
Abstract
Abstract
The value of breastfeeding for mothers, babies, and society is well established, yet in the United States too many women do not breastfeed. The U.S. Public Health Service set forth breastfeeding goals for 2010 and subsequently developed report cards so that breastfeeding trends could be followed for each state. Many efforts are made by healthcare professionals to encourage and support new mothers, but some areas in the United States have low levels of breastfeeding. This report examines aspects of obstetricians' education, role, and responsibility to promote and support breastfeeding. Additionally, some current trends affecting the practice of breastfeeding are considered, including shorter hospital stays, rapidly rising cesarean delivery rates (soon to approach 50%), and increasing proportion of working mothers. Because obstetricians often have the first contact with expectant mothers and there are over 20 million prenatal visits annually in the United States, obstetricians have many opportunities to promote breastfeeding. Together with the efforts of other physicians, nurses, and lactation specialists, we can improve the efforts to promote and support breastfeeding.
Introduction
The second colleague, a dedicated scholar whose opinions are respected worldwide, is Ruth Lawrence, Professor of Pediatrics and Obstetrics at the University of Rochester, Rochester, NY. A leader who has relentlessly led the effort to make breastfeeding the standard for all mothers, Ruth is a pioneer in toxicology and neonatology. Her book on breastfeeding, coauthored with her son Robert, is the standard for breastfeeding throughout the world. I salute these two members of the Academy of Breastfeeding Medicine and thank them for their leadership and tutelage.
My interest in breastfeeding as a public health measure stems from a talk by Margaret Heckler, Secretary of the U.S. Department of Health and Human Services from 1983 to 1985, outlining the goals of Healthy People 1990. She emphasized the public health benefits of breastfeeding and its extraordinary value for people while incurring little or no cost. I remember being impressed by her commonsense approach to the many measures that can be implemented such as exercise, diet, and avoiding tobacco. Each step requires individual effort, and yet it is the individual who benefits, at essentially no cost to the public. In this era of spiraling expenditures for medical care, this approach is practical and productive for our national health.
Benefits of Breastfeeding
It is always appropriate to reiterate the public health benefits of breastfeeding, and even though they are well established, breastfeeding is underutilized. For this article, simply listing these benefits should suffice.1,2 Advantages for the baby include:
Species-specific and age-specific nutrients Immunologic protection Infection protection Changes composition to meet the infant's need Biologic signals Allergy prophylaxis Psychological and cognitive benefits
While all of these benefits are well established, in my judgment, the immunologic and anti-infection properties are the most compelling when discussing benefits with a woman making a decision about feeding her baby.
Benefits of breastfeeding for the mother include:
Psychological Enhancing postpartum recovery Facilitating return to the prepregnancy state Decreasing the risk of developing ovarian and breast cancer Lowering the incidence of osteoporosis and hip fracture after menopause
When discussing maternal values of breastfeeding with a expectant mother, emphasizing a decreased risk of developing ovarian and breast cancer and a lower incidence of osteoporosis and hip fracture after menopause, even though remote, can be compelling selling points.
Benefits of breastfeeding for society include:
Fewer illnesses and fewer visits to the physician Lower medical expenses Less absenteeism from work Lower costs for families and public programs Ecological issues—disposal of cans, bottles, and liners
In these days of heightened social and economic concern each of these benefits is important. However, it would appear that the prospects of fewer illnesses and fewer visits to physicians would result in lower medical expenses, and should prove convincing and appealing to any prospective mother.
Areas of High and Low Breastfeeding
Based on information such as the advantages listed above, the U.S. Public Health Service set forth breastfeeding goals in Healthy People 2010:
3
75% of mothers initiating breastfeeding 50% breastfeeding at 6 months 25% breastfeeding at 12 months 40% exclusively breastfeeding at 3 months 17% exclusively breastfeeding at 6 months
Since 2002 the Centers for Disease Control and Prevention (CDC) has been tracking the trends of breastfeeding in the United States. Breastfeeding monitoring has been included in the immunization surveillance so that it is a comprehensive national evaluation. The CDC provides report cards on breastfeeding outcome indicators on a state by state basis. The most recent CDC report cards list the preliminary data for 2007. For the percentage of infants ever breastfeeding, a broad brushstroke would indicate the West Coast, the western states, along with Hawaii and Alaska, New York, the New England states, and Virginia reached the goal of greater than 75% ever breastfeeding. Overall, three out of every four new mothers in the United States start out breastfeeding, which means that the United States has met the 2010 objectives for breastfeeding initiation.
