
Abstract
Abstract
Background:
Numerous studies have documented short- and long-term differences in growth and body composition based on whether an infant is breastfed or formula-fed. However, little is known about whether these differences result from the substance consumed (breastmilk vs. formula) or from the delivery method (breast vs. bottle). This prospective pilot study compared the growth and body composition patterns of 19 predominantly breastfed/nursing infants (NG) and 18 infants fed significant quantities of breastmilk by bottle (BG) during the first 6 months of life.
Methods:
Infants were measured in a laboratory setting each month by trained staff. Growth measures (length, weight, and head circumference) were compared to World Health Organization growth standards. Body composition, including relative fat mass (%FM), was measured using an air-displacement plethysmography system (Pea Pod®, Life Measurement, Inc., Concord, CA).
Results:
With the exception of small differences in length and weight scaled for length (body mass index and weight-for-length z-score) present at birth and continuing for the first 1–2 months of life, NG and BG infants were similar in weight, weight-for-age z-scores, head circumference, fat mass, and %FM. However, BG infants were three times more likely to exceed the 85th percentile for weight velocity during the 4–6-month age interval than NG infants (33% vs. 10%, respectively), but this did not reach statistical significance in this sample size (p = 0.12).
Conclusions:
This pilot study suggests the delivery method (breast vs. bottle) for breastmilk may not dramatically affect growth for the first 4 months of life; however, future research with larger samples will be needed to carefully evaluate longer-term growth patterns in infants fed breastmilk by bottle.
Introduction
Another major problem with dichotomizing feeding mode is that it fails to account for the independent effects of what (breast milk, formula) is fed from how (breast, bottle) the substance is delivered. 8 The protective effects of breastfeeding may be attributable to substances in the breastmilk, such as leptin and insulin-like growth factor, that are absent, biologically active, or in lower levels in formula.9,10 A second possibility is that the nature of breastfeeding, where parents have less capability to encourage overconsumption of milk, is responsible for this protective effect. 8 Thus, research aimed at understanding whether and how breastfeeding may protect against later obesity should clearly separate out the effects of the substance consumed from the delivery method. With this information, researchers and clinicians could design more effective intervention strategies for the early years of life.
One way to learn more about the risk associated with the delivery method (breast, bottle) is to carefully study the early growth and caloric intake patterns of infants fed significant quantities of breastmilk by bottle compared with breastfed infants. This study design provides a relatively consistent effect of the substance being consumed (breastmilk) while varying the method of delivering the milk (breast, bottle). This study design was used to compare the anthropometric and compositional growth of infants fed a significant proportion of breastmilk by bottle to infants fed breastmilk by breast during the first 6 months of life. Based on what is known about caregiver-led bottle-feeding behaviors in formula-fed infants,11–13 we hypothesized that infants fed breastmilk by bottle would demonstrate more rapid growth (weight-for-age, weight-for-length, body mass index [BMI], and their z-scores) and body fat deposition (relative body fatness [%FM]) compared with infants who were predominantly nursed.
