
Abstract
Abstract
Objective:
This study investigated possible influences of medical interventions during labor on maternal blood pressure during a breastfeed 2 days postpartum.
Subjects and Methods:
Sixty-six primiparae with normal deliveries were consecutively recruited. Blood pressure was measured at –5, 10, 30, and 60 minutes during a morning breastfeed 2 days postpartum. Five treatment groups were formed based on the medical interventions received during labor: Non-medicated mothers (Control group, n=21); mothers receiving epidural analgesia (EDA) with oxytocin (OT) stimulation (EDAOT group, n=14); mothers receiving EDA without OT stimulation (EDAnon-OT group, n=7); mothers receiving OT stimulation only (OT intravenously [iv] group, n=9); and mothers receiving 10 IU of OT intramuscularly (im) only (OT im group, n=15).
Results:
Baseline diastolic, but not systolic, blood pressure differed between the groups as displayed by significantly lower diastolic blood pressure in the EDAnon-OT group compared with the Control group, the OT iv group, and the EDAOT group (p=0.045, p=0.041, and p=0.024, respectively). Both systolic and diastolic blood pressure fell significantly during the breastfeeding session in the Control group (p=0.001 and p=0.004, respectively), the OT im group (p=0.006 and p=0.001, respectively), and the EDAOT group (p=0.028 and p=0.002, respectively), and the fall in diastolic blood pressure tended to be significant in the OT iv group (p=0.050). The duration of skin-to-skin contact before breastfeeding correlated positively with the decrease in systolic blood pressure in the OT im group (Rs=0.540, p=0.046).
Conclusion:
Administration of EDA during labor lowers baseline diastolic blood pressure and abolishes the fall in blood pressure in response to a breastfeed 2 days after birth.
Introduction
The neuropeptide oxytocin (OT), which is produced in the hypothalamus, was originally known to stimulate uterine contractions during labor and milk ejection during breastfeeding. 12 OT has, however, been shown to have a much broader pattern of effects. It has been demonstrated to induce maternal behavior and to facilitate bonding between mother and young in several types of mammalian species. 13 In addition, OT induces calm and antistress effects such as lowering of blood pressure and cortisol levels in rats through central mechanisms.14,15 Long-term antistress effects, including a decrease in blood pressure, are induced in response to repeated administration of OT. 16
Because OT exerts the effects described above, it is likely that the physiological and psychological adaptations observed in breastfeeding women are caused by the exposure to OT during breastfeeding.
Skin-to-skin contact between mother and infant before breastfeeding has been shown to induce maternal OT release 17 and to decrease the mothers' cortisol levels. 2 In addition, infants who are placed in skin-to-skin contact with their mother cry less, 18 display reduced heart rate, 19 and have an increased skin temperature. 20 Taken together, these data indicate that skin-to-skin contact in connection with breastfeeding stimulates interaction and induces calm in both mother and infant.
Experiments in sheep demonstrate that the release of OT into the brain and circulation is decreased by administration of a peridural anesthesia during labor and that the development of maternal behavior and attachment to the young is inhibited as a consequence of the lack of OT. 13
We have previously shown that medical interventions, such as epidural anesthesia (EDA) in order to relieve pain during labor, OT infusion (intravenously [iv]) in order to stimulate uterine contractions, and OT given intramuscularly (im) as an injection immediately after birth to prevent postpartum hemorrhage, influence the mothers' endogenous OT, prolactin, adrenocorticotropin hormone, and cortisol levels 2 days after birth2,21 as well as their psychological adaptation to breastfeeding. 9
It should be of clinical relevance to find out whether also the maternal blood pressure pattern observed in response to breastfeeding 2 days after birth is influenced by medical interventions such as EDA or OT given iv or im in connection with birth. In the present study we also wanted to investigate whether the duration of skin-to-skin contact affects the maternal blood pressure pattern. The investigation was performed on the same mothers as participated in the previous studies.2,9,21
Subjects and Methods
Inclusion criteria
The study was conducted at one of six maternity clinics located in Stockholm, Sweden, between January 2002 and December 2003. All eligible participants were consecutively informed about the study 10–24 hours following delivery by the same two midwives associated with the research team. The following inclusion criteria were applied for participation in the study: The mothers should not have smoked during the last 3 months before pregnancy or during pregnancy, have a prenatal body mass index less than 30 kg/m2, show no signs of hypertension during the pregnancy or birth, and should have had a normal vaginal delivery without complications for the mother or infant. Furthermore, the infant should have had an Apgar score of at least 8 at 1 minute after birth. The infant should not have been separated from the mother after the birth, not even for medical examination, and the infant should have been exclusively breastfed.