Figure 1 shows the 2007 success rate of the Healthy People 2010 goal of 75% of children breastfed, with only 24 states achieving the 2010 goals. 3
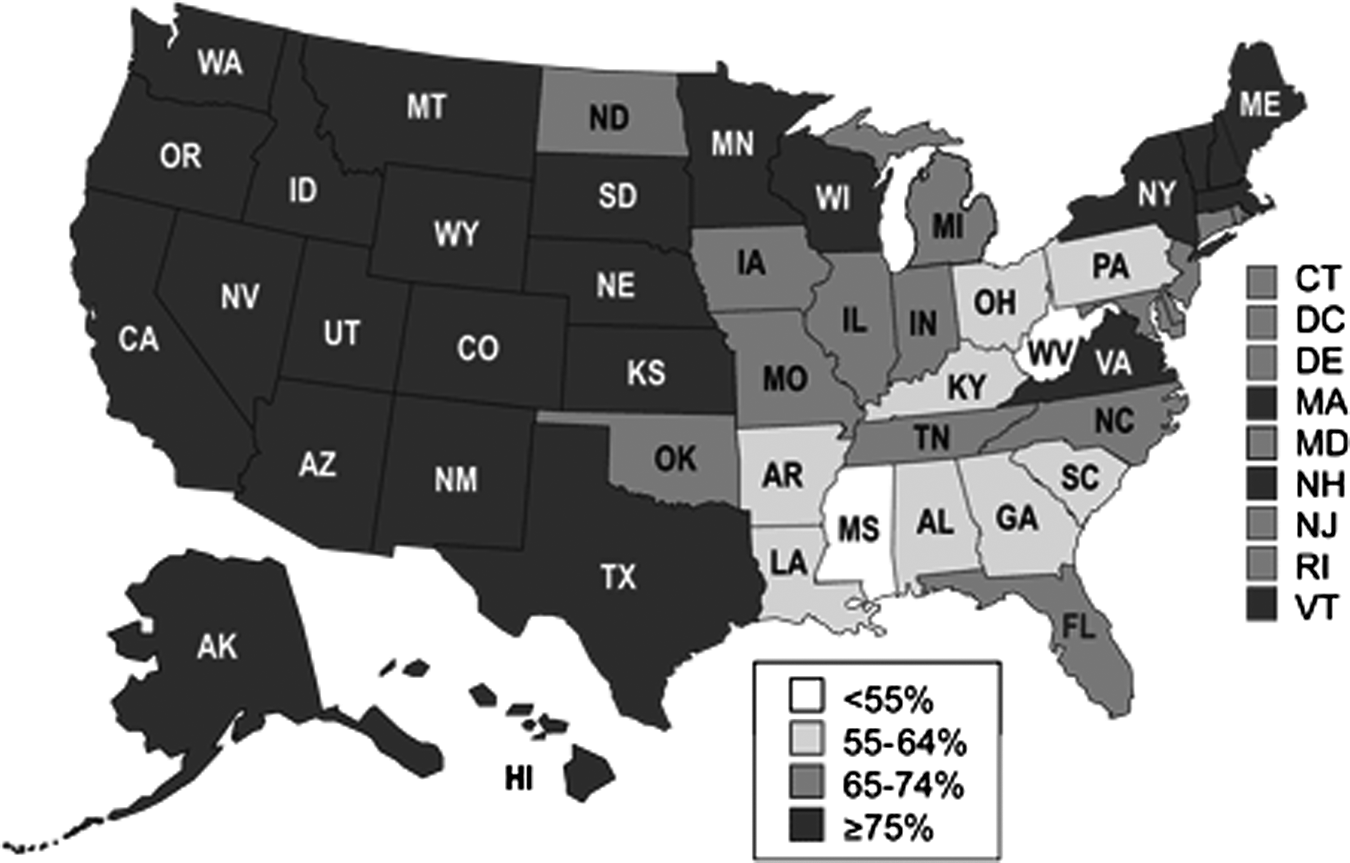
Percentage of children ever breastfed, 2007. 3
For the percentage of breastfeeding mothers reaching the goal of 50% at 6 months in 2007, again, Hawaii, Alaska, the West Coast and some of the western states, and Minnesota plus Vermont, New Hampshire, and Massachusetts achieved this level 3 (Fig. 2).