Subjects and Methods
Study design
These data are part of an ongoing prospective longitudinal study designed to assess how early feeding experiences affect growth and body composition during the first 2 years of life. Mother–infant dyads were recruited from Centre County, PA prior to the infant turning 1 month old. Mothers were recruited from the local hospital's maternity unit as well as daycare centers and businesses providing child-oriented products and services. Mother–baby dyads were screened for eligibility based on general inclusion and exclusion criteria and then were considered against stricter inclusion and exclusion criteria for membership into either the nursing group (NG) or bottle-feeding breastmilk (BG) group. For inclusion, mothers must have been ≥18 years old at study entry and delivered a singleton pregnancy. Exclusion criteria included health problems or conditions that could interfere with breastmilk production (e.g., post-delivery hemorrhage), failure to provide breastmilk for 6 months postpartum in any previous pregnancies, intention to provide more than one bottle of formula per day during the first 6 months post-delivery, and presence of health problems that could interfere with completion of study activities. For inclusion in NG, mothers must have intended to limit bottle feeding to one bottle per day of breastmilk and/or formula. For inclusion in BG, mothers must have planned to return to work full-time by 6 weeks postpartum (or provide pumped milk for a similar amount of time per week). Only healthy, term (>36 weeks in gestational age) infants with a birth weight exceeding 2,500 g were included. Infants were excluded if they had any medical conditions that affected growth, development, or parental feeding practices. For infants in daycare, only those in a stable, consistent feeding environment were included. Specifically, this meant the baby must have been assigned to a consistent staff member (not rotate care providers each day) and the daycare manager must have felt confident the infant's care provider would remain at the facility during the 6-month study. For the data presented here, the initial subject pool included 24 NG mother–infant dyads and 26 BG mother–infant dyads. All study procedures were approved by the The Pennsylvania State University's Institutional Review Board, and all mothers provided active consent prior to study entry.
BG mothers were provided with commercial breast pumps (Avent™ ISIS IQ Duo [Royal Philips Electronics, Eindhoven, The Netherlands] or Medela Pump In Style® [Medela AG, Zug, Switzerland]), feeding bottles, and bottle nipples for use during the 6-month study. All items were commercially available products. Various bottle sizes were provided, and mothers were required to use the provided bottles during the 6-month study. The manufacturer's slow flow nipples were given to the mothers, and they were required to use them during the study to reduce the chances that bottle feeding would interfere with breastfeeding success. All mothers had access to a lactation consultant to address problems with breastfeeding and/or pumping.
Protocol
Mothers and infants reported to the laboratory each month for assessment of growth, body composition, and feeding mode from month 1 to month 6 post-delivery. In several cases, fathers attended the visits to help answer questions about infant feeding, particularly if they were the primary caregiver during the mother's work hours. Visits were scheduled within 1 week of the infant's monthly “birthday.” Parents were asked a series of questions to assess feeding mode during the previous month and additional questions to screen for health problems that might impact growth (e.g., dehydration, blood in stool, intolerance to formula or breastmilk, etc.). All questions were asked in the English language as at least one parent in all families was fluent in English (study eligibility requirement).
Assessment of feeding mode
At each monthly visit mothers, and in some cases fathers, were asked to estimate the percentage of milk consumed during the past month that was breastmilk (as opposed to formula) and the percentage of breastmilk consumed at the breast (as opposed to by bottle). When estimating these values, parents were prompted to consider changes in feeding mode that occur on weekdays versus weekends and changes that had occurred across the month. Information on timing of solid food introduction was collected, but is not included in the analyses.
Growth
Birth weight, length, and head circumference data were reported by mothers, as measured by the hospital staff. All subsequent growth measurements were made by a total of three trained staff. The primary measurer (C.J.B.) collected all head circumference measurements and assisted with all length measurements. Growth measurement procedures were based on recommendations by the Maternal and Child Bureau of the Health Resources and Services Administration. 14 Nude weight (mass) was measured to the nearest gram in duplicate using a high-precision baby scale (Baby Weigh Scale, Medela Inc., McHenry, IL). Nude recumbent length was measured to the nearest 1 mm in duplicate using a calibrated infant length measuring board (Seca 416 Infantometer, Seca Corp., Hamburg, Germany). One staff member held the baby's head in contact with the headpiece in the Frankfort horizontal plane. The other staff member aligned the infant's trunk and legs, extended both legs (when possible), and brought the foot piece firmly against the heels. Head circumference was measured in duplicate using a Teflon® (Dupont, Wilmington, DE)-coated non-stretchable head circumference measuring band (Seca 212 Measuring Tape, Seca Corp.).
