RowanMarnieMBBS1*DeaconJaneMBBS1GarbinCathy1McClellanHollyB.Sc.1WatsonMichaelMBBS, DTM&H, MPH23HepworthAnnaB.Sc.1GeddesDonnaPh.D.1HartmannPeterPh.D.1
School of Biomedical, Biomolecular, and Chemical Sciences, The University of Western Australia, Crawley, WA, Australia
Clinipath Pathology, Perth, WA, Australia
School of Medicine, University of Notre Dame, Freemantle, WA, Australia
1. Persistent Nipple Pain—Is Staphylococcus Aureus the Cause?
Background: Sore nipples, with or without visible damage, remain a commonly cited maternal reason for early weaning.
Objective: Determine the incidence of Staphylococcus aureus in breastfeeding mothers with persistent nipple pain.
Methods: Breastfeeding dyads (n = 90) were recruited to three groups: controls, mothers with no pain; minimal trauma, mothers with pain and minimal nipple trauma; or obvious trauma, mothers with pain and obvious nipple trauma. Swabs were taken from one nipple and the noses of both mother and baby, and a breastmilk sample was obtained. Samples were cultured using selective media. Rates of carriage were compared for the three groups, taking into account infant age. Significance was p < 0.05.
Results: Both pain groups had significantly higher rates of positive nipple and milk cultures than the controls, with highest rates in the obvious trauma group. The milk results were similar. No differences were seen between controls and pain groups in rates of nasal carriage. All dyads where there was a positive nipple or milk had at least one positive nose result. Of the mothers with positive nipple and/or milk cultures, 93% and 96%, respectively, had positive baby nose cultures.
Conclusions: The increased incidence of S. aureus in all women with nipple pain suggests that it is a possible cause for nipple pain with minimal trauma and that microbiological culture should be considered in such cases. The strong association of infant nasal carriage with both nipple and milk carriage requires further investigation to determine causation and implications for management.
Funding: Medela AG.
BasmaA. AliM.D.1*AhmadAzza K.M.D., Ph.D.2Abdel-HafeezEkhlas H.M.D., Ph.D.2MoslamFadia A.M.D.3
Pediatric, Faculty of Medicine, Minia University, Minia, Egypt
Parasitology, Faculty of Medicine, Minia University, Minia, Egypt
Community and Preventive Medicine Departments, Faculty of Medicine, Minia University, Minia, Egypt
2. In Vitro Study of Anti-Protozoal Effect of Human Breastmilk
Background: Giardiasis and amoebiasis are the most commonly reported pathogenic protozoal diseases in tropical and subtropical countries, including Egypt. Some reports showed that the incidences of giardiasis and amoebiasis were decreased in breastfed infants. This protective effect has been attributed to the anti-infective and anti-inflammatory properties of human breastmilk.
Objective: To assess the direct in vitro lethal effect of colostrum and mature human milk on Entamoeba histolytica and Giardia lamblia trophozoites and compare them with artificial milk.
Methods: Forty samples (20 of colostrum and 20 of mature human milk) were collected from 40 apparently healthy lactating mothers, and another 20 samples of artificial humanized milk were prepared for comparison. Different milks were added in the cultured media with E. histolytica and G. lamblia trophozoites at different concentrations (2%, 5%, and 10%). Tubes were incubated for 30 minutes, 1 hour, 4 hours, and 18 hours, respectively. At the end of incubation, only motile parasites were counted with a hemocytometer. All experiments were done in triplicate and repeated at least twice.
Results: There were significant lethal effects on both E. histolytica and G. lamblia trophozoites on the media supplemented with colostrum and mature human milk rather than artificial milk or the control after 30 minutes. Furthermore, there were significant lethal effects of different concentrations of colostrum and mature milk on E. histolytica and G. lamblia at different periods of incubation with no statistically significant differences between them.
Conclusion: Colostrum and mature milk have significant lethal effects on E. histolytica and G. lamblia and protect breastfed infants more than artificial milk.
GurkaKelly K.MPH, Ph.D.12KellamsAnn L.M.D.2*Locasale-CrouchJenniferPh.D.1GurkaMatthew J.Ph.D.12
West Virginia University, Morgantown, WV
University of Virginia, Charlottesville, VA
3. Breastfeeding and Cognition: The Role of Confounders
Background: The association between breastfeeding and intelligence has been researched extensively; studies suggest a link between breastfeeding and cognition. However, these associations may not be causal, but due to residual confounding.
Objectives: To determine whether breastfeeding initiation and duration enhance cognition at 4 years of age and to identify what factors confound this association.
