
Abstract
Abstract
Background:
A significant number of mothers have breastfed their babies from one breast only or from one breast more than the other. They presented to the breast clinic with complaints that mainly involve the breast that was not used or less used for breastfeeding.
Methods:
The database of the Breast Unit at King Fahd Hospital, Jeddah, Saudi Arabia, was reviewed from April 1998 to March 2010. The lactation history of any patient coming to the breast clinic was documented, including number of children, duration of lactation, and the way they performed breastfeeding.
Results:
During the study period, 54 patients have breastfed their babies exclusively from one breast (Group 1), and 21 have breastfed from one breast more than the other (Group 2). Patients gave different reasons for this practice, with nipple retraction being the commonest. In Group 1, 46 of 54 (85%) presented with complaints in the breast that was not used for breastfeeding (unsuckled), and only eight of 54 (15%) presented with complaints in the used (suckled) breast (p = 0.000). In Group 2, 13 of 21 (62%) presented with complaints in the breast that was less used for breastfeeding (less suckled), five of 21 (24%) presented with complaints in the breast more used for breastfeeding (more suckled), and three of 21 (14%) presented with complaints in both breasts equally (p = 0.418).
Conclusion:
Mothers who practice unilateral breastfeeding are candidates for future development of different breast problems in the unsuckled/less suckled breast.
Introduction
Unilateral breastfeeding is practiced by some of our patients. They presented to the breast clinic with different complaints that involve the breast not used or less used for breastfeeding. In this study, we reviewed this breastfeeding practice and the pattern of disease development in this group of patients.
Patients and Methods
The database of the Breast Unit at King Fahd General Hospital, Jeddah, Saudi Arabia, has been reviewed from April 1998 to March 2010. During that period, 2,091 parous patients with different breast problems were seen. Of these, 54 patients have exclusively breastfed from one breast (Group 1), and 21 patients have breastfed from one breast more than the other (Group 2). In the lactation history, mothers were asked about the minimum and the maximum duration they practiced breastfeeding for all babies; duration of breastfeeding for each baby was not specifically asked for. (This is summarized in Table 5 as a range for the subgroup.)
Reasons why patients breastfeed from one breast were analyzed. History of breast disease and/or breast surgery was documented. The presenting complaints and the pattern of breast diseases were also documented.
Bilateral mammography was done for patients ≥40 years old and for those with clinical suspicion of malignancy, and bilateral breast ultrasound was done for patients <40 years old. For patients with an inflammatory condition or suspicion of abscess collection, only ultrasound was performed regardless of age. Histopathology results were only available for cases that required biopsy or surgical intervention.
Statistical analysis
In this study, all data values are expressed as numbers, percentages, averages, and ranges. Comparison between the lactating breast and the diseased breast was done by using a χ2 test to evaluate the association between the unsuckled/less suckled breast and occurrence of breast disease. A p value of <0.05 was accepted statistically significant. Statistical analysis was performed using software (SPSS version 12, SPSS Inc., Chicago, IL).
Results
Of 2,091 parous patients with breast problems seen over a 12-year period, 54 patients have exclusively lactated from one breast (Group 1), and 21 patients have lactated from one breast more than the other (Group 2). In the latter group, patients were inconsistent whether it was mainly less duration or less frequency of breastfeeding.
In both groups, patients were Saudis; the age range was 21–80 years (average, 41 years), and the parity range was 1–13 (average, 6). Age of the patient at the first breastfeeding episode was not documented. Duration of breastfeeding for each mother varied between one baby and another. The shortest (minimum) duration of breastfeeding was generally practiced for the first breastfeeding episode; then, for subsequent babies, mothers tend to breastfeed for longer periods. They were unable to recall the duration of breastfeeding for each child, especially when parity was as high as 13; however, they could estimate the minimum and the maximum duration they breastfed.
The right side was preferred for breastfeeding over the left (right-to-left ratio was 34:20 in Group 1 and 11:10 in Group 2).
In Group 1, 46 of 54 (85%) presented with complaints in the breast that was not used for breastfeeding (unsuckled breast), and only eight of 54 (15%) presented with complaints in the used (suckled) breast (p = 0.000). In Group 2, 13 of 21 (62%) presented with complaints in the breast less used for breastfeeding (less suckled), five of 21 (24%) presented with complaints in the breast more used for breastfeeding (more suckled), and three of 21 (14%) presented with complaints in both breasts equally (p = 0.418).