Body composition
We used an air-displacement plethysmography device (Pea Pod®, Life Measurement, Inc., Concord, CA) to measure infant body composition at 1, 3, and 6 months of life. This device directly measures infant mass and volume and then calculates density (mass/volume). The device's software predicts absolute fat mass (FM) and %FM and absolute and relative fat-free mass (FFM and %FFM, respectively) from density based on previous detailed studies of infant body composition. Several research studies have demonstrated the safety and accuracy of this technique.15,16 While this device is Food and Drug Administration–approved for use in infants from 1 to 8 kg, we have received an Institutional Review Board exception for use of the Pea Pod in infants up to 10 kg, allowing us to capture body composition data on all infants during the first 6 months of life.
Statistics
Demographic data are reported as mean ± SD values or as percentages, where appropriate. Differences between NG and BG demographic and birth data were assessed using t tests for continuous variables and either χ2 tests or Fisher's exact test based on the cell size for categorical variables. SAS version 9.1 (SAS Institute, Inc., Cary, NC) was used for statistical analysis of the data.
Anthropometric data were entered into the World Health Organization (WHO) Anthro program for analyses and calculation of age- and sex-specific z-scores (www.who.int/childgrowth/software/en/). Growth and body composition data were compared between NG and BG groups across all 6 months using the SAS Proc Mixed procedure with a random coefficients model. This method of analyzing longitudinal data allows data to exhibit correlation and non-constant variance. We tested both linear and quadratic models and found that all growth and body composition data fit a quadratic model. Thus, quadratic model analyses are presented. Infant sex was added as cofactor in the analyses given the known sex-specific growth differences in infants. Covariates typically added to these models, including maternal prepregnancy BMI, maternal gestational weight gain, gestational age at birth, and birth weight, were considered. They were not found to be significantly related to the outcome variables and are not included in the final statistical model.
As previous data show that the divergence in growth between formula-fed and breastfed infants occurs in the 4–6-month range, 17 the recently published WHO growth velocity standards 18 were used to examine whether NG or BG infants were more likely to experience accelerated weight gain during the 4–6-month interval. Accelerated weight gain was defined as exceeding the 85th percentile for sex-specific weight gain during the 2-month interval between the 4- and 6-month visits. χ2 analysis was used to test for differences in the percentage of infants in NG and BG experiencing accelerated weight gain.
Results
Participants
Of the 24 NG mother–infant dyads recruited for the study, five dyads were removed when the final sample was constructed. One dyad dropped out because of difficulties completing study procedures, and another was unable to complete visits when detained outside the country. Study personnel removed three dyads from the pool: two for exceeding bottle/formula intake limits and one for infant growth failure due to maternal milk insufficiency. Of the 26 BG mother–infant dyads recruited for the study, eight dyads were removed when the final sample was constructed: Six were removed for exceeding formula intake limits, one was removed for noncompliance with study procedures, and one was removed for infant growth failure due to severe gastroesophageal reflux disease. The characteristics of mothers and infants that make up the final sample are shown in Table 1. Of the demographic and baseline variables examined, only maternal employment status varied between BG and NG groups, with BG mothers more likely to be engaged in full-time employment and NG mothers more likely to be unemployed (p = 0.002).
BG, bottle-fed breastmilk group; BMI, body mass index; NG, nursing group.
