
Abstract
Abstract
Background:
Human immunodeficiency virus type 1 (HIV-1) transmission through breastmilk is the chief modality through which HIV-1 is transmitted from HIV-1-infected mothers to their babies in developing countries, where alternative feeding options lack practical feasibility. The development of an approach to inactivate the HIV-1 virions ingested by an infant on a daily basis through breastmilk is thus of critical importance.
Methods:
Copper has potent virucidal properties. Stoichiometric concentrations of copper ions inactivate the HIV-1 protease, which is essential for viral replication. Cell-free and cell-associated HIV-1 infectivity is inhibited when the virus is exposed to copper oxide in a dose-dependent manner. Passage of high titers of a wide range of HIV-1 isolates, spiked in culture medium, through filters containing copper oxide powder resulted in their deactivation.
Results:
In the current study, we demonstrate that the infectivity of three different HIV-1 isolates, spiked in breastmilk obtained from HIV-1-seronegative donors, or of wild-type isolates found in breastmilk obtained from HIV-1-seropositive donors, is drastically reduced (>98%) when exposed to copper oxide.
Conclusions:
This study is proof of concept that copper oxide is efficacious against HIV-1 found in breastmilk and serves as the basis for further research aimed at determining the possible effects that copper may have on the nutritional and anti-infective properties of breastmilk. Furthermore, this supports the continuing study of the feasibility of developing a filtering device, such as an “at-the-breast” disposable shield that can be used discreetly and safely by HIV-1-infected mothers during breastfeeding.
Introduction
Estimates of the postnatal transmission rate with no mother/baby interventions vary, with reports ranging from 15%5,6 to 39%7,8 in sub-Saharan Africa among study groups of HIV-positive women who breastfed for an extended period of about 2 years and were anti-retrovirus-naive after birth. A Zambian study 8 reported that for 514 infants still breastfeeding at 6–12 months, when neither the mother nor the infant received a preventive MTCT intervention, the estimated vertical transmission rate was 39.3%.
Breastfeeding HIV transmission risks remain throughout the feeding duration. Furthermore, data suggest that this risk is variable because of a complex interaction between the mother's “infectiousness” and the baby's “susceptibility” 9 at the systemic and mucosal levels, including infant intestinal patency, feeding patterns, infant immunity, maternal viral load, maternal co-morbidity such as mastitis, maternal advanced disease, nutritional factors, viral characteristics, and infant intestinal inflammation/immune activation (as reviewed by Kourtis et al. 1 and Walter et al. 9 ). Yet, evidence showing nearly equivalent infant morbidity and mortality when breastfeeding was replaced with mixed or replacement feedings led the World Health Organization to reiterate that “mothers known to be HIV-infected (and whose infants are HIV uninfected or of unknown HIV status) should exclusively breastfeed their infants for the first 6 months of life, introducing appropriate complementary foods thereafter, and continue breastfeeding for the first 12 months of life. Breastfeeding should then only stop once a nutritionally adequate and safe diet without breastmilk can be provided.” 10
Other than nutritional factors, human milk contains anti-infective factors, developmental-stimulating growth factors and hormones, immune function modulators, and anti-inflammatory agents that confer protection against disease and reduce infant morbidity and mortality in spite of harsh environments.11,12 Even when breastmilk is HIV infected, advantages exist for the vulnerable infant to breastfeed exclusively, which for developing, under-resourced nations is an efficient and sustainable phenomenon.9,13
Sustainable technology to prevent breastmilk MTCT of HIV is lacking. We propose the use of copper. Copper ions, either alone or in complexes, have been used for centuries to disinfect fluids, solids, and tissues.14,15 Copper or copper-containing compounds have potent antiviral properties. 16 The deactivation by copper of infectious bronchitis virus, poliovirus, herpes simplex virus, and other enveloped or non-enveloped, single- or double-stranded DNA or RNA viruses has been reported (reviewed by Borkow and Gabbay 16 ). HIV-1, both free and even 3 hours after infecting cells, is inactivated by cupric ions. 17 Stoichiometric concentrations of copper ions inactivate the HIV-1 protease, 18 an essential protein for assembly and replication of the virus. Copper ions may cause nonspecific damage to HIV by damaging the envelope phospholipids and denaturing the virus nucleic acids. 16
The capacity of copper oxide–containing filters to reduce infectious titers of a panel of viruses spiked into culture medium, including HIV-1, has been demonstrated.19,20 These filters very efficiently reduced the infectious viral titers of all HIV-1 isolates tested, including wild-type and drug-resistant isolates, laboratory and clinical isolates, and isolates from varying clades. Just a few minutes of exposure of the virions to the copper oxide powder in the filters rendered them non-infectious. Copper oxide affected free viruses, virions being formed within the cytoplasm of cells during the cell exposure to copper, and virions prior to their budding from the cells. Cell-associated HIV-1 transmission was also attenuated in a dose-dependent manner by copper oxide. The multisite, antiviral mechanism of copper oxide 16 explains the high susceptibility of all HIV-1 isolates tested, with no clade or other specificity.