In total, 86 mothers fulfilled all inclusion criteria and were hence asked to participate and consecutively informed about the study. These mothers were admitted to the maternity ward on weekdays (Monday–Friday). Twenty of the mothers subsequently declined participation. Sixty-six mothers gave their informed consent to participate in the study.
Routine labor procedures
EDA is often used as pain relief during labor. The pharmaceuticals used in EDA are bupivacain and sufentanil, which may be either administered as a bolus dose (i.e., 25 mg of bupivacaine [2.5 mg/mL] and 10 μg of sufentanil [5 μg/mL]) or by continuous infusion (i.e., 45 mg of bupivacaine [5 mg/mL] and 50 μg of sufentanil [50 μg/mL] mixed with 34 mL of NaCl [9 mg/mL]). In the present study the EDA was administered by continuous infusion as long as necessary.
OT infusions are given to initiate or to augment labor. The infusion starts at a rate of 12 mL/hour and is increased by 12 mL each 30 minutes (10 IU/8.3 μg OT in 500 mL of Ringer's acetate).
OT is often given im after birth in order to stop bleeding. According to Swedish labor routines, all women giving birth should receive OT (10 IU) im to prevent postpartum bleeding. During this study period midwives were instructed not to administer OT im to the women fulfilling the inclusion criteria. However, some midwives did not comply with this instruction, and therefore some mothers did receive OT im postpartum. These mothers were included as a separate group (see below).
Study groups defined by medical interventions
The following groups were identified based on the medical interventions individual mothers had received during and after labor: Mothers who received neither OT stimulation or EDA during labor or OT im after birth (Control group, n=21); mothers who had received OT stimulation only during labor (OT iv group, n=9); mothers who had received 10 IU OT im after birth but no other treatment (OT im group, n=15); and mothers who had received EDA during labor (EDA group, n=21).
The latter group was divided into two groups for the purpose of a more detailed investigation of the effect of EDA with or without concomitant OT infusion: EDAOT group (n=14) and EDAnon-OT group (n=7).
Medical interventions of the eligible nonparticipants
Of the 20 mothers who declined participation in the study, 13 had received EDA, three had received OT iv, and four had received no medical intervention at all. The mothers declining participation in the study did not differ statistically from the participating mothers regarding maternal age, duration of pregnancy, and duration of first and second stage of labor and neonatal birth weight.
Routines at the maternity ward
Day- and night-rooming-in was practiced at the clinic where the study was conducted. The rooms were designed to create a friendly atmosphere giving an “at-home feeling.” The fathers or partners were present during the birth and the subsequent days at the maternity ward. Frequent breastfeeding and skin-to-skin contact between parents and newborns were encouraged. During the experiment the father and the two midwifes conducting the experiment were present in the room together with the mother and the infant.
Procedures during the breastfeeding experiment 2 days after birth
The experiments were performed on day 2 after birth, when the babies were between 24 and 48 hours old. The mothers were asked to call for the researchers as soon as the newborns started to show signs of wanting to breastfeed in the morning. The newborns, who were lying in the same bed as their mothers, were then placed in skin-to-skin contact on their mother's chest in order to initiate breastfeeding. The infants' legs and trunk were covered with a light blanket in order to keep them warm. The mothers were told to behave naturally and openly and that the researchers would not interfere. The mothers were permitted to ask the researchers to assist their breastfeeding if needed. Conversation was minimized during the observation period.
The infants initiated breastfeeding themselves. The mothers were asked to stay in the breastfeeding position for 60 minutes, irrespective of active breastfeeding or not.