Feeding mode
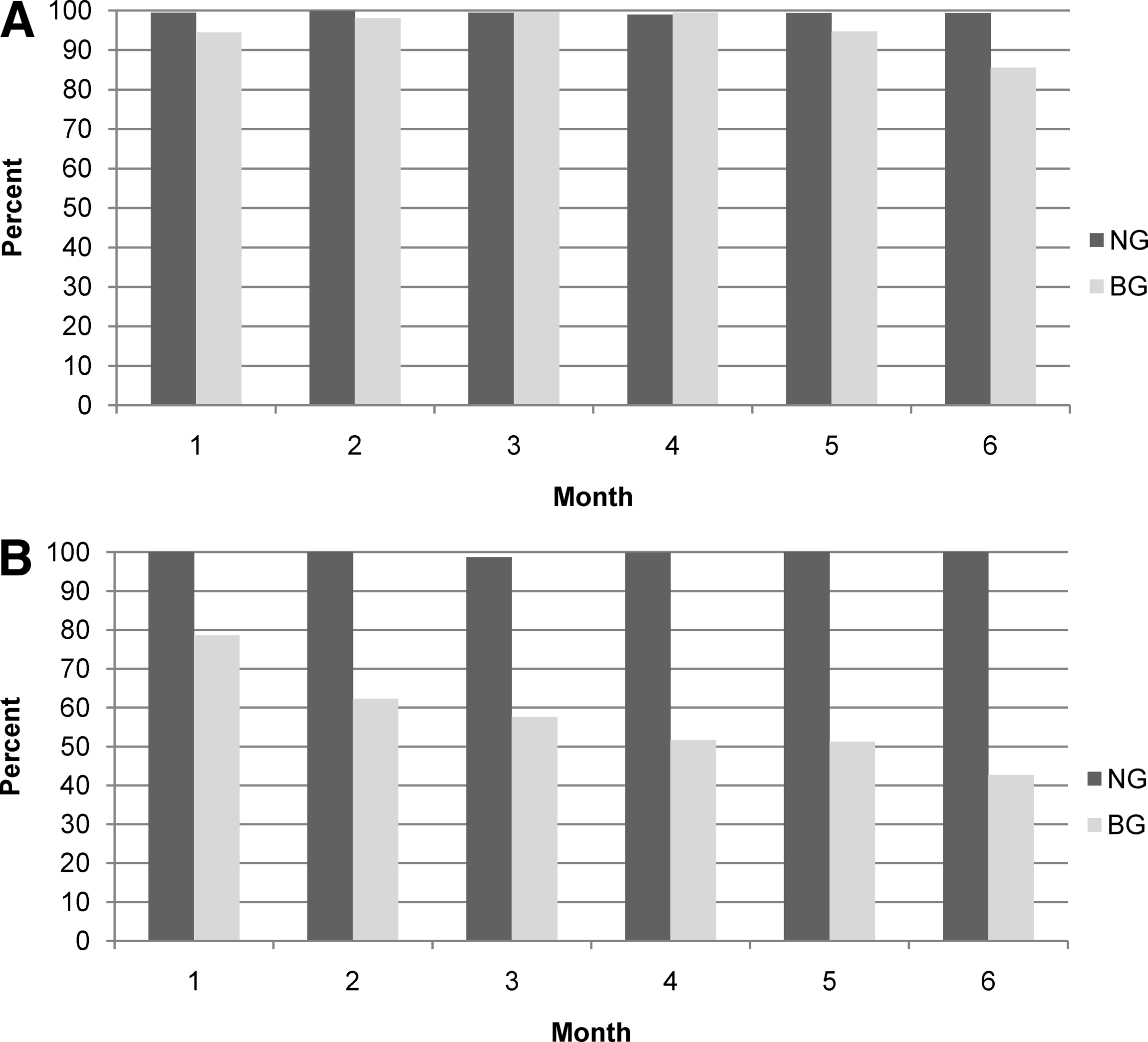
Figure 1 compares the relative amounts of breastmilk versus breastmilk substitute provided (Fig. 1A) and the relative amount of breastmilk delivered by breastfeeding versus bottlefeeding (Fig. 1B) for the two groups. As a group, nearly all the milk that NG infants received during the 6-month study was breastmilk, with more than 98% delivered at the breast. Of the milk that BG infants received, about 95% was breastmilk in months 1–5, dropping to 85% at month 6. In contrast to NG infants, the BG infants received a significant proportion of breastmilk by bottle, from 22% at month 1 to almost 60% by month 6.