As opposed to copper sulfate or other copper salts, copper oxide is poorly soluble in aqueous solutions. 21 The amount of copper that is expected to leach out into the milk as it passes through copper oxide–containing filters is less than 1 μg/dL. This is based on measurements of copper that leached into aqueous and lipid solutions as they passed through copper oxide–containing filters (authors' unpublished data). Copper is an essential element for humans; its biochemistry has long been studied and is well understood. 22 Excess copper in humans at the level that is expected to be leached out into the milk as it passes through the copper-containing filters is not toxic. 23 On the contrary, copper oxide is widely used in vitamin supplements as the source of copper. The USA National Academy of Sciences Committee noted that daily intakes up to 3 mg/day in children and 8–10 mg/day for adults are considered tolerable and nontoxic. 23
This study, which was aimed at determining, as a proof of principle, if copper oxide can be used to deactivate HIV-1 in human breastmilk, serves as a basis for future development of a filter strategy tailored to the uniqueness of the maternal–child dyad feeding relationship within cultural sanctions of resource-poor societies. More specifically, our goal is to explore the development of a copper oxide–containing, single-use, disposable at-the-breast device, which can be used discreetly and safely by HIV-1-infected mothers during breastfeeding.
Materials and Methods
Breastmilk samples
Twenty breastmilk samples were obtained from HIV-1-seronegative women between birth and 8 weeks postpartum, presenting for clinical care at the Shaare Zedek Medical Center, Jerusalem, Israel. These were unused milk samples frozen immediately after breast pumping and kept frozen until used. In addition, 20 breastmilk samples (∼80 mL) were obtained from HIV-1-seropositive, anti-retroviral-naive women between birth and 8 weeks postpartum presenting for clinical care at the Langata and Pumwani maternity clinics, in Nairobi, Kenya, following the approval of the Texas Tech University Health Sciences Center and Kenyatta National Hospital Institutional Review Boards. These breastmilk samples were collected with a Medela (McHenry, IL) Symphony® Plus hospital-grade double electric breast pump. This pump is known to mimic the baby's nursing rhythm, and it is specifically designed for a faster let-down and milk flow. The donated milk samples of the HIV-1-seropositive women were put in sterile containers and used fresh within 3 hours of donation.
Donor recruitment
The HIV-1-seropositive donors were identified through health providers' referrals at the Langata and Pumwani City Council of Nairobi maternity clinics. The health providers explained the study in Swahili, the most common language of Kenya, and the donors signed the informed consent forms. All women who agreed to participate in the study were compensated with a cotton baby blanket and 1,500 Ksh (approximately $20 US).
Viruses
HIV-1IIIB (clade B, X4), HIV-1 MVP5180 (clade O, X4R5), and azidothymidine-resistant HIV-1 (clade B, X4) clinical isolates were tested with breastmilk obtained from HIV-1-seronegative donors. HIV-1IIIB and HIV-1 MVP5180 were obtained from the NIH AIDS Research and Reference Reagent Program (Rockville, MD); the clade B clinical isolate was obtained at Kaplan Medical Center (Rehovot, Israel). All isolates were propagated by subculture in MT-2 cells. Clarified supernatant fluids containing 105–108 50% tissue cell culture infectious doses (TCID50)/mL served as viral inocula.
Detection of HIV-1 infection
Viral growth was assessed by (a) microscopic assessment of syncytium formation by two independent observers of HIV-1 infection of CD4+ MT2 cells. The titer was calculated by using the end point dilution method of Reed and Muench 24 or (b) determining the number of infected cMAGI cells. 25 MT2 and cMAGI cell lines were cultured in RPMI 1640 medium (Biological Industries, Israel Beit Haemek Ltd., Kibbutz Beit Haemek, Israel) containing 10% fetal calf serum (Biological Industries) and 1% antibiotics (Pen-Strep-Nystatin suspension, Biological Industries). The cMAGI cell line is a lymphocyte cell line stably transfected with a plasmid containing the HIV-1 long terminal repeat fused to β-galactosidase. 26 These cells stain blue only when infected with HIV-1.