Methods: Cognitive data from 1,050 children, followed prospectively from birth during the National Institute of Child Health and Development Study of Early Child Care and Youth Development, were analyzed. Of primary interest were breastfeeding (never; 0–6 months; longer than 6 months) and its association with standardized (mean = 100; SD = 15) cognitive outcomes. Extensive modeling was performed to measure the impact of suspected confounders on this relationship.
Results: Significant (p < 0.05) positive associations were observed between breastfeeding and cognitive outcomes before adjusting for other factors. After adjusting for typically measured factors, particularly during retrospective studies (e.g., maternal age, education), significant—albeit smaller—positive associations persisted. However, after adjusting for variables typically not collected and often unavailable in retrospective studies—namely, observed quality of the home environment, mother's attitude regarding modernity of parenting, and maternal verbal IQ—no association between breastfeeding and cognition was observed.
Conclusions: This study suggests that the association between breastfeeding and childhood cognition may be due to residual confounding. It is important in examining this relationship to collect data on certain confounding factors that explain most, if not all, of the observed association.
Funding: NICHD grant R03-HD055298.
ParkerLesliePh.D.*SullivanSandraM.D.KruegerCharlenePh.D.
University of Florida, Gainesville, FL
4. Effect of Early Breastmilk Expression on Milk Volume and Timing of Lactogenesis Stage II Among Mothers of Very Low Birth Weight Infants: A Pilot Study
Background: Breastmilk is associated with health benefits in very low birth weight (VLBW) infants. A low milk supply and delayed lactogenesis stage II (LGS2) limit delivery of breastmilk to VLBW infants.
Objective: The purpose of this randomized pilot study was to evaluate the effect of initiation of milk expression <60 minutes following delivery compared to <6 hours in mothers of VLBW infants on the onset of LGS2 and milk volume.
Methods: Women were randomized to one of two groups. Group I (n = 10) began milk expression <1 hour following delivery, and Group II (n = 10) <6 hours. Milk volumes were measured on Days 1–7, 21, and 42. To determine timing of LGS2, women were questioned daily regarding a feeling of fullness in their breasts. Mean milk volumes and timing of LGS2 were compared using t tests.
Results: Group I produced more milk during all measurement sessions during the first 7 days, and this was statistically significant on Day 5 (p = 0.037). Total milk volume of mothers in Group I during the first week was over twice that of Group II and was marginally significant (p = 0.071). Group I produced significantly more breastmilk at both 3 (p = 0.003) and 6 (p = 0.02) weeks. Group I attained a statistically significantly earlier LGS2 (p = 0.03).
Conclusions: These findings suggest initiation of milk expression prior to 1 hour may increase milk volume and decreased time to LGS2 in mothers of VLBW infants.
NielsenSusan B.M.Sc.1*ReillyJohn J.Ph.D.1FewtrellMary S.Ph.D.2WellsJonathan C.K.Ph.D.2
Section of Human Nutrition, University of Glasgow, Scotland, UK
Institute of Child Health, University College, London, UK
5. Adaptations to Prolonged Exclusive Breastfeeding: Longitudinal Study of Mother–Infant Pairs following Who Recommendations on Infant Feeding
Background: The World Health Organization (WHO) recommends 6 months of exclusive breastfeeding, but breastfeeding rates worldwide reveal low levels of exclusivity and duration. Mothers often perceive milk supply to be insufficient to meet infant needs for 6 months.
Objective: The present study aimed to determine adequacy of milk intake at 6 months of age as well as changes in milk intake during prolonged exclusive breastfeeding.
Methods: Fifty mother–infant pairs were included from Scotland in a longitudinal observational study. At two time points, milk intake, total energy intake (from the doubly labeled water method), and anthropometry were measured, and questionnaires and behavior diaries were completed.
Results: Forty-seven mother–infant pairs completed, and 41 were exclusive breastfeeding at both time points. Mean (SD) infant ages were 15.4 (1.3) and 24.5 (1.3) weeks, respectively. Milk intakes were 923 (122) g/day at the 1st time point (n = 36) and 999 (146) g/day at the 2nd time point (n = 33). Milk intake increased significantly between time points (p = 0.003, n = 26 paired measurements). Infant total energy intakes and growth were adequate, compared to estimated energy requirements and WHO Child Growth Standards. Behavioral data indicated increased efficiency of breastfeeding over time, with no evidence of strain on breastfeeding practices.
Conclusions: Exclusive breastfeeding to 6 months is achieved by high milk intakes, which increase as infant energy needs increase, with normal infant growth and no marked changes in breastfeeding practices. This new evidence should help governments and health professionals in supporting mothers to follow WHO recommendations on infant feeding.