Blood pressure recordings
Maternal systolic (SBP) and diastolic (DBP) blood pressures were measured by a blood pressure monitor (Omron R5-1 wrist blood pressure monitor, Omron Healthcare, Hoofddorp, The Netherlands), which was attached to the mother's right wrist after the mother had been lying in the supine position for an initial resting period of at least 10 minutes. Blood pressure was measured 5 minutes before infants were placed skin-to-skin with their mothers (baseline blood pressure); subsequent measurements were performed at 10, 30, and 60 minutes after breastfeeding had been initiated.
Data analysis
The data were analyzed using the software Statistical Package for the Social Sciences (SPSS/PASW) version 17.0 (2009) (SPSS Inc., Chicago, IL). Because the number of participants in each group were relatively small and a normal distribution could not be taken for granted, nonparametric tests were used throughout the study. Clinical background data were described by medians and interquartile distances (Q25 – Q75). In order to test differences in background data between the groups, the Kruskal–Wallis test for independent samples was performed.
Data on blood pressure (SBP and DBP) were described by means and SDs.
Mann–Whitney U tests were performed for all five subgroups to test for differences in baseline SBP and DBP.
Wilcoxon signed rank tests were performed for all five subgroups in order to test changes between baseline SBP and SBP at 60 minutes as well as baseline DBP and DBP at 60 minutes.
Furthermore, the difference between baseline SBP and SBP obtained at 60 minutes was calculated (ΔSBP). The same procedure was also performed for DBP (ΔDBP).