Finding a suitable membrane
After we consulted with membrane manufacturers, the following four membranes—Versapor® 800, GN-4 Metricel®, type A/E glass fiber, Super®-1200 (Pall Corp., Ann Arbor, MI)—and a filter device already containing an integrated membrane, Sartopure 300® (Sartorius Stedim, Goettingen, Germany) were selected for analysis. Twenty milliliters of different breastmilk samples, obtained from HIV-1-seronegative donors, was mixed with up to 500 mg of one of the six different copper oxide powders tested and thoroughly and constantly stirred for 5 minutes at room temperature with a vortex-mixer to maintain the copper oxide particles in suspension. The breastmilk alone and the aliquot exposed to the copper powder then were passed at a flow rate of ∼5 mL/minute with a peristaltic pump through the four membranes tested by using a 25-mL syringe and a 37-mm in-line membrane holder (Pall Corp.) or were passed directly through the Sartopure 300 filter. For the Sartopure 300 filters, 40 mL of breastmilk was used per filter as the void volume of the filter is ∼25 mL, and to get milk out of the filter at least 35 mL needed to be applied to it. The copper oxide powders had a D50 particle size (50% of the particles above this value) of 1.5 up to 18 μm. The capacity of the milk to pass through the filters without clogging the filters and the capacity of the filters to prevent the passage of the copper oxide particles were determined by visual observation.
Inhibition of HIV-1 infectivity of breastmilk samples
Next, 20–100-mL aliquots of breastmilk obtained from HIV-1-seronegative donors were spiked with HIV-1 at 105 TCID50/mL and mixed with copper oxide powder at 0.2–3 mg/mL. After being constantly and thoroughly mixed for 5 minutes at room temperature, the samples were passed through the membranes or the Sartopure 300 filter as described above. The eluates were collected and subjected to multiple sequential dilutions in appropriate culture medium. Each dilution was then added to 2 × 105 MT-2 or cMAGI target cells in 96-well microplates using three replicate wells per dilution. After 2 hours of incubation at 37°C, the cells were washed thoroughly and incubated in a humidified CO2 incubator at 37°C. Viral infectivity was determined after 3–5 days of incubation at 37°C in a moist 5% CO2 incubator, as described above. Breastmilk without virus, passed through the membrane, was used as a negative control for viral activity. HIV-1-spiked milk samples to which no copper powder was added served as positive controls for HIV-1 infectivity. Three different breastmilk samples were tested for each HIV-1 isolate examined. The percentage reduction of the infectious HIV-1 titers was determined by the following formula: (100 – [A/B]) × 100, where A is the titer of the virus in the milk after the milk exposure to copper oxide particles and filtration (treatment) and B is the titer of the virus in the milk after filtration (control). The log reduction was calculated as log10 TCID50/mL of the titer obtained from the control minus the log10 TCID50/mL of the treated sample. Data are the mean and SD values obtained by three separate experiments. Breastmilk samples obtained from HIV-1-seropositive donors were subjected to the same treatment but without adding any virus to them. In brief, the 80-mL milk aliquots were divided into two: 40 mL was kept as is, and 40 mL was mixed with 120 mg of copper oxide powder. After 5 minutes of thorough and constant mixing of both samples, each sample was passed through a Sartopure 300 filter, and the viral infectivity of the eluates, as determined on target cells, was examined during 3 weeks of incubation.
Results
The fatty layers of the breastmilk passed through the membranes remained in the Versapor 800, GN-4 Metricel, and Super-1200 membranes, and elution of mainly the aqueous layer occurred (Table 1). These membranes were clogged especially when early breastmilk, rich in fat, was tested. The type A/E glass fiber membrane and Sartopure 300, with pore sizes of 1 and 5 μm, respectively, were not clogged and did not affect the milk integrity. Thus, they were further examined for their capacity to block passage of six copper oxide powders, of varying particle size, added to breastmilk samples. The glass fiber membrane was found unworkable, as it was clogged by all the copper oxide powders tested or some of the copper powder passed through the membrane during filtration. With the Sartopure 300 filter, five out of the six powders tested clogged or passed through it; however, one copper oxide powder did not clog or pass through the Sartopure membrane, even when 100 mL of breastmilk containing 300 mg of copper oxide was filtered. This copper oxide powder has a D50 of 18 μm and no particles below 6 μm (Fig. 1). Further studies were thus performed with this powder and Sartopure 300.