Funding: Scottish Government Chief Scientist Office, Yorkhill Children's Foundation.
OhyamaMakikoM.D., Ph.D.*NagasawaMayumiM.D.
Kanagawa Children's Medical Center, Kanagawa, Japan
6. How Japanese Women Maintain Milk Supply for Months in a Nicu Setting? Interviewing Mothers 1 Month after Delivery
Background: Maintaining sufficient milk supply for months is a challenge for mothers whose infants are in a neonatal intensive care unit (NICU). There is no standard of effective expression in a setting of long-term mother–infant separation.
Objective: To clarify how mothers manage expression for a long period and to find out effective support for them.
Methods: We interviewed mothers who gave birth at term or preterm in our hospital and were instructed both hand expression and electric pumping using Symphony® (Medela) before mothers' discharge and expressing at 1 month from April 2007 to May 2010. We excluded mothers whose infants were discharged or transferred to other wards or other hospitals or too ill to feed at 1 month. We asked how they expressed and how much milk they obtained at 1 week and 1 month.
Results: Interviewed were 175 mothers. The most common way of expression was double pumping combined with hand expression, followed by hands only, and double pumping without hands expression at both 1 week and 1 month. No relationship was found between the way of expression and mean daily volume (MDV). At 1 week, 103 mothers produced <500 mL of milk. Forty of them produced >500 mL/day at 1 month. Sixty-six percent of mothers who produced >300 mL/day at 1 week developed >500 mL/day MDV at 1 month.
Conclusions: About two-thirds of Japanese mothers use hand expression combined with or without pump. More than 300 mL/day MDV is one indicator for sufficient MDV at 1 month.
NarasimhanSudha RaniM.D.*KifleAlganeshCelsiMichelleMcCormickMargieCurryJanicePowersMelanieBrooksJulieKhauvChhuyShowalterLynnJegatheesanPriyaM.D.
Santa Clara Valley Medical Center, San Jose, CA
7. Implementation of Who's Ten Steps to Successful Breastfeeding to Improve Exclusive Breastfeeding
Background: Maternity practices and breastfeeding knowledge of healthcare staff are associated with an increased percentage of infants who exclusively breastfeed. We initiated an educational program to train nursing staff to promote exclusive breastfeeding.
Objective: To improve exclusive breastfeeding of all healthy infants at the time of hospital discharge.
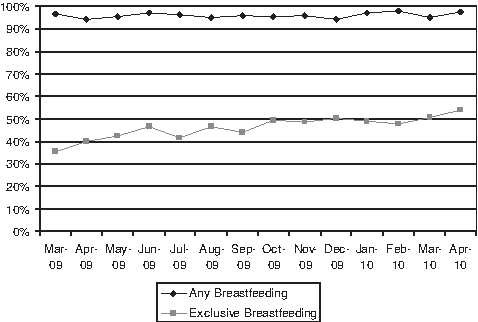
Methods: A mandatory 15-hour educational program based on the World Health Organization's (WHO's) Ten Steps to Successful Breastfeeding curriculum was initiated in April 2009 for all maternal–child health nursing staff. The outcomes of exclusive and any breastfeeding at the time of discharge (n = 4,747) were collected prospectively. Staff self-assessment tools were performed to evaluate the effectiveness of the educational program. We compared the outcomes from March 2009 to April 2010 using the generalized linear model.
Results: Seventy percent of nurses (n = 225) were trained over a 1-year period. We had a significant increase in the percentage of exclusively breastfed infants from 35% to 54% (p < 0.001) (Fig.) while any breastfeeding remained high (96%). The staff self-assessment tool showed that their knowledge on early initiation/support of breastfeeding improved after participating in the educational program.
Percentage of infants breastfeeding at the time of hospital discharge.
Conclusions: Implementation of an intense breastfeeding educational program for all nurses led to a significant and sustained improvement in exclusive breastfeeding. Our results also suggest that in addition to completing a lactation educational program for all nursing staff, we need to focus on other maternity practices including prenatal education to further increase exclusive breastfeeding.
Funding: First 5 of Santa Clara County for providing funding support for staff training and VMC Foundation for their continued support.