Parental report of (
Growth and body composition
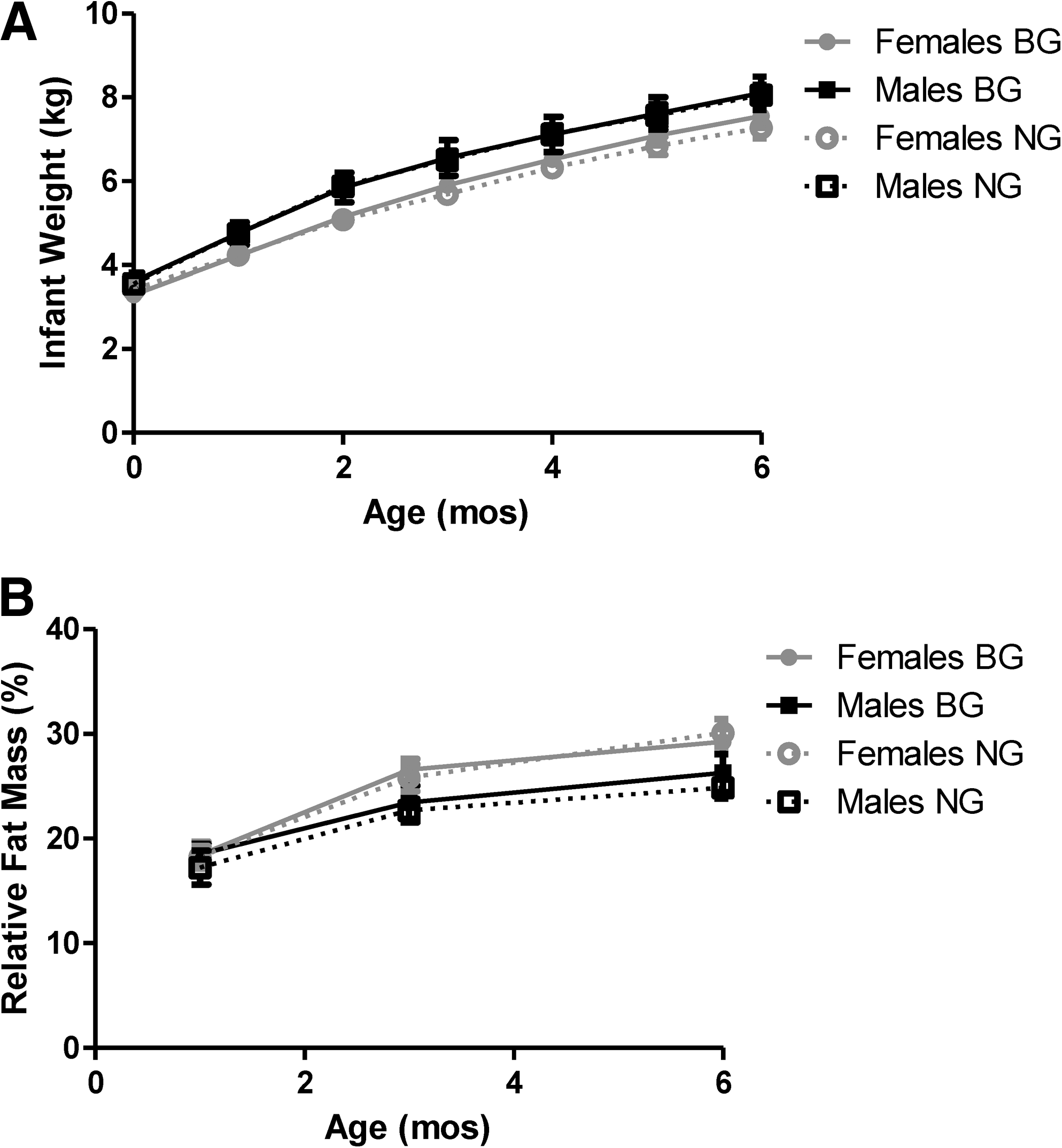
Nearly all infants displayed the expected patterns of steady weight and fat gains during the 6-month study. Figure 2 shows the average growth lines for male and female BG and NG infant groups. Figure 3 shows other growth and body composition variables for NG and BG infant groups as predicted by the quadratic mixed model analyses. These quadratic mixed model analyses were used to test whether there were growth differences between NG and BG groups across the 6-month study. NG infants were significantly longer than BG infants at month 1 (p = 0.01), leading to statistically higher values for length-for-age z-scores at 1 month (p = 0.03) and statistically lower weight-for-length z-scores at months 1 (p = 0.006) and 2 (p = 0.01) and BMI-for-age z-scores at month 1 (p = 0.03) compared with BG infants. No significant differences were observed between NG and BG groups at any age for the following variables: weight, weight-for-age z-score, head circumference-for-age z-score, FM (in kg), %FM, and FFM (in kg). Using the predicted average differences between groups as the effect size, a power value of 0.8, an α = 0.05, and the variance and within-subject variation calculated in each repeated-measures analysis of variance, a post hoc reverse power calculation was completed. The estimated sample sizes needed to detect a significant difference for variables such as weight, weight-for-age z-score, FM, and %FM is approximately 100–200 infants per group.