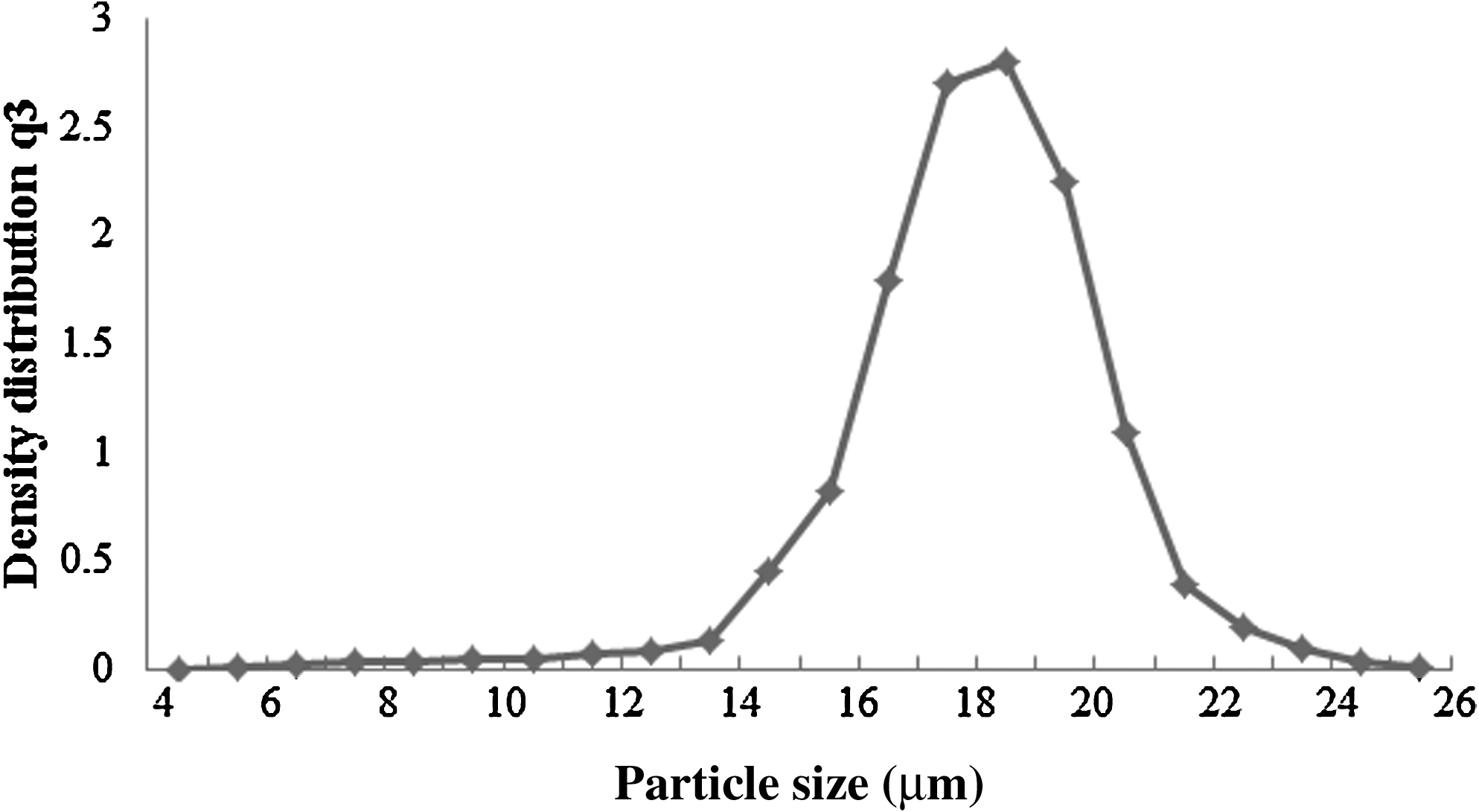
Particle size distribution of the copper oxide powder used.