HayduSuzanneMPH1ShieldsLeona K.M.N.1SaraivaCarinaMPH1RamstromKarenD.O., MSPH1*FaheyCindyMSN2PetersKaren A.MBA2
California Department of Public Health: Maternal, Child and Adolescent Health Division, Sacramento, CA
The Perinatal Advisory Council: Leadership Advocacy and Consultation, Los Angeles, CA
8. Birth and Beyond California: Before and after a Hospital Continuous Quality Improvement Project to Support Breastfeeding
Background: Exclusive breastfeeding is the optimal mode of infant feeding for the first 6 months of life. According to 2007 data published by California Department of Public Health (CDPH), out of 87% planning to breastfeed, less than 43% of women exclusively breastfeed their infants while in the hospital. In 2008, the Maternal, Child, and Adolescent Health Division, CDPH began piloting Birth and Beyond California (BBC) to improve exclusive breastfeeding rates by assisting participating birthing hospitals to adopt evidence-based breastfeeding policies and Model Hospital Policy Recommendations. Selected Regional Perinatal Programs of California partnered with hospitals to develop and utilize interdisciplinary continuous quality improvement (CQI) teams to implement these policies.
Objective: Collaborate with California birthing hospitals with the lowest exclusive breastfeeding initiation rates to develop CQI that implements the Model Hospital Policy Recommendations.
Methods: Hospitals completed a Breastfeeding Policy Self-Appraisal before and after interventions to track their progress in policy implementation. Pre–post tests measured staff knowledge and self efficacy.
Results: In 23 participating hospitals, 685 staff completed BBC training leading to increased staff knowledge and self-efficacy. CQI strategies found imperative to implement evidence-based maternity policies and practices included: obtaining early administrative buy-in, creating a multidisciplinary hospital CQI team to develop and monitor breastfeeding policies, training staff to initiate skin-to-skin and attachment, and initiating a network among birthing hospitals. Educational materials developed and tested by BBC are available at the CDPH Breastfeeding and Healthy Living website.
Conclusions: CQI is essential in overcoming barriers to a mother's choice to initiate exclusive breastfeeding in the hospital.
Funding: California Department of Public Health, Maternal, Child, and Adolescent Health Division, Title V Federal Block Grant of the Social Security Act.
Poster Abstracts
WaltersKarenMPH, MPP*VaughanJanetMPHHanniKristaM.S., Ph.D.HernandezLisaM.D., MPH
Monterey County Health Department, Salinas, CA
1. Guidelines to Implementing a Local Lactation in the Workplace Policy
Background: Women returning to work postpartum may face challenges related to continuation of breastfeeding. The mother's decision to breastfeed often depends on support she receives in the workplace. Local county government can provide support to lactating mothers wishing to return to work through the implementation of local lactation in the workplace policies.
Objectives: We quantified the need for and identified steps for developing an effective lactation in the workplace policy. We summarized our steps in a workplace lactation policy development toolkit.
Methods: We conducted surveys and used other surveillance methods with lactating mothers interested in returning to work postpartum, local perinatal workers, and breastfeeding coordinators at other counties in California. Data were used to develop a workplace lactation policy, support its adoption through county government, and develop a toolkit summarizing our steps.
Results: The majority of lactating mothers wanted support for continuing lactation after they returned to work. With a county supervisor's support, the Monterey County Health Department was successful in having the Lactation in the Workplace Policy approved by the Board of Supervisors on April 13, 2010. Our toolkit consists of basic and best practices, an Employee's Guide to Breastfeeding in the Workplace, suggested employee breastfeeding educational trainings and materials, and guidelines to develop a local lactation policy.
Conclusions: Monterey County Health Department was able to use a data-driven methodology to successfully pass a local policy for workplace lactation accommodation. Future work will assess the policy's implementation in county workplaces.
NelsonDesiree*BentBeckyM.D.
Sacred Heart Medical Center RiverBend, Springfield, OR
2. Baby Connection: A Demonstration of Step Ten World Health Organization/United Nations Children's Fund Ten Steps to Successful Breastfeeding
Background: The World Health Organization has established a global program for breastfeeding support. The Ten Steps to Successful Breastfeeding address prenatal education, in the hospital or birth center care, and continued support after discharge. The literature supports the Ten Steps as evidenced-based care. Step Ten is: Foster the establishment of breastfeeding support groups and refer mothers to them on discharge from the hospital or clinic. Baby Connection is a collaborative, community-based demonstration of Step Ten. The primary focus of Baby Connection is to provide mothers with an opportunity to experience breastfeeding support and education that is evidenced based. Education is provided by experienced feeding specialists who are International Board Certified Lactation Consultants or clinical lactation educators. Baby Connection also provides an opportunity for mothers to meet and talk with each other.
Objective: To demonstrate key topics that the mothers identified as important to them.
Methods/Results: A retrospective review of the documentation revealed seven key areas of concern: (1) infant feeding patterns; (2) infant feeding techniques, latch, and positioning; (3) infant sleep patterns; (4) breastmilk supply; (5) infant weight gain patterns; (6) starting complementary foods, timing, and food choice; and (7) working and breastfeeding.