(

(
In comparison to the WHO weight gain velocity curves approximately 10% of NG infants and 33% of BG infants exceeded the sex-specific 85th percentile weight gain velocity for the 4–6-month age interval. This difference did not reach statistical significance in this sample (p = 0.12). A post hoc power analysis of this data, using a power value of 0.90 and an α = 0.05, showed that approximately 75 infants would be needed in each group (total n = 150) for this difference to become statistically significant. The proportions of NG and BG infants exceeding the 85th percentile weight gain velocity for the 0–2- and 2–4-month intervals were minimal and equivalent between groups (p = 1.00 for both intervals).
Discussion
Researchers continue to debate the role of early life feeding practices in the prevention of obesity later in life. 19 A substantial source of this debate originates from the various study designs used in the area. 20 Most studies to date have been largely epidemiological studies assessing the statistical relationship between breastfeeding and obesity later in life. Despite efforts to statistically minimize the effects of confounding demographic and lifestyle factors (e.g., Owen et al. 3 ), ultimately we cannot rule out alternative explanations when utilizing this research design. Other researchers have studied sibling pairs, who presumably experience many of the same confounding factors but have been breastfed for different lengths of time.21,22 Another large study randomized mothers to a breastfeeding promotion intervention. 23 While some research designs are better suited to answer the questions of whether and how breastfeeding provides protection against later obesity, all designs suffer from one or more significant weaknesses. 8 Without a way to ethically randomize mother–baby dyads to feeding condition, researchers have continued to search for unique and novel ways to minimize confounding effects, accurately capture the exposure of interest (breastfeeding, formula, bottle feeding), and appropriately measure the outcome (obesity).
This pilot study used a novel research design for evaluating the effects of delivery mode (breast vs. bottle) on growth and body fatness during the first 6 months of life. This study design can assess the contribution of exposure to bottle feeding as a risk factor for early accelerated growth and fatness. On a practical level, this study also is the first published report of growth and body composition patterns in infants fed significant quantities of pumped breastmilk.