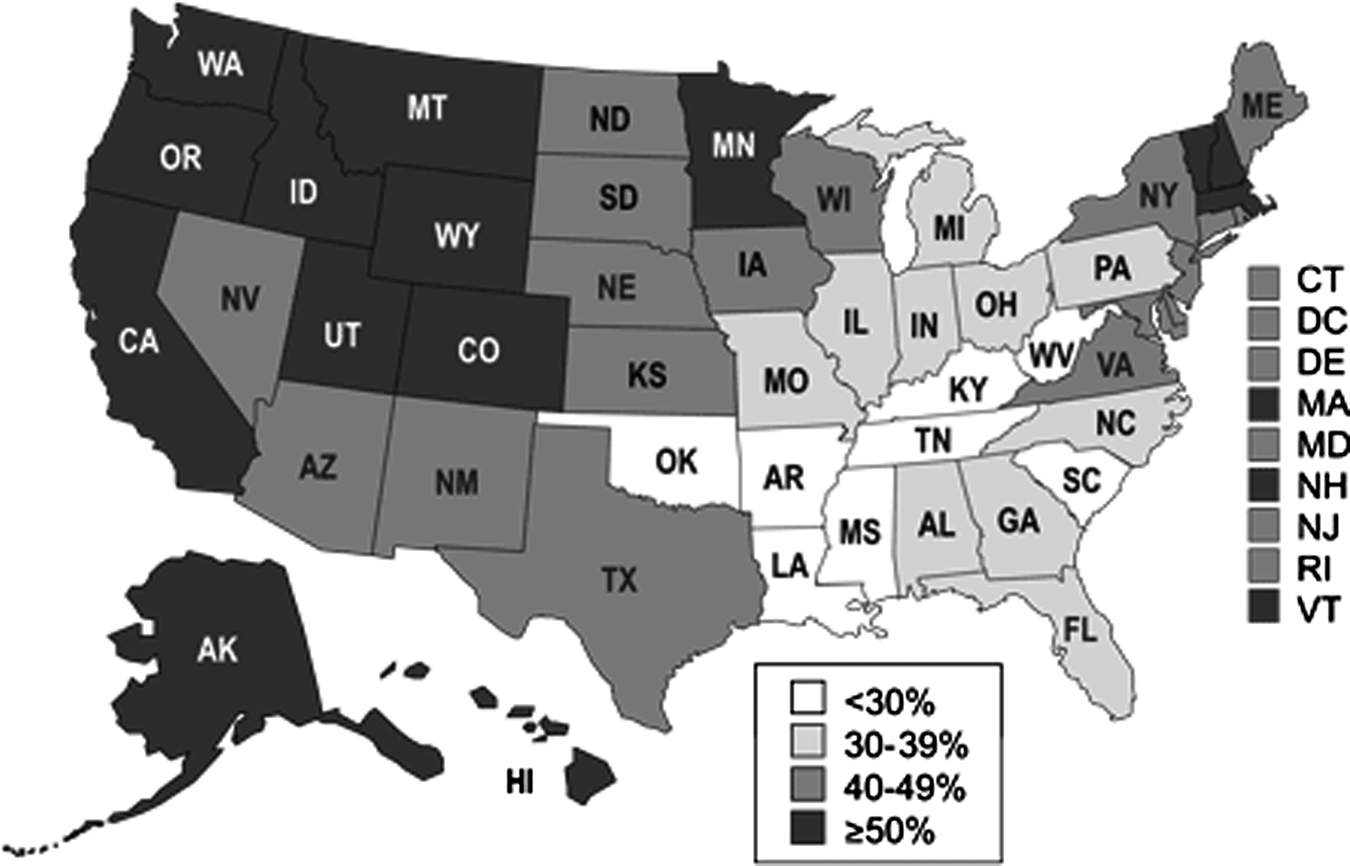
Percentage of children who are breastfed at 6 months, 2007. 3
For the percentage of breastfeeding mothers achieving the goal of 25% at 12 months in 2007, again, Hawaii, Alaska, the West Coast and some of the West, Minnesota, plus Vermont, New Hampshire, and Maine, or 15 states, achieved the goal 3 (Fig. 3).