Conclusion: Mothers have multiple key areas of concern regarding the care and feeding of their babies, and they will seek information about these concerns. Continuing support is viewed as a positive experience as evidenced by the frequency with which mothers return to Baby Connection each week and comments recorded in focus group interviews.
LabbokMiriamM.D., MPH*TaylorEmilyMPHColganBrookMPHNickelNathanMPHCameronBarbaraM.A., MSWTurayKhadijaMPHRingel-KulkaTamarM.D., MPHJensenElizabethMPH
Carolina Global Breastfeeding Institute, Department of Maternal and Child Health, Gillings School of Global Public Health, University of North Carolina, Chapel Hill, NC
3. Addressing Disparities in Breastfeeding through a Comprehensive Statewide Approach
Background: The Carolina Global Breastfeeding Institute carried out a review of the literature on exclusive breastfeeding and studies of the “State of Breastfeeding” in North Carolina. Gaps and facilitators were identified, and approaches to changing policy and practices were considered in discussion with the State Department of Public Health.
Objective: To address disparities in breastfeeding in North Carolina through a comprehensive approach through translational and operational research addressing identified obstacles.
Methods: Systematic review of the literature, re-analysis of existing datasets, and formative, translational, and operational research techniques were employed.
Results: Re-analysis of county and state data, formative research in faith-based, community/county, and service settings, and operational study of interventions in hospital and child care settings have yielded information upon which to build a comprehensive approach to reducing disparities in breastfeeding North Carolina and beyond. As a result, several operational interventions are underway at the program and policy levels, to increase breastfeeding, including (1) a proposed statewide hospital-based Ten Steps assessment, (2) a proposed statewide effort to increase exclusivity of human milk feeding, (3) a disparities-based targeting of hospitals for Ten Steps support, (4) a disparities-based targeting of child care facilities, (5) disparities-based community-based participatory research in two settings, and (6) an intention study to further elucidate barriers to achievement of breastfeeding goals. This approach has been successful, and up-to-date findings, as well as uptake in other settings, are included.
Conclusions: Targeted interventions, if based on preliminary study to identify population-based issues, can reduce disparities in breastfeeding rates in the United States.
PreerGenevieve L.M.D.1*EdwardsRoger A.Sc.D.2PisegnaJessica M.MSEd3PhilippBarbara L.M.D., FABM1
Boston Medical Center and Boston University School of Medicine, Boston, MA
Northeastern University School of Public Health, Boston, MA
Boston Medical Center, Boston, MA
4. Got Rates? asking the Right Breastfeeding Question on the Massachusetts Birth Certificate
Background: In Massachusetts, statewide breastfeeding data are collected together with birth certificate information. All mothers are asked, “Are you breastfeeding or do you intend to?” This question fails to assess whether mothers are actually breastfeeding and yields no information about exclusive breastfeeding rates.
Objective: To determine whether maternity facilities in Massachusetts collect their own breastfeeding rates.
Methods: We administered an online survey on breastfeeding rate collection to all 50 maternity facilities in Massachusetts.
Results: We had a 90% response rate from facilities representing 96% of births in Massachusetts: 71% of respondents were nurse managers or clinical administrators, and 78% of respondents reported that their facility used a method besides birth certificate data to collect breastfeeding rates. More facilities used a paper-based system than an electronic medical record. Ninety-three percent of respondents stated they would be interested in a statewide effort to collect breastfeeding rates.
Conclusions: The majority of maternity facilities in Massachusetts collect their own breastfeeding rates; most facilities desire help from the state in this process.
Implications: Our results demonstrate the limited utility of breastfeeding rates derived from the current birth certificate question. Additionally, they may reflect the impact of 2010 Joint Commission Perinatal Core Measures requiring maternity facilities to collect exclusive breastfeeding rates. A new version of the Massachusetts birth certificate question could provide a powerful tool for collecting data on exclusive breastfeeding. For example, the simple question “Has your baby received any formula during his hospital stay?” would provide accurate information for the calculation of exclusive breastfeeding rates.
TchengBarbara M.M.D.1*PurdyIsabell B.Ph.D.2WhitesideChristy3
Department of Pediatrics, Ronald Reagan UCLA Medical Center & Mattel Children's Hospital at UCLA, Los Angeles, CA
Division of Neonatology and Developmental Biology Department, David Geffen School of Medicine at UCLA, Ronald Reagan UCLA Medical Center & Mattel Children's Hospital at UCLA, Los Angeles, CA
UCLA Department of Nursing, Ronald Reagan UCLA Medical Center & Mattel Children's Hospital at UCLA, Los Angeles, CA
5. Resident Case Report: Making the Case for Baby-Friendly Hospital Initiative
Background: At a large university-based teaching hospital, multiple efforts to adhere to all 10 steps of the Baby-Friendly Hospital Initiative have resulted in small improvements, but the commitment to complete all the steps has not been present.