Using this novel research design to examine early growth and fat deposition patterns in infants, we observed that infants fed breastmilk grew similarly for the first 4 months of life regardless of the delivery mode. After the early differences in length between NG and BG groups resolved, the infants displayed comparable growth over the first 6 months in weight, weight-for-age z-score, weight-for-length z-score, BMI-for-age z-score, FM, %FM, FFM, and head circumference-for-age z-score. This is in contrast to the wealth of information available on infants fed human milk substitutes by bottle. Collectively, these studies suggest that infants may grow similarly for the first 2–3 months and then the rate of weight gain is significantly increased in formula-fed infants relative to breastfed infants.17,24 Infants who are breastfed for 9 months are, on average, 400 g lighter than formula-fed infants by the end of the first year; after 12 months of breastfeeding this difference increases to 600–650 g. 24 Studies are suggestive, but not conclusive, that this excess weight gain is due to accretion of excess body fat.24–26
A recent study using air-displacement plethysmography to evaluate growth and body fat differences between infants fed breastmilk and formula did not find any significant differences from birth to 3 months; 27 however, this may not be a long enough follow-up to detect between-group growth differences. To rule out the possibility that we were missing growth differences that were just emerging in the 4–6-month age mark, we also used the WHO growth velocity standards to determine if NG and BG infants differed in the prevalence of rapid weight gain during this period of time. We defined rapid weight gain as exceeding the sex-specific 85th percentile interval weight gain. Approximately 10% of NG infants and 33% of BG infants exceeded this limit for growth velocity, a difference that was not statistically significant in this small sample (p = 0.12) but would reach significance with approximately 75 infants per group. Interestingly, the proportion of infants exceeding the 85th percentile weight velocity in the 0–2- and 2–4-month intervals was nearly identical between BG and NG groups. Future studies with larger sample sizes should closely examine this high-risk period—the age when solid foods are often introduced in the diet. One study suggests that growth diverges when solid foods are introduced because breastfed infants compensate for the additional solid food calories by proportionally decreasing breastmilk consumption. Formula-fed infants did not make this compensation, perhaps because they were encouraged by caregivers to continue to consume the expected amount of formula. 28
The study design presented here has two major strengths. First, the NG and BG mothers tend to be fairly similar in lifestyle and demographic variable as mothers in both groups were likely to initiate breastfeeding at birth and continue breastfeeding during the 6-month study. The only statistical difference between groups of the demographic variables we assessed was employment: BG mothers were more likely to be employed full-time. Second, because we kept the substance fed (breastmilk) similar between groups, we could focus on assessing the independent effects of delivery mode (breast, bottle) on rapid infant growth. In order to achieve this objective, we had strict inclusion criteria for enrollment, and many dyads were eliminated during construction of the final sample for data analysis. We wanted to ensure the NG dyads had very limited use of bottles and formula and that the BG dyads had limited use of formula but regular and significant exposure to bottlefeeding. While this allows for an improved study design and it allows us to evaluate the growth of infants exclusively fed breastmilk but by both bottle and breast, the results may not apply to the large population of U.S. infants who are fed mixed diets of breastmilk by breast, breastmilk by bottle, and supplemental formula.6,7 Future research should carefully evaluate the growth of infants fed in the spectrum of methods used today, to independently assess the role of delivery mode (breast, bottle) and substance (human milk, milk substitute) in producing the risky growth patterns that may predispose an infant to later obesity.
One limitation of this design that we cannot rule out is whether the breastmilk may differ in some crucial way when delivered by the breast versus by bottle. Studies have not shown a role in foremilk–hindmilk fat level differences in producing infant satiety, which suggests this difference between delivery modes would not affect growth and caloric intake.29,30 Studies of pasteurized human milk suggest that the pasteurization process may partly destroy growth regulating bioactive factors such as leptin 31 and, when bottlefed to infants, produce short-term reductions in caloric intake and growth. 32 The mothers in this study did not pasteurize their milk; however, in the absence of evidence to the contrary we cannot rule out that refrigeration and/or freezing in household refrigerators affects growth-regulating substances in the milk.