Spearman's correlation coefficients were calculated between ΔSBP and between ΔDBP with the time mother and infant spent in skin-to-skin contact before initiation of suckling.
Ethical consent
The ethical committee at the Karolinska Institutet, Stockholm, Sweden, approved the study.
Results
Clinical background data
Clinical background data on mothers, newborns, and breastfeeding are given in Table 1. There were no differences among the groups in any of the variables described.
Data are medians [interquartile distances (Q25 – Q75)].
EDA, epidural anesthesia; im, intramuscularly; iv, intravenously; OT, oxytocin.
Blood pressure during breastfeeding 2 days postpartum
Mean SBP and DBP obtained at each time point for the five study groups during the breastfeeding session 2 days postpartum are presented in Table 2 and in Figures 1 and 2.
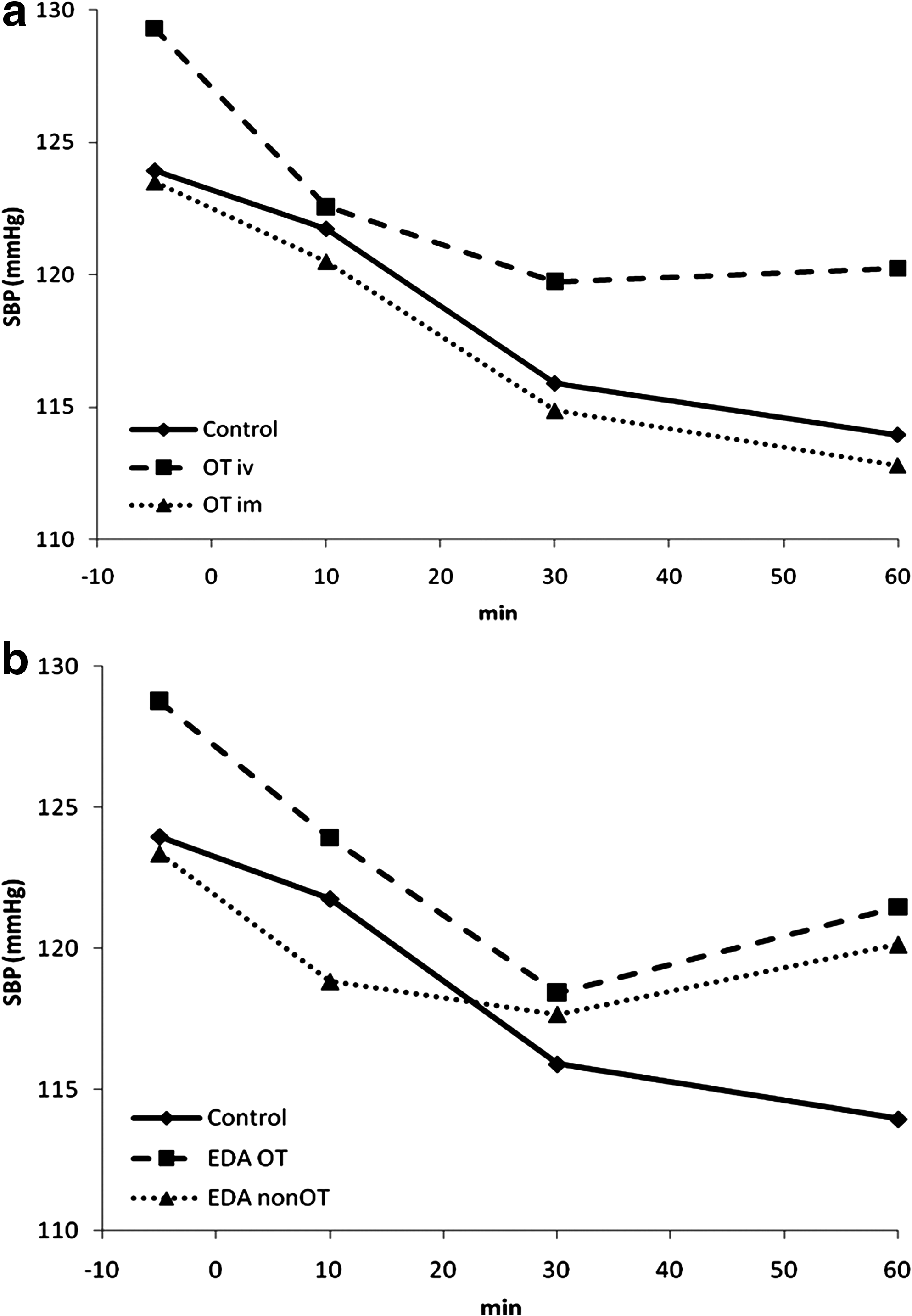
SBP (in mm Hg) in
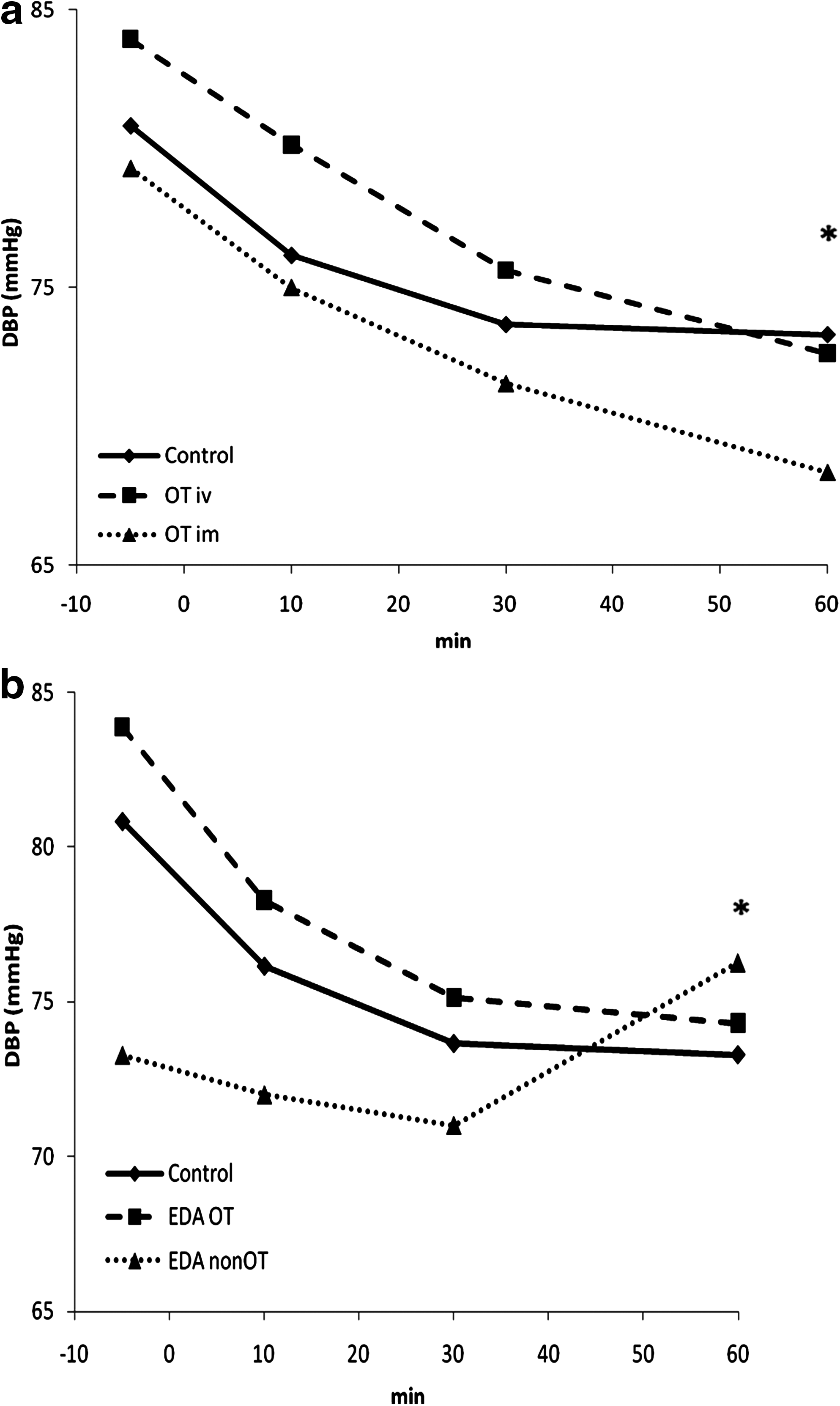
DBP (in mm Hg) in
Data are mean (SD) values (in mm Hg).
DBP, diastolic blood pressure; SBP, systolic blood pressure.
Decrease in blood pressure
Both SBP and DBP decreased significantly in the control group, the OT im group, and the EDAOT group, and DBP approached a significant decrease in the OT iv group during breastfeeding. By contrast, no decrease in either SBP or DBP was seen in the EDAnon-OT group (for p values for each group, see Table 3).
Blood pressure data are mean (SD) values (in mm Hg). The p values based on Wilcoxon signed rank tests are presented.
Baseline blood pressure
Baseline SBP before breastfeeding did not differ significantly between the different study groups (p=0.849).