As detailed in Table 2, above 98% reduction of HIV-1 infectivity was achieved with all laboratory isolates when using 2 mg/mL copper oxide powder. Among 20 samples obtained from HIV-1-seropositive women and tested, HIV-1 could be cultured from four samples only. It is important that in all four samples in which HIV-1 was detected, the exposure of the milk samples to 3 mg/mL copper oxide resulted in 1.8, 1.8, 2.4, and 3 (2.25 ± 0.57; mean ± SD) log reductions (>99% reduction) in infectious viral titers compared with the infectious titers found in the same samples passed through the same filters but not preexposed to the copper oxide powder (Table 3).
The virus was tested after being exposed to 2 mg/mL copper oxide powder for 5 minutes.
TCID, 50% tissue cell culture infective dose.
The virus was tested after exposure to 3 mg/mL copper oxide powder for 5 minutes.
Discussion
Prior to testing the capacity of copper oxide particles to deactivate HIV-1 in breastmilk donated from HIV-1-seropositive women in cell culture experiments, two main technical/developmental difficulties needed to be addressed. First, we needed to find a suitable membrane through which breastmilk can readily pass without altering the milk composition, as breastmilk is a complex mixture of fats, proteins, carbohydrates, and minerals in an aqueous solution. Second, we needed to make sure that these membranes would block passage of copper oxide particles, as these particles would kill the cell cultures. After solving the above-described technical difficulties, we examined the capacity of varying amounts of the copper oxide powder to reduce HIV-1 infectivity when incubated at room temperature for 5 minutes with HIV-1-spiked breastmilk samples obtained from healthy HIV-1-seronegative donors. We found that while 2 mg/mL copper oxide powder resulted in very efficient reduction of the infectivity of the laboratory HIV-1 strains (above 98%), it did not completely abolish the infectivity. Therefore, in order to assure efficacy, it was decided to use 3 mg/mL copper oxide when testing the efficacy of the copper oxide particles in reducing HIV-1 infectivity in fresh samples obtained from HIV-1-seropositive women. Similar reduction (∼99%) of HIV-1 infectivity was obtained with fresh samples obtained from HIV-1-seropositive women. Although absolute neutralization of HIV infectivity was not achieved, we presume that a reduction of >98% in the infectious HIV-1 units present in the breastmilk following exposure of the milk to the copper oxide particles would significantly reduce the risk of a baby becoming HIV infected as a consequence of breastfeeding. This assumption is strongly supported by the careful analysis conducted by Richardson and Hughes 27 of data gathered in a previous study 28 that examined HIV-1 MTCT in a cohort of 358 HIV-1-infected anti-retroviral-naive breastfeeding women. Richardson and Hughes 27 calculated that the breastmilk infectivity rates per day of the children breastfeeding from mothers with prenatal HIV-1 RNA plasma viral loads above the median viral load (43,120 copies/mL) was approximately fourfold higher than those of children breastfeeding from mothers with prenatal HIV-1 RNA plasma viral loads below the median viral load (0.00044 [95% confidence interval 0.00019, 0.00075] versus 0.00011 [95% confidence interval 0.00003, 0.00025], p = 0.01). Similarly, studies of HIV-1-infected breastfeeding mothers participating in postnatal anti-retroviral regimens have reported lower MTCT rates among infants of women with lower viral loads29,30 or higher CD4 counts. 31 CD4 counts are inversely related to viral load. 32 These data suggest the accumulative risk of a breastfeeding infant becoming HIV-1 infected, which increases as the duration of breastfeeding lengthens, 33 would be reduced considerably by plummeting the sheer numbers of infectious HIV-1 units within the milk to less than 2%. Such a drop in exposure potentially represents a significant reduction of the 25–45% rates, without perinatal anti-retroviral regimens, of MTCT of HIV-1 attributed to usual and customary breastfeeding in sub-Saharan Africa. 34
Although recent MTCT rates under the influence of perinatal anti-retroviral regimens are reported to be 2.6–4.1%, 31 in sub-Saharan Africa tremendous gaps in access to such regimens within and between counties now and in the future exist. 35 Only about one-third of people estimated to be in need of HIV anti-retroviral treatment have access, 36 a fact that motivated the recent Treatment 2.0 Initiative, coordinated by UNAIDS and the World Health Organization. This initiative calls for “radical simplification, innovation in drug design and diagnostics, renewed commitment and resources, and adapted delivery systems,” 37 to provide universal HIV treatment with sustainability. We propose that an “at-the-breast” device could serve as an adapted delivery system that deactivates and delivers less risky breastmilk to the infant.