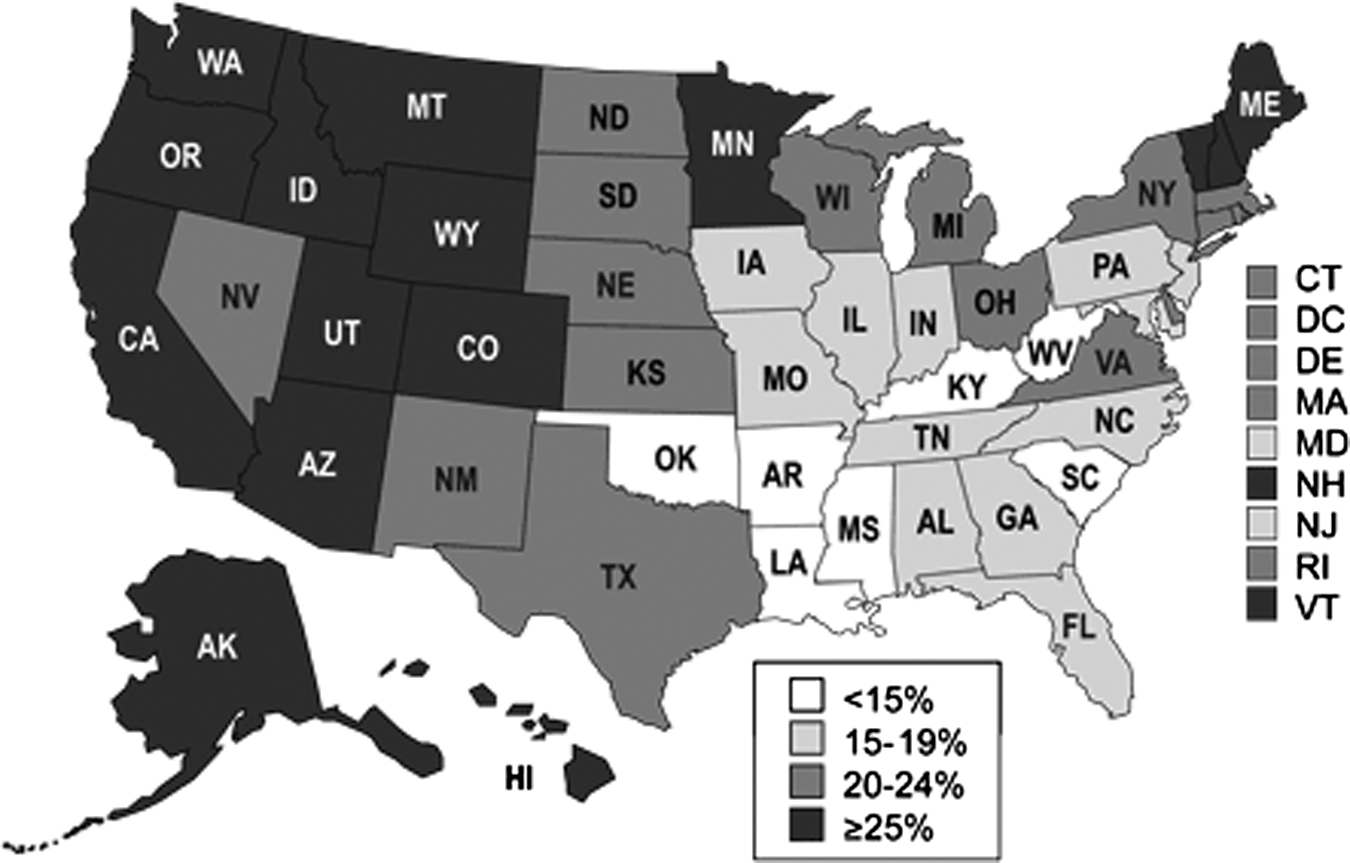
Percentage of children breastfed at 12 months. 3
For exclusive breastfeeding by 40% or more of mothers at 3 months, Alaska, Hawaii, the West Coast and many of the western states, Minnesota, Maine, New Hampshire, and Vermont achieved the goal. At 6 months, 15 states achieved the goal of 17% or more of mothers exclusively breastfeeding; the states were Alaska, the West Coast, some western states, Minnesota, and the New England states.
It appears that U.S. women want to breastfeed with 75% initiating, but there is a significant dropoff by 3, 6, and 12 months of breastfeeding and exclusive breastfeeding. One can conclude that there is a clear geographic pattern and most likely a lack of support and certain obstacles, i.e., the 20% of breastfeeding infants who are fed formula in the hospital by well-meaning but ill-informed nurses.