Reasons reported by patients for unilateral breastfeeding for both groups are summarized in Table 1. Some patients in Group 1 breastfed a few times from the unsuckled breast, but they stopped because of infant refusal or vomiting. None of them related her practice to social, occupational, or cultural reasons. For both groups, the presenting complaints are summarized in Table 2. Clinical examination did not show any discrepancy in size between the two breasts, but the unsuckled/less suckled breast felt thicker.
Three patients with bilateral breast pain were excluded.
In Group 1, 34 mammograms and 43 ultrasounds were available for review; however, three mammograms and 10 ultrasounds were not. In Group 2, 13 mammograms and 12 ultrasounds were available, but three mammograms and one ultrasound were not. Mammographic and ultrasonographic findings in each group are summarized in Table 3. There was no specific clinical or radiologic finding that characterizes the unsuckled/less suckled breast.
Three patients with bilateral breast pain were excluded.
The diagnosis of breast disease in these patients was based on clinical and radiologic assessment (Table 4). Some cases had pathologic confirmation by core needle biopsy or surgical intervention. All the discovered cases of breast cancer were invasive ductal carcinoma, not otherwise specified except one that was ductal carcinoma in situ. Table 5 summarizes breast cancer risk factors in each subgroup. None of the patients who developed breast cancer in our study had a positive family history of breast or ovarian cancer.
Three patients with bilateral mastalgia were excluded.
Histologic confirmation available.
Positive family history of breast cancer in one patient in each of these subgroups.
One patient in this subgroup was smoking 20 cigarettes per day for 5 years.
One patient in this subgroup used oral contraceptive pills (OCP) inconsistently between her 11 pregnancies.
Discussion
Unilateral breastfeeding is an unusual practice about which our patients only occasionally talk. Some will voluntarily mention this information when they complain about their breast, and they will refer to the unsuckled/less suckled breast as a diseased breast.
Our patients were Saudis coming mainly from the western region of the Kingdom by virtue of the location of our center. There is nothing in our customs or traditions that influence the pattern of breastfeeding. In fact, in our culture, breastfeeding is encouraged, mothers speak about it proudly, and they prefer to breastfeed for as long as they can, preferably for 24 months as dictated by our religion (Islam). Some of them would even consider a short period (e.g., a few months) of breastfeeding as if they did not breastfeed.
Our youngest patients were 21 years old, but the age of the patients at the first breastfeeding episode was not documented. We do not have any data to support the proposal that unilateral breastfeeding practice is related to inexperienced young mothers. Multiparity (as high as 13 children) and long durations of breastfeeding (up to 24 months) did not prevent mothers from continuing unilateral breastfeeding because of fear of lactating from a diseased breast. We did not check if our patients were right- or left-handed, but the preference for the right side was mainly related to an easier position during breastfeeding. Some patients mentioned more than one reason for unilateral breastfeeding. The combination of nipple retraction and strange milk color and odor was fairly common. Some patients actually tasted the breastmilk and found it salty. They were convinced that this milk was different or actually produced by a diseased breast. Nipple retraction was the commonest reason mentioned by our patients (Table 1) because the baby will not be able to latch on the nipple. This is a problem in moderate and severe cases only. Mild nipple retraction can be overcome by encouraging breastfeeding in the immediate postpartum period and before the breast become significantly engorged with milk. If breastmilk was not evacuated properly, mammary ducts will distend, and secretions stagnate within the ducts and may cause inflammation and sometimes superadded infection. Repeated inflammation can occur with every episode of breastfeeding and will further worsen nipple retraction due to fibrosis.