Given the lifetime burden of HIV/AIDS care for infants who acquire HIV via breastfeeding and the shortened mortality when care is not available or is inconsistent, a device that shows promise to dramatically reduce viral load in breastmilk warrants further research and development, which would include evaluation of the influence of copper on the functioning of anti-infective properties of breastmilk, determination of the amount of copper leaching into breastmilk followed by toxicity studies using an infant animal model, maternal/infant human factor testing, and, ultimately, human clinical trials.
We have shown in previous studies that free-flow passage of medium containing HIV-1 or other viruses through filters containing copper oxide results in significant reductions of the viral infectious titers.19,20 In the present study, we were able to demonstrate that HIV-1 infectious titers, both when HIV-1 is spiked in high titers to non-infected breastmilk samples and, more importantly, when present in breastmilk of HIV-1-seropositive women, could be significantly reduced when the virus was exposed to copper oxide for 5 minutes. These results are a proof of principle that copper oxide can inactivate HIV-1 also in human breastmilk and serve as the impetus to further explore the possibility of using copper oxide in the context of reduction of MTCT.
Obviously further development is necessary. Because it has been shown that soluble copper ions neutralize HIV-117,18 and because copper oxide particles serve as a reservoir of copper ions, a filtering device with copper oxide particles with a significant, smaller particle size should be developed. In the current study, because of the technical problems described above, very large copper oxide particles of a mean diameter of 18 μm were used. Assuming the particles are spherical, then the surface area is 4 × π × (particle radius) 2 . A particle of 18 μm diameter has a surface area of ∼1018 μm2. Assuming we would use particles of 1 μm diameter, then in the same volume that an 18-μm particle occupies, ∼5,832 particles of 1 μm can be introduced. A particle of 1 μm diameter has a surface area of 3.14 μm2. Thus 5,830 particles of 1 μm have a surface area of 18,312 μm2, which is ∼18 times the surface area of the 18-μm particle. Therefore, using smaller particle size would increase very significantly the surface area of the copper oxide in contact with the milk, allowing for significantly higher copper ion release. Ideally, the copper oxide powder should be in the nanometer to micron particle size range. Such particle size may allow reducing significantly the exposure time needed to achieve >98% reduction of HIV-1 infectivity. It may be that increasing the surface area by 18-fold would reduce the needed exposure time to achieve the same reduction of the viral titers by 18 (i.e., in order to receive a 98% reduction instead of 5 minutes of exposure, ∼17 seconds would suffice). Obviously this assumption needs to be verified experimentally.
The positive results of this study strongly encourage us to explore the development of a filter strategy tailored to the uniqueness of the mother–child dyad feeding relationship within cultural sanctions of resource-poor societies. More specifically, we hope to develop a copper oxide–containing, single-use, disposable at-the-breast device that can be used discreetly and safely by HIV-1-infected mothers during breastfeeding, perhaps similar to a conventional breast/nipple shield in design. Given, however, that studies on conventional nipple shields lack rigor and report contradictory risks and benefits associated with use, 38 a departure from previous nipple shield designs may be necessary. Obviously, the copper-impregnated device proposed will require an evidenced-based design process that is accompanied by bioengineering and breastfeeding expert guidance. A safe, user-friendly device, designed with lactation anatomy and physiology and cultural specificity in mind, is our overarching goal and consistent with the recent scale-up initiative in HIV treatments announced by UNAIDS and the World Health Organization and with U.S. Food and Drug Administration device research and development processes.37,39 The reason of having a single-use, disposable device would be to avoid problems of loss of efficacy and contamination of the device. Such a device would need to be inexpensive for effective global dissemination and access.
We aim at developing a breast shield containing extremely small copper oxide particles, which will most probably be embedded in the nipple section base material. This may be done in parallel to using a fine metallic copper mesh to further increase antiviral efficacy. The breast shield should be designed in a way that will allow sufficient exposure time of the breastmilk to the copper for the viral neutralization to occur. Achieving this should not affect the capacity of the baby to suckle breastmilk through the breast shield and should not allow the release of copper oxide particles into the breastmilk. The development goal remains to significantly reduce the HIV-1 infectious titers and the risk of HIV-1 MTCT.
Footnotes
Acknowledgments
This work was funded by a grant from the Bill & Melinda Gates Foundation through the Grand Challenges Exploration Initiative and further supported by the Texas Tech University Health Sciences Center Florence Thelma Hall Endowment and the Laura W. Bush Institute for Women's Health.
Disclosure Statement
No competing financial interests exist.