Recently, I had the honor of giving a lecture at the American College of Obstetricians and Gynecologists' District IV Fall Meeting in Savannah, GA. It was an opportunity to demonstrate how these report cards can be used as a guide to how well we are doing in achieving the national goals in an area. As an example, District IV had five states whose report cards showed they were below the national average on all indicators, whereas Virginia, Maryland, and the District of Columbia exceeded national averages by at least one indicator (Table 1). 3
Data were obtained from the Centers for Disease Control and Prevention. 3
Obstacles to Breastfeeding
There are many obstacles to successful breastfeeding, which include inadequate instruction, poor support, and lack of workplace accommodations. Some of the obstacles are under physicians' direct control. For example, well-intentioned obstetricians may tell their rooming-in patients that if they are too tired after delivery they may send their newborns to the nursery “so they can get a good night's sleep.” Thus the mother misses her best opportunity for help and supervision with a fussy baby in the middle of the night. The next morning she is discharged and on her own. Another example is the well-meaning nurse with the breastfeeding newborn who is hungry and fussy in the nursery and feeds the baby formula. It is unfortunate that 25% of breastfeeding babies are fed formula before discharge. 4 Other barriers to successful breastfeeding can be found in ethnic and racial groups where early introduction of solids (West Coast Hispanics) can decrease the success of breastfeeding. The Healthy People 2020 objectives will address barriers including evaluation of maternity practices and worksite support.
In a recent report racial and ethnic difference in breastfeeding were described for 2004–2008. 5 Non-Hispanic blacks had lower levels of breastfeeding than non-Hispanic whites in 48 of 50 states. Hispanics had lower prevalence than non-Hispanic whites in western states, but higher in eastern states and overall. Most states were not meeting the Healthy People 2010 targets in any ethnic group. 5
Role of Obstetricians in Promotion and Support of Breastfeeding
Because the obstetrician often has the first contact with the expectant mother, there is a unique and critical opportunity to influence her choice to breastfeed. It stands to reason that the approach of the obstetricians and their office and clinic staff have an enormous influence on the mothers' final choice. Accepting the premise that breastfeeding is the best choice, it follows that appropriate instruction, promotion, and support are needed to assure prospective mothers that this is the preferable and doable choice for them.
Perhaps one of the most important influences of the obstetricians' approach to breastfeeding comes from his or her education and training. A review of obstetric textbooks shows a wide variety of breastfeeding information, content, and quality (Table 2). For instance, in two widely used textbooks, the one edited by Gabbe et al. 6 has 28 pages by Dr. Edward Newton, a member of the Academy of Breastfeeding Medicine, devoted to breastfeeding, whereas Williams Obstetrics, edited by Cunningham et al., 7 has 6 pages. Management of High-Risk Pregnancy by Queenan et al. 8 has 6 pages by Newton and Faranoff. The 5th edition of Maternal-Fetal Medicine by Creasy et al. 9 has 18 pages by Ruth and Robert Lawrence, and Protocols for High-Risk Pregnancy edited by Queenan et al. 10 has 7 pages by Hansen and Rosenberg. Of note is the chapter by the Lawrences in Creasy et al., 9 which covers anatomy, physiology, initiation of lactation, and the practical aspects necessary for lactation management. In my view, this is the gold standard.
Residency Curriculum
The residency curriculum is guided by the Council on Residency Education in Obstetrics and Gynecology educational objectives set forth in the 2009 (9th edition) of the Core Curriculum (accessible to members at www.acog.org/departments/dept_web.cfm?recno=1). While the objectives require counseling on the benefits of breastfeeding, they do not list initiation or physiology of lactation, which, of course, is the basic knowledge one needs when making decisions on family planning and breastfeeding in general. They require education in diagnosis and treatment of benign breast disorders, breast engorgement, and mastitis. The extent of the curriculum is limited, and the content is essentially pathology-oriented. Additional areas need to be covered, e.g., physiology of lactation and common problems of lactation.
While textbooks and residency curriculum are important, inclusion of questions on breastfeeding in certification examinations is critical. When one is learning a specialty or preparing for an examination, knowing that questions on a subject will appear on the certification exam is the ultimate motivating factor for learning. The American Board of Obstetrics and Gynecology certification requires a written followed by an oral examination. Maintenance of certification, started in 1986, is a critical part of the ongoing certification process. A discussion (at the American College of Obstetricians and Gynecologists' Annual Clinical Meeting, May 16, 2010) with the directors, Drs. Larry Gilstrap and Kenneth Noller (personal communication), assured me that both exams contain breastfeeding questions.
On balance, it appears that obstetricians get average education and training in breastfeeding, but improvement should be made in the areas of the physiology of lactation and practical aspects of breastfeeding.
Survey of Obstetrical Breastfeeding Support
In view of the Healthy People 2010 goals, it appears that obstetricians are a major factor in the achievement of the breastfeeding objectives. While my distinct impression is that almost all obstetricians would answer that breastfeeding is the preferred way of feeding a baby, it seems likely that different levels of support exist. To that end, a survey of obstetricians was developed. Twenty questions were directed at the level of interest of performance and level of breastfeeding. This was administered to obstetricians according to standard sampling technique for all states in the United States. The survey is almost complete. The data will be broken into four tiers, looking at the top and bottom tiers. A comparison with Healthy People 2010 indicators will be made with the intent of finding where and how to increase promotion and support.