Our patients commonly present with pain (Table 2). The majority point to the nipple and retro-areolar area as the most painful spot, and from there, pain may radiate to the whole breast. Pain can be due to distention of the ducts that was building up with each episode of lactation. It can also be due to inflammatory processes or fibrocystic changes. It was reported that stimulation of inflammatory pathways leads to reactive tumor stroma that cause mammary hyperproliferation, progression to fibrosis, and development of neoplasia. 5 The relation between mammary epithelium and stroma as a stimulus for future disease development is a major research subject; lactation may beneficially affect this relation. 3
There was no specific radiologic finding that characterizes the unsuckled/less suckled breast (Table 3); however, asymmetric parynchymal density was a common mammographic finding (Fig. 1). Asymmetric parynchymal density in the retro-areolar area in patients with unilateral nipple retraction (Fig. 2) correlated with duct ectasia on ultrasound. Other patients were found to have fibrocystic changes on ultrasound, but this was not in the direct retro-areolar location. Mammographic density is considered an important risk factor for the development of breast cancer. 6 Radiologic findings of malignancy in our patients (for example, stellate lesion on mammogram or ill-defined hypo-echoic lesion on ultrasound) were the same as in any case of breast cancer. Normal mammograms and breast ultrasounds were found in patients presenting with breast pain with no obvious underlying pathology.
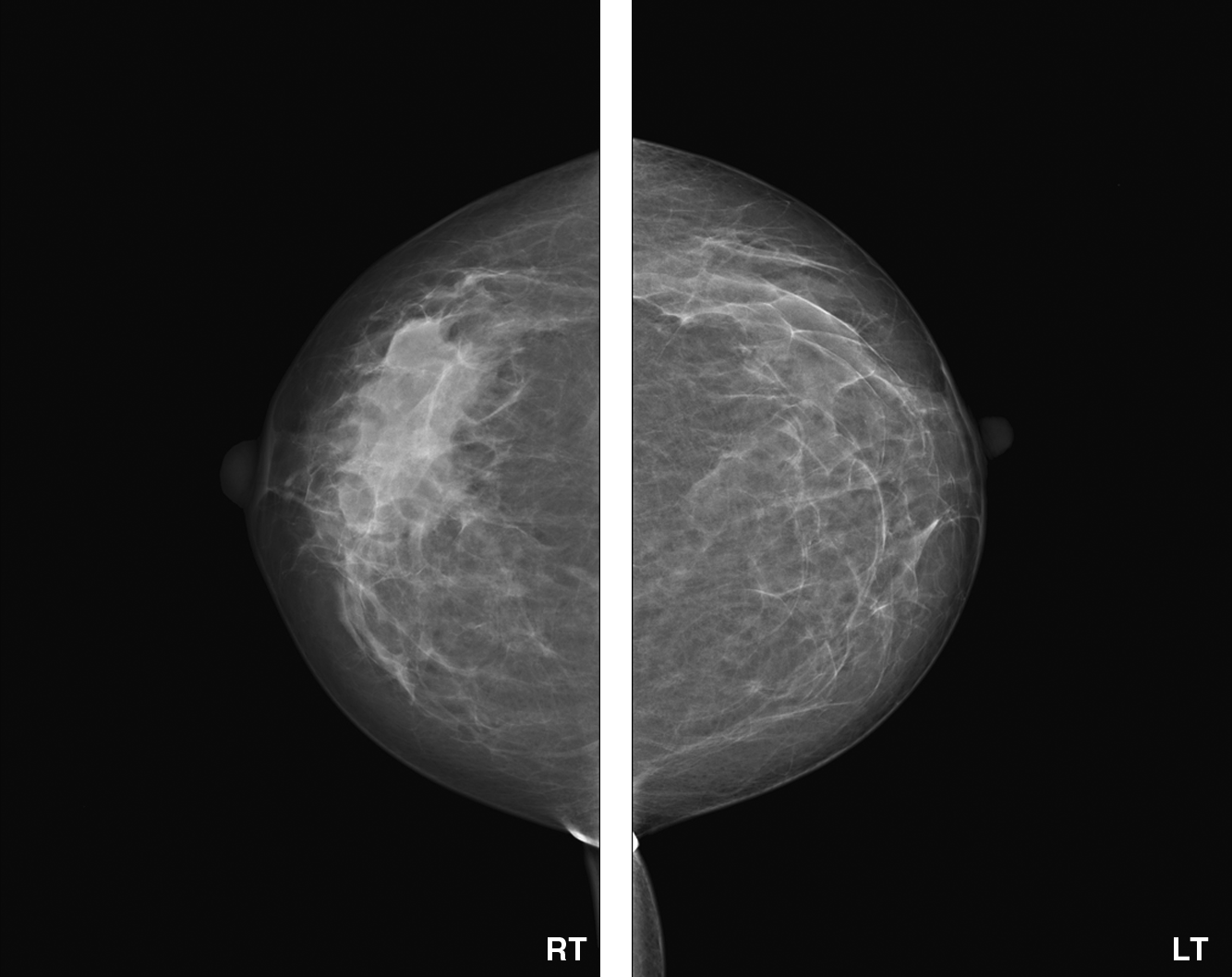
Bilateral mammography: Craniocaudal view of a 43-year-old woman who breastfed from the left breast exclusively showing right asymmetric parynchymal density.