Methods/Objective: This case study identifies the three major challenges of our institution in becoming Baby-Friendly and the successful strategies that are being used to overcome these barriers.
Results: The greatest obstacles are overcoming assumptions in financial barriers, educating physicians and nurses, and eliminating formula donations to the hospital. In order to seek administrative support, the World Health Organization Ten Steps of Successful Breastfeeding were discussed with the COO. Additional letters of support were obtained from the CFO, CEO, Chief Nursing Officer, Medical Directors of Neonatology, OB-GYN, and Pediatrics, and Nursing Directors of NICU and Maternal-Newborn. To receive educational materials and instruction, an application was submitted to Birth and Beyond California. Our institution was chosen to receive this program to educate healthcare staff, using a “train-the-trainer” method. To further address education, the pediatric residency breastfeeding curriculum was redesigned to include the free online Wellstart International curriculum and bedside lactation rounds. The first step to limiting formula was collecting data regarding the amount of formula used and its costs, including the stocking fee.
Conclusions: University-based teaching hospitals can lead the way in promoting breastfeeding. Successful strategies to becoming Baby-Friendly are being employed to overcome even the most difficult challenges of educating a large hospital medical staff and eliminating formula donations, despite the perceived financial barriers.
Abul-FadlAzza M.A.M.D.1*KharboushIbrahimPh.D.2FikryMohgaPh.D.3AdelMonaM.Sc.1
Pediatric Department, Benha Faculty of Medicine, Benha, Egypt
Alexandria High Institute of Public Health, Alexandria, Egypt
Alexandria Health Directorate Ministry of Health, Alexandria, Egypt
6. Determinants of Mother Willingness to Relactate in the First 3 Months Postpartum
Background: Early discontinuation of breastfeeding exposes babies to severe and fatal illnesses. Finding effective ways for supporting mothers to return to breastfeeding is a priority in child health.
Objective: The aim of the study was to identify the barriers to relactation among Egyptian women who have stopped breastfeeding in the first 3 months postpartum and to test different interventions for relactation.
Methods: This is a prospective longitudinal cohort study of 200 non-breastfeeding mothers with babies <3 months of age. They were proportionately selected from 11 health centers in six out of the seven districts of Alexandria, Egypt. The mothers were randomly assigned to three different forms of counseling to relactate, including coaching, problem solving, and cautioning. All were followed up over a period of 6 weeks.
Results: The mothers had introduced bottle feeding because of perceived milk insufficiency (66.5%), nipple soreness (49.5%), and infant strike (26.5%). Breastfeeding initiation was delayed after 3 hours in 87%; 46.5% and 100% of babies were, respectively, exposed to pacifiers and bottles before 6 weeks of life. All mothers tried to change their practices, but only 10% were able to relactate over the period of follow-up. The most effective educational strategy was the problem solving (45%) and the coaching (50%). The least effective was the cautioning approach (5%). Determinants of relactation included mother education (100%), cup feeding with no nipples or soothers (70%), and husband involvement (70%).
Conclusions: Baby-Friendly practices at birth and postnatal support for breastfeeding continuity using effective communication strategies that raise mother's self esteem are pivotal to ensuring successful breastfeeding.
7. Comparison of the Knowledge Attitude and Practice of Mothers in Upper Versus Lower Egypt Towards the Ten Steps of the Unicef-Bfhi Program
Introduction: Despite the proven effectiveness of the Ten Steps to Successful Breastfeeding adopted by the World Health Organization/UNICEF Baby-Friendly Hospital Initiative (BFHI), implementation strategies are still a major concern.
Aim: To assess the knowledge, attitudes, and practices of mothers towards practices related to the Ten Steps.
Subjects and Methods: This is a cross-sectional descriptive study including 1,053 breastfeeding mothers with infants <24 months attending maternal–child health units in 12 governorates: five in Upper Egypt (UE) and seven in Lower Egypt (LE).
Results: Delayed breastfeeding initiation was present in 75% in LE and 61% in UE. Nipple pain occurred in 56% of mothers in UE and 36% in LE (p < 0.001). Maintaining milk by expression was practiced by 42.8% of mothers in LE and 12% in UE. Two-thirds of mothers in UE and LE offered herbal drinks, and one-third fed formula to babies before 6 months. Pacifiers were offered early by 43.2% in LE and 39.2% in UE and bottle by 56.8% in UE and 51.9% in LE. Mothers think that babies can only be fed by bottle in 60.5% in UE and 39.2% in LE (p < 0.001), while 66% in UE compared to 44% in LE knew the negative effects of bottles on breastfeeding (p < 0.0001).
