differences, although African American women in the United States have higher rates of obesity and lower rates of breastfeeding initiation than white women.3,34,35
An additional limitation of this analysis is in the assessment of the outcome variable. At the 3-month interview, breastfeeding initiation was determined by asking women, “Did you ever breastfeed this baby?,” and it is possible that participants varied in their interpretation of the question. However, we found similar results when we compared our current definition of breastfeeding initiation with that of initiation defined as breastfeeding for 1 week or longer. This suggests that we are capturing women who persevered with breastfeeding rather than women who made a brief attempt to breastfeed.
In this article, we found that prepregnancy obesity negatively influenced breastfeeding initiation and that higher levels of depressive symptoms, stress, and anxiety and lower levels of self-esteem did not alter this adverse association. Studies examining the role of psychological factors should explore the possible mediating role of clinically diagnosed depression and anxiety. It may be that clinical levels of depressive symptoms and anxiety, not diagnosed by the CES-D or the State-Trait Anxiety Inventory, may be associated with breastfeeding. Furthermore, a dataset with a larger sample size and thus greater statistical power than ours can provide the ability to examine differential effects by race. Future studies should also explore other reasons why women who enter pregnancy overweight or obese are less likely to breastfeed. Given the prevalence of prepregancy obesity and the health benefits of breastfeeding, it is critical to elucidate the pathways between the two. As we advance our understanding of infant feeding decisions, we can better target interventions for improving breastfeeding initiation rates.
Footnotes
Acknowledgments
U.J.M. was responsible for the analysis and writing of the manuscript. A.M.S.-R. was the principal investigator and guided the statistical analysis and writing of the article. A.H.H. was a co-investigator of the study and provided guidance for the statistical analysis. A.H.H., L.S.A., and M.E.B. provided significant advice in the writing of the manuscript. We would like to thank all of the Pregnancy, Infection, and Nutrition Postpartum investigators: Nancy Dole, Kelly Evenson, David Savitz, June Stevens, and John Thorp for obtaining funding and designing the study. Additionally, we would like to thank Kathryn Carrier for managing the PIN study. This study received support from the National Institutes of Health (the National Institute of Child Health and Human Development [grants HD37584 and HD39373] and the National Institute of Diabetes and Digestive and Kidney Diseases [grants DK61981 and DK56350]) and the Carolina Population Center.
Disclosure Statement
No competing financial interests exist.