Current Trends Affecting Breastfeeding
Obstetrics is a dynamic specialty with many social, financial, and scientific factors affecting the discipline. Scientific advances as sonography, rubella immunization, and Rh-immune prophylaxis have brought about positive effects for mothers and infants. However, many social and financial trends are resulting in negative effects. Therefore, the healthcare team must continually seek solutions to the changing landscape of practice. 11
In 2006, 4.2 million deliveries occurred in a hospital, whereas 38,568 deliveries occurred outside hospitals, including freestanding birthing centers, clinics, homes, or other. Because greater than 99% of deliveries are in hospitals, the following discussions will concern only patients who are planning hospital deliveries. 11
Decreasing length of stay
In the 1960s and 1970s the hospital stay for primiparas was 7 days, and that for multiparas was 5 days. Today the hospital stay for uncomplicated deliveries is limited to 1 day postpartum. If the mother delivers before midnight, she is discharged the next morning. While such a radical change in hospital utilization was initially thought to be severe and nearly impossible to achieve, over the years, the medical community has adjusted to this necessity. Unlike in the past, when breastfeeding instruction, observation, and supervision were possible postpartum, today these measures are limited. Accordingly, much of the preparation and education must be provided during the antepartum period. The instruction and breastfeeding supervision require efficient and effective use of time in the hospital. While these changes have been an economic necessity, this is an example of a current trend that has required ingenuity and coping to create a pleasant and successful stay for a patient.
Rising cesarean delivery rate
The cesarean delivery rate has been rising with no signs of abatement. In 1970 the cesarean rate was 5.5%. It rose to 16.5% by 1980, reaching 22.9% in 2000. Since 2000 the rate has continued to creep upward to the point where it reached 32.3% in 2008. Recent data indicate that one-third of cesarean deliveries are in primigravidas. 12 This signals that in the near future the rate may reach 50%. 11
Non-emergency cesarean deliveries, while generally safe today, carry a significant increase in future morbidity and mortality due to rises in the incidence of placental complications (placenta accreta, abruption, etc.) and uterine rupture in a setting of increasing the cost of care. Vaginal birth after cesarean delivery is one means to curtail the rising cesarean rate but because of numerous factors has almost disappeared as an option. Hospital administrators tend to resist vaginal birth after cesarean delivery as professional liability costs escalate and hospital reimbursement is considerably higher for cesarean than vaginal births. Some patients are concerned about going through long labors with the possibility of having to undergo another cesarean. Some obstetricians may prefer a scheduled 30–45-minute session in the operating room to the uncertainties of a laboring patient with a uterine scar. Thus, there is a serious need to curtail the number of cesareans in primigravidas as a means of decreasing the overall rate.
The rising rate of cesarean deliveries also has an unfavorable impact on the breastfeeding experience. There is commonly separation and delay in the holding and bonding of the newborn. Our clinical challenge now is to recreate the way we conduct a cesarean delivery so that it is more conducive to bonding while remaining safe. Numerous attempts have been helpful, but we have only begun to explore ideal practices. One such attempt is a launching point for ways to improve the cesarean experience. This is called “the natural cesarean delivery.” 13 While this technique is bold and certainly unproven, it does present examples of what can be explored. Any modifications of accepted practice must be considered experimental and be scientifically studied to evaluate safety.
Preparation for “natural cesarean delivery” includes administering spinal/epidural anesthesia with needle through needle, with bupivacaine, placing the pulse oximeter on a toe, placing the electrocardiogram leads on the lateral chest, and utilizing the non-dominant arm for the intravenous line.
The top of the operating table is raised, and the ether screen is temporarily lowered so the mother and father can observe as the baby emerges, which occurs over approximately 3 minutes while the baby is still supported by a functioning placenta and umbilical cord. The baby's head is allowed to remain in the incision to encourage drainage of fluids from the nostrils as a result of external compression of the uterus and maternal soft tissues as observed in Figure 4. The parents observe the emergence of their baby through cesarean incision (Fig. 5). In Figure 6, the baby's trunk is eased out by a combination of uterine contractions and gentle pressure by the obstetrician to assure his or her face is toward the parents. The baby's well-being is monitored by observing crying and facial reactions. The uterine incision to delivery time is prolonged compared with normal procedures, but usually is within 3 minutes.