Conclusions: Interventions to improve community practices towards BFHI should be individualized to regional needs with a focus on educational strategies.
FlahermanValerie J.M.D., MPH1*HicksKatherine G.1LeeKathryn A.Ph.D.2
Department of Pediatrics, University of California, San Francisco, San Francisco, CA
Department of Family Health Care Nursing, University of California, San Francisco, San Francisco, CA
8. Provider Messages Regarding Newborn Weight Loss Impact Maternal Perception of Milk Supply
Background: Newborn weight loss is associated with maternal perception of insufficient milk supply. The impact of provider recommendations on maternal perception of the relationship between newborn weight loss and milk supply is unknown.
Objective: We examined how provider messages influence maternal perception of newborn weight loss among mothers with concerns about milk supply.
Methods: We conducted a qualitative study with 10 focus groups of 56 mothers of infants 2–6 months old who had concerns regarding milk supply. We completed three groups with mothers who breastfed exclusively for 2 months, four groups with mothers who breastfed with formula for 2 months, and three groups with mothers who discontinued breastfeeding before 2 months. A trained facilitator questioned participants about breastfeeding experiences, weight loss concerns, and provider messages. Sessions were audio recorded and transcribed verbatim. The transcripts were coded independently by two investigators and analyzed using Grounded Theory methods.
Results: Many mothers felt that newborn weight loss was due to insufficient milk supply and reported associated guilt, fear, and anxiety. Mothers reported that their healthcare providers frequently reinforced the connection between weight loss and milk supply problems. Mothers who started formula often did so in response to providers' comments about weight loss and were relieved when their baby's weight began increasing.
Conclusions: Providers' messages about newborn weight loss in the first weeks of life affect a mother's emotional state and her perception of milk supply. Providers should be aware that messages regarding weight loss may promote formula use.
Funding: V.J.F. has been supported on this project by grants 5 K12HD052163 and 1 K23HD059818 from the National Institute of Child Health and Human Development.
RosinStefanie
University of Bielefeld, Bielefeld, Germany
9. Experts in the Lactation Field Identify Remaining Obstacles to Rebuilding the Breastfeeding Culture
Background: In spite of World Health Organization (WHO)/UNICEF programs and subsequent measures to promote breastfeeding, breastfeeding still does not represent the norm for infant feeding on a global scale.
Objective: A questionnaire for experts in the field of lactation was designed to assess the international situation of breastfeeding, lactation consulting, and breastfeeding promotion to assess the work situation including contentedness, motivation, and acceptance, the progress of breastfeeding promotion including the identification of remaining obstacles, and ranking of priority measures towards a breastfeeding culture.
Methods: Quantitative evaluations based on closed question items included mainly descriptive statistics. Qualitative methods based on open question items categorized mutually exclusive answer groups by paraphrasing.
Results: Lactation consulting is lacking of payment and career opportunities on an international level and needs a firm position in the healthcare system with reimbursement to the full extent of work. However, lactation consultants describe themselves as mostly contented and idealistically motivated. Societal and political support is poor, and research funds are lacking, National Committee for Breastfeeding should gain political weight and take on additional tasks. Healthcare providers without education in lactation represent a decisive obstacle to breastfeeding. WHO/UNICEF measures remain priority with overdue implementation.
Conclusions: Health policies to protect and promote breastfeeding including legislation, consumer protection, and the integration of lactation consulting in the healthcare systems represent key measures to achieve progress in the implementation of WHO/UNICEF measures and subsequent programs to re-establish the breastfeeding culture. A basic education of all healthcare providers in the lactation field seems indispensable to promote breastfeeding consistently.
McIntyre-DanielSophiaM.D., MPH*LiberatosPennyPh.D.
New York Medical College School of Health Sciences and Practices, Valhalla, NY
10. Discussion of Infant-Feeding Method and its Relationship to Breastfeeding Initiation: The Role of the Healthcare Provider
Background: Rates of breastfeeding among African-Americans have long been found to be lower than those for whites and Latinas. Although low socioeconomic status among African-Americans has often been cited as a factor, other factors may play a role—especially that of the healthcare provider (HCP).
Objective: To examine the role that the HCP may play in infant-feeding choice, specifically, to assess whether the timing of the discussion by the HCP regarding infant-feeding method (IFM) influences likelihood of breastfeeding among college-educated African-American women, a subgroup not often studied in this area.