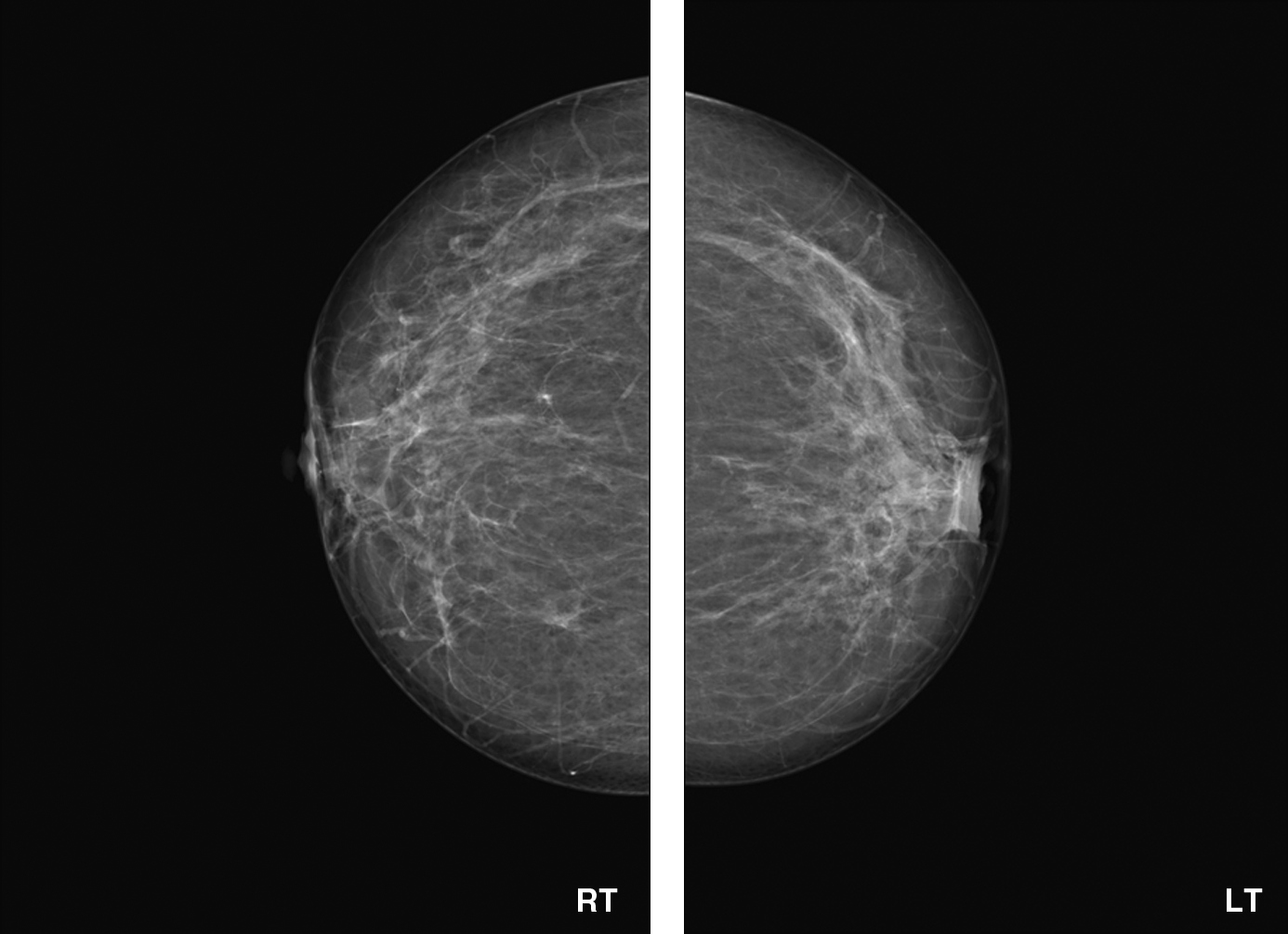
Bilateral mammography: Craniocaudal view of a 46-year-old woman who breastfed from the right breast exclusively because of left nipple retraction showing left asymmetric parynchymal density in the retro-areolar area.