The baby's head is allowed to remain in the incision to encourage drainage of fluids from the nostrils as a result of external compression of the uterus and maternal soft tissues. Reprinted with permission from from Smith et al. 13

The parents observe the emergence of their baby through cesarean incision. Reprinted with permission from from Smith et al. 13

The baby's trunk is eased out by a combination of uterine contractions and gentle pressure by the obstetrician to assure the baby's face is toward the parents. Reprinted with permission from Smith et al. 13
The baby is handed to the midwife, who is standing directly alongside the mother's head. Skin-to-skin contact is established within a minute of the completion of the (3-minute) delivery. The ether screen is raised while the surgical closure is completed. The baby is kept warm with towels and bubble wrap.
“The natural cesarean delivery” can be broken down into five separate areas for evaluation:
Viewing and emergence of the delivery—evaluate the desirability of direct viewing; test mirror versus direct view. Incision compression of the head—evaluate the effect on the infant. “Walking out”—probably the least appealing or practical to my mind, with major issues that need to be evaluated such as the likelihood of hypothermia, effectiveness of respiratory drainage, and assessment of the infant's condition. Giving the baby to the mother during closure—this is already in practice in varying degrees in the United States, but generally after initial newborn evaluation and Apgar scores are completed. Practicality. What changes or innovations are appropriate and practical in various hospital settings? For example, if a hospital has a very high volume of cesareans, some immediate bonding and skin-to-skin contact might have to occur in the recovery room. In hospitals where there is more time to have the patient remain in the operating/delivery room, placing the baby on the chest for skin-to-skin contact and early breastfeeding could be very feasible.
11
In some hospitals in the United States the baby is given to the mother as soon as the 5-minute Apgar is performed.
Increasing proportion of working mothers
Over 60% of new mothers are in the workforce. Assuring that the mother gets adequate time to get acclimated to her child and the rhythm of breastfeeding should be major concerns of both obstetricians and pediatricians. Management of breastfeeding must include a return-to-work plan. While most of this is in the province of the pediatrician, the obstetrician must be supportive and informed.
Improving conditions for the working mother must be an ongoing mission of all physicians involved in delivery and infant care. The survey by the National Conference of State Legislatures in 2009 14 indicates the states in which there are mandates for both employer lactation support and support for breastfeeding in public (Fig. 7) versus states only mandating support for breastfeeding in public. The two states with no breastfeeding legislation are Idaho and Nebraska.
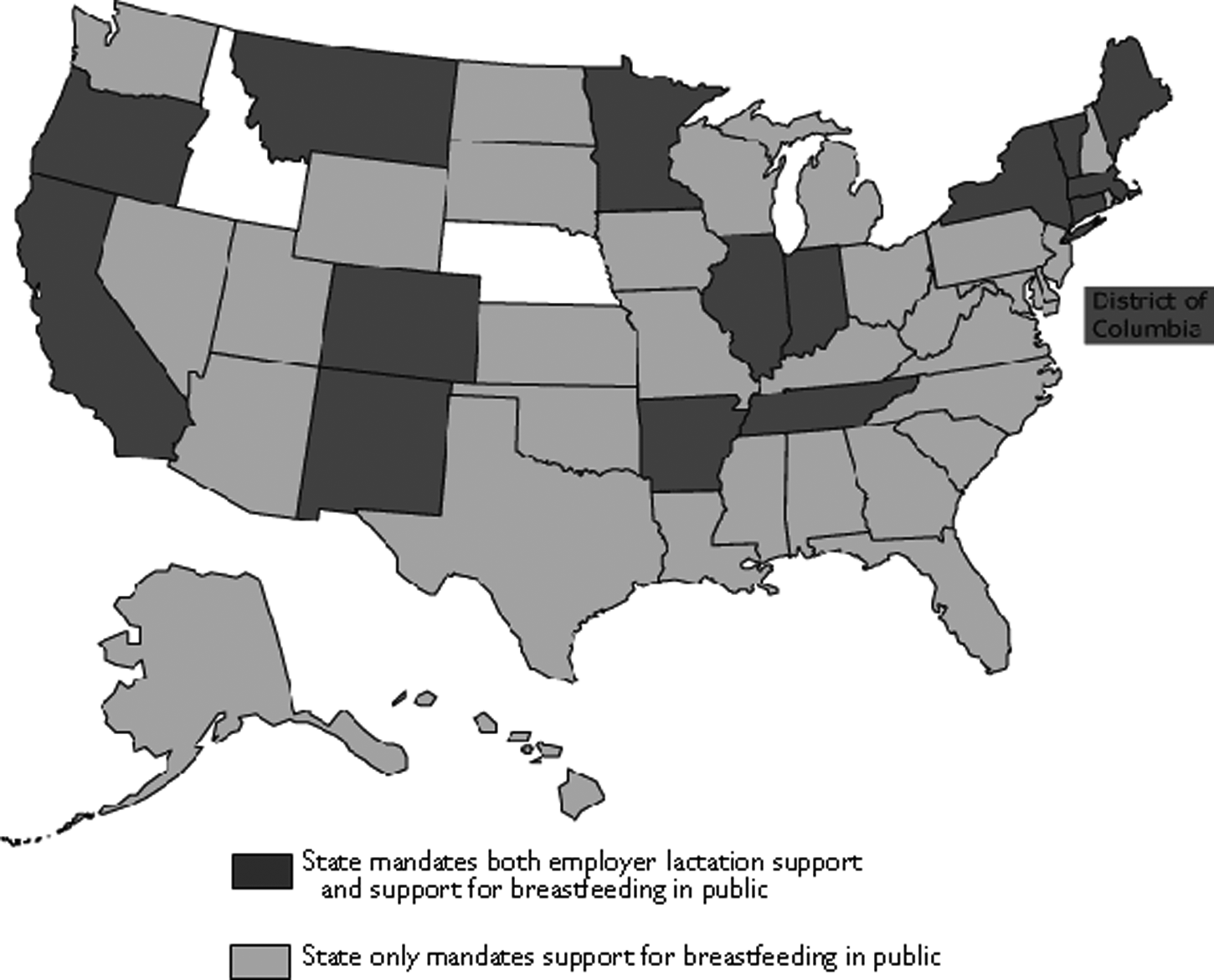
Legislative support for breastfeeding in public and/or employer lactation support according to the National Conference of State Legislatures in 2009. 14
Increasing delivery of care by groups