A second limitation of the study is the small sample size in each group. In order to limit the feeding conditions to which the infants were exposed, strict recruitment criteria were used, and a substantial number of subjects were eliminated in constructing the final sample. This study serves as an appropriate pilot study to examine the sample size needed to detect growth differences between NG and BG infants during the first 6 months of life. Based on the small average group differences we observed in key growth and body composition variables, we estimate that between 100 and 200 subjects per group would be necessary for these differences to become statistically significant and approximately 75 in each group to detect growth velocity differences in the 4–6-month interval. However, it is important to note that these differences may be statistically significant but impractical in the real world. These differences may not result in meaningful effects on overall lifetime risk for overweight. Future studies that follow the infants for longer duration should examine whether these differences in growth resolve over time or whether they increase after 6 months, as seen in previous detailed comparisons of growth of breastfed and formula-fed infants. 33
A third limitation is the lack of objective measured intake of breastmilk and formula, as well as the amount of breastmilk consumed by breast and bottle. The NG group received nearly 100% breastmilk, 100% by breast across the 6 months of the study. Most NG parents never fed formula or breastmilk by bottle, and the few who did explained that these unique situations were memorable. Thus, the parental estimate of intake shown in Figure 1 is very likely to be accurate for NG infants. The BG group had a more complicated path to estimating monthly intakes of substance and feeding mode. The parents were asked to consider various aspects of feeding mode when answering the series of questions that ultimately result in the data shown in Figure 1, such as changes in feeding mode across the week (weekdays vs. weekends) or larger trends in feeding that occurred across the month. We asked them to consider number of feedings by bottle and breast as well as to consider bottles that had mixed contents. The fairly regular feeding schedule (substance and delivery mode) of these infants helped parents provide answers in which they felt confident. The families who had more complicated feeding regimens, who used significant amounts of formula, or who made dramatic transitions in breastfeeding and/or formula feeding across the study were excluded from these analyses, as they did not cleanly fall in to the NG or BG groups. This provides an extra layer of confidence when interpreting the study findings.
While this research design has strengths and limitations for studying the effects of bottle feeding behaviors on rapid infant growth, on a practical level this pilot study provides relevant and timely information on growth and body composition patterns of a small sample of infants nearly exclusively fed breastmilk, by both bottle and breast, during the first 6 months of life. As current Academy of Breastfeeding Medicine recommendations include exclusive breastfeeding for the first 6 months of life, 34 this study has monitored growth during the highest-risk period of time for infant growth failure in infants fed breastmilk. No evidence of growth failure was observed in the bottle-fed infants, and their growth and body composition was similar to nursing infants during all 6 months of the study. The only exception was the 4–6-month weight velocity, where the bottlefed infants were three times more likely to exceed the 85th percentile weight velocity than nursing infants. This finding was not significant, but the study was underpowered to detect this difference adequately. This pilot study, which is the first published study documenting growth and body composition patterns of infants fed significant quantities of breastmilk by bottle, demonstrates that this infant population can be studied and should be evaluated more thoroughly. Given the prevalence of pumping and bottle feeding of breastmilk in the United States,6,7 additional research on larger samples of infants is needed to understand the impact of these feeding choices on a variety of both maternal and infant health outcomes.
Conclusions
This prospective study suggests that infants who are nearly exclusively fed breastmilk during the first 6 months of life grow similarly for the first 4 months of life whether the milk is delivered through breastfeeding or a mix of breastfeeding and bottle feeding. Infants fed significant quantities of breastmilk by bottle had similar patterns of weight, length, weight-for-length, BMI, head circumference, and body fatness when compared with a reference group of breastfed infants. However, BG infants were three times more likely to exceed the 85th percentile for weight velocity during the 4–6-month age interval than NG infants (33% vs. 10%, respectively), but this did not reach statistical significance in this sample size (p = 0.12). More research is needed to verify these findings in a larger sample and to evaluate differences in parent feeding practices between these groups.
Footnotes
Acknowledgments
C.J.B. gratefully acknowledges financial support from the Penn State Children, Youth, and Families Consortium and The Huck Institute for the Sciences. Sincere appreciation is extended to Dr. Leann Birch, who contributed to the design of the study, Ms. Michele Marini, who assisted with data processing and analyses, and Ms. Darcy Gungor and Ms. Jenny Spino, who assisted with data collection. Our research team also thanks the mothers and babies who were so dedicated to this study.
Disclosure Statement
Breast pumps and feeding bottles/nipples were provided at no cost to mothers in the bottlefed breastmilk group by Philips Avent Inc. and Medela, Inc. These companies have not had any input into study design, data analysis, or the manuscript. C.J.B. declares no financial conflicts of interest.