Our patients practiced unilateral breastfeeding for the first child and continued for subsequent children. They are convinced that this breast is diseased or not functioning. It has been reported that after breastfeeding several children from one breast, the other breast completely cease to function. 7 Byers et al. 8 proposed that the inability to breastfeed due to insufficient milk supply could be due to malfunctioning of the breast tissue, and they found that the risk of breast cancer was greater among this group.
Table 4 shows the pattern of breast disease in each group. The unsuckled breast is mainly affected by acute and chronic inflammatory conditions like abscesses and granulomatous mastitis. We believe that this might be related to the unrelieved milk engorgement that causes overdistention of the ducts with subsequent disruption in the duct wall and possible extravasation of milk into the surrounding stroma. 9 Symptomatic duct ectasia that is associated with pain or palpable abnormalities and fibrocystic changes are significant finding in the unsuckled/less suckled breast. Breast pain (mastalgia) that was not related to any clinical or radiologic finding is a common diagnosis in both groups and subgroups. In Group 2, three patients (14%) presented with mastalgia in both the less suckled and the more suckled breasts equally. This may not be related to the breastfeeding practice because mastalgia is the commonest breast symptom that women of any age group can present with. In Group 1, three patients developed invasive ductal carcinoma in the unsuckled breast. They had no risk factors for developing breast cancer. It has been reported that Chinese Tanka (boat people) women breastfeed with only the right breast by custom. They have three- to fourfold increases in the risk of cancer developing in the unsuckled left breast for patients 55 years old and over. 10 From our small sample size, it is difficult to conclude that breast cancer was due to unilateral breastfeeding.
Different theories have been reported about the mechanism for a protective effect of lactation on the breast tissue. For example, breast fluid estrogen levels are suppressed for several years after lactation; this may diminish breast cancer risk by altering the hormonal milieu.1,2 Breastmilk protects the breast tissue by excretion of fat soluble carcinogens; the level of a potential carcinogen, cholesterol β-epoxide, is lower in the breast fluid of women during lactation and for up to 2 years after lactation. Also, lactation may alter the breast tissue so that it is less exposed to potential carcinogens and more exposed to potentially protective agents. 2 Direct physical changes in the breast that accompany milk production may also contribute to the observed protective effect.3,4 Our patients have a persistent hormonal influence on the breast lobules on the side not used for breastfeeding. They lack some or all of these protective mechanisms in the unsuckled/less suckled breast. By allowing the natural process of breastfeeding, the breast tissue will be relieved and subsequently protected from developing diseases in the future.
We believe that the only significant reason for unilateral breastfeeding is moderate or severe nipple retraction. Other factors are subjective, and unless we examine our patients during breastfeeding we will not be able to prove that the breast is actually diseased or is producing inedible milk. During our practice, we are discussing this observation with our patients as well as midwives and nurse educators. So far, a minimal change in this practice was observed, and longer follow-up is required to document that.
Conclusions
We are not sure whether the unsuckled/less suckled breast is actually diseased or malfunctioning as our patients believe. However, it is clearly evident that unilateral breastfeeding is associated with morbidities that can be prevented in some cases. We believe that unilateral breastfeeding is practiced—but unnoticed—in all societies and that speaking about it will encourage other investigators to dig into a patient's history and may find it related to different breast diseases.
If we educate the future moms and encourage them to properly breastfeed, then we can minimize the practice of unilateral breastfeeding and the morbidity associated with it.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contribution of Ghassan Baslaim, M.D., for the help with data analysis.
Disclosure Statement
No competing financial interests exist.