While the solo practitioner is becoming a rarity, the loss of one's “personal physician” can have compensations. Practicing by physicians in teams or groups, when done properly, can be very rewarding to patients and physicians. For instance, in areas of physician coverage, protocol development, and consultations, clearly the physicians in group practices have advantages. Concerning patient education and programs (breastfeeding), practicing in groups can provide a distinct advantage in the development of resources for patient education programs.
Increasing age at delivery (2006)
The birth rate for women 40–44 years old was 9.4 births per 1,000 women, the highest for this group since 1968. Women 44–49 years old had 105,529 live births, a record high for the United States, with nearly 25% of these were first births for mothers. 11 The older mother is commonly a professional woman who has delayed her child-bearing. While older mothers run a higher risk of chromosomal abnormalities, once the absence of that problem is confirmed, the other potential health problems are offset by the sheer delight of having a baby. In my experience, their willingness to follow whatever advice that ensures them of having a healthy baby is exemplary. They have an excellent record of breastfeeding.
Opportunities to Promote Breastfeeding
Each patient visit can be an opportunity to promote and reinforce the value of breastfeeding. According to the National Center for Health Statistics, there were over 25 million obstetrics-gynecology visits in 2006: Routine prenatal exams constituted almost 20 million office visits, postpartum exams 2,379,024, and general medical exams another 1.7 million. 11 Because any visit related to pregnancy is an opportunity to reinforce the value of breastfeeding, it should be part of our mission to use these visits to educate and promote the value of breastfeeding.
Physician's role
From my perspective, we all must work together, but there are certain areas of responsibility that are generally best done by specific professionals.
The obstetrician's role
Promote and support breastfeeding
Support and assure initiation of breastfeeding
Better utilize the patient contact opportunities and lactation support professionals
The pediatrician's role
Promote and support breastfeeding
Support and assure initiation of breastfeeding
Assure continuation of breastfeeding
One of my major concerns is weaning some physicians from formula company financial support. Too many babies area given formula on their first day in the hospital, and this is a matter that is under the control of physicians.
Closing Comments
We need major efforts directed to the cesarean delivery challenge. Special effort is necessary to support the working mother. Exclusive breastfeeding is important, but breastfeeding for all is critical. A major effort in encouraging nearly 100% of mothers to initiate breastfeeding will pay major health dividends. Finally, we need to recruit more young obstetricians to the Academy. We have come a long way through the dedicated work of many, but major challenges lie ahead. I am confident the Academy of Breastfeeding Medicine can and will meet these challenges.
Footnotes
Disclosure Statement
No competing financial interests exist.