In contrast, baseline DBP was significantly lower in the EDAnon-OT group compared with the baseline DBP in the Control group, the OT iv group, and the EDAOT group (p=0.023, p=0.014, and p=0.011, respectively). However, there was no significant difference in baseline DBP between the EDAnon-OT group and the OT im group (p=0.102).
Correlations between duration of skin-to-skin contact before breastfeeding and decrease in SBP and DBP
In the OT im group, the duration of skin-to-skin contact before breastfeeding was positively correlated to the fall in SBP occurring during the 60 minutes of breastfeeding (Rs=0.540, p=0.046). Thus, the longer the newborns were lying in skin-to-skin contact with their mothers before initiation of suckling, the more the maternal SBP decreased during the breastfeeding session 2 days later.
No such relationships were found in the other groups.
Discussion
The main findings of the present study were that both SBP and DBP decreased significantly, or approached a significant decrease, during the breastfeeding session in all groups except for the EDAnon-OT group. In addition, the same mothers (EDAnon-OT group) had significantly lower baseline DBP compared with the Control group, the OT iv group, and the EDAOT group; however, other factors were not accounted for.
Women who breastfeed display a decrease in blood pressure during the actual breastfeeding session.3,4 We have previously shown that medical interventions given during labor, such as EDA and OT infusion, influence the mothers' release pattern of endogenous oxytocin, prolactin, adrenocorticotropin hormone, and cortisol levels in connection with breastfeeding 2 days after birth.2,21 In the present study we wanted to investigate if the same interventions also affect the pattern of maternal blood pressure in response to breastfeeding 2 days after birth.
During breastfeeding the neuropeptide OT is released into the circulation in response to the infants' suckling. The circulating OT activates the receptors in the myoepithelial cells of the mammary glands to cause milk ejection. In parallel, there is a release of OT in the brain from oxytocinergic nerves originating in the paraventricular nucleus. The nerves project to important regulatory centers in the brain, including areas in the hypothalamus and the brain stem that are of importance for control of cardiovascular function, for example, the nucleus tractus solitarius and the dorsal vagal motor complex. 12
Data from animal experiments show that administration of OT decreases blood pressure, probably via activation of α2-adrenoreceptors in the nucleus tractus solitarius and adjacent areas in the brain stem. 22 It is therefore likely that the decrease in maternal blood pressure observed during breastfeeding is caused by OT released into the brain in response to the suckling stimulus.
The data from the present study show that blood pressure was not decreased in response to breastfeeding in mothers having received EDA alone (EDAnon-OT group). The reason why breastfeeding did not lower blood pressure in these mothers is probably due to their lower baseline blood pressure, which does not allow further decrease.
One reason behind the low baseline blood pressure in the EDAnon-OT group might be that the decrease of blood pressure induced by the EDA during labor is sustained. The two pharmacological constituents of EDA—bupivacain and sufentanil—exert additive effects on the decrease of blood pressure.
An alternative explanation might be that the baseline blood pressure 2 days after birth is related to maternal endogenous OT secretion in the brain. High levels of OT result in a decrease in sympathetic vasoconstriction and consequently a decrease in DBP.
Mothers having received EDA combined with OT (EDAOT group) displayed higher baseline blood pressure compared with mothers having received an EDA alone (EDAnon-OT group). We have previously shown that the mothers in the EDAOT group have significantly lower circulating OT levels and higher cortisol levels during a breastfeeding session 2 days after birth, compared with the mothers in the EDAnon-OT group.2,21 Taken together, these findings might suggest that the mothers who received EDA with or without OT infusion during labor have a decreased or increased activity, respectively, in their endogenous OT secretion, both into the circulation and into areas in the brain.
The activity in the central OT system in turn influences their cortisol and blood pressure—high OT secretion being linked to lower cortisol levels and blood pressure and low OT secretion to higher cortisol levels and blood pressure. These differential effects on endogenous OT secretion might have been induced by the EDA with or without OT during labor. 21
Also, other studies indicate a relationship between OT levels and low blood pressure: The higher the OT levels, the lower the blood pressure. 23
In our study DBP was more affected than SBP. In previous studies similar differential effect on DBP have shown to be associated with OT administration.24,25
For the mothers in the OT im group there was a positive correlation between the duration of skin-to-skin contact before the onset of suckling and the decrease in SBP during the 60-minute observation period.
When infants are lying in skin-to-skin contact on their mothers' chest, they stimulate maternal OT release by massage-like movements with their hands. 17 Longer duration of skin-to-skin contact before suckling has also been shown to reduce mothers' cortisol levels during the breastfeeding session. 2 The results from the present study suggest that the OT released from the presuckling period due to the skin-to-skin contact also contributed to the decrease in blood pressure observed during the breastfeeding session in the mothers in the OT im group. The reason for seeing the effects only in the OT im group may be related to the fact that OT im administration gives rise to temporarily very high levels of OT, which may exert effects different from those exerted by OT iv administration.
The number of participants in the present study is small. However, because the inclusion criteria were strict and procedures were standardized, we believe that important information can be obtained from the present study, as has been the case in other studies performed under similar conditions.26–28
In order to better understand the effect on breastfeeding related decrease in blood pressure by skin-to-skin contact and by medical interventions such as EDA and OT infusions, further detailed controlled studies with a larger number of participants need to be performed.
Conclusion
The results from the present study suggest that EDA, as well as OT infusion, given during labor may exert effects on the maternal blood pressure pattern in response to breastfeeding 2 days after delivery. In addition, the duration of skin-to-skin contact before the onset of suckling may play a role in reducing maternal blood pressure during breastfeeding.
Footnotes
Acknowledgments
The authors would like to thank all mothers and babies for participating in this study, the staff at BB Stockholm, and Ingela Wiklund for participating in collection of data. The authors would also like to thank Strategic Research Programme in Care Sciences for financial support.
Disclosure Statement
No competing financial interests exist.