Methods: Eighty-five African-American women were recruited through the alumni association of Spelman College and through local chapters of the Delta Sigma Theta sorority. They were asked to complete a survey questionnaire through Survey Monkey regarding their infant-feeding choices.
Results: More than one-quarter of the women reported no discussion regarding IFM by their HCP, and an additional one-third had already decided by the time the HCP raised the issue. Timing of discussion was subdivided into three groups: early, 1st trimester or before (n = 12); late, after 1st trimester (n = 36); or no discussion (n = 19). Women reporting an early discussion with their HCP were also significantly more likely to report that their HCP had discussed the benefits of breastfeeding, that the HCP showed strong/moderate support for breastfeeding, and that they were more likely to breastfeed.
Conclusions: The findings of this study support the importance of early and frequent discussions by the HCP regarding IFM in contributing to improving rates of breastfeeding among African-American women.
JoshiRavneet S.M.D.*VinodAnuradhaGowriDivya
Department of Pediatrics and Neonatology, Manipal Hospital, Bangalore, India
11. Experience of a Lactation Physician at a Tertiary Care Center in Urban India
Background: Practice of breastfeeding medicine as a specialty has been limited to very few centers in India. Manipal Hospital, Bangalore, a tertiary referral center, has recently introduced lactation physician services to assist newborns and their mothers with lactation problems.
Objective: To evaluate the role of a specialist lactation physician in tertiary care maternal–child health centers in India.
Methods: A retrospective study of data from October 2009 to March 2010 was conducted. This covered a population of term, preterm, and high-risk newborns requiring neonatal intensive care unit (NICU) care.
Results: Out of the 1,208 deliveries conducted during the study period, 355 (29%) were referred for lactation consultation. Maternal reasons of reference were flat/inverted/large nipples (23%), engorged breast (32%), sore nipples (16%), and medical conditions like gestational diabetes mellitus, hypothyroidism, polycystic ovary disease, and obesity (37%). Neonatal reasons of reference were term babies with feeding problem (42%), preterms (29%), and multiple births (5%). Key interventions included adjusting position (59%), latch (72%), frequency of feeding (55%), technique of expression/pumping regimen (33%), and adding a galactogogue (20%). Key challenges overcome were formulation of a hospital breastfeeding and supplementation policy, early intervention in high-risk NICU cases, and training of residents and staff to support breastfeeding. The outcome after lactation consultation was satisfactory in >90% cases.
Conclusion: Accurate assessment and timely interventions by a lactation physician helped in establishing breastfeeding and reduced the incidence of bottle and formula feeding.
WittAnnM.D.12*FlockeSusanPh.D.34SmithSamanthaM.A.3MasonMary Jane3
Breast Feeding Medicine of Northeast Ohio, Cleveland, OH
Senders Pediatrics, Cleveland, OH
Department of Family Medicine, Case Western Reserve University, Cleveland, OH
Department of Epidemiology & Biostatistics, Case Western Reserve University, Cleveland, OH
12. Integrating Lactation Consultants into a Pediatric Practice
Background: Although research shows that healthcare professionals' support improves breastfeeding duration, many physicians do not believe they have adequate time to address breastfeeding concerns during office visits. To comply with the American Academy of Pediatrics 2005 breastfeeding policy regarding newborn follow-up, the study practice began utilizing a lactation consultant overseen by a physician to conduct the initial office visit for all breastfeeding infants.
Objectives: (1) Describe a pediatric practice's implementation of routine lactation consultation evaluation for all breastfeeding infants approximately 2 days after hospital discharge. (2) Evaluate the impact of the program on breastfeeding rates.
Methods: A retrospective chart review was performed on consecutive newborns before (2007) and after (2009) implementation of the program. Exclusive breastfeeding was assessed at each well child visit during the infant's first 9 months. Logistic growth curve and χ2 analyses were used to test the association between implementation status and exclusive breastfeeding.
Results: Mothers and infants in 2007 and 2009 were similar with regard to type of insurance, parity, gestational age, multiple births, and cesarean sections. Overall, exclusive breastfeeding improved after program implementation (odd ratio = 1.12, 95% confidence interval 1.02–1.23). In 2009, exclusive breastfeeding rates at 2 months, 4 months, 6 months, and 9 months were greater than 2007 rates by 10%, 15%, 11%, and 9%, respectively. Logistic growth curve analysis indicated the difference across these time points was significant between 2007 and 2009.
Conclusion: A routine post-discharge outpatient lactation visit coordinated within a primary care practice improved breastfeeding initiation, and this effect was sustained for 9 months.
Funding: This project was supported in part by a grant from HRSA DHHS/HRSA D54 HP05444-01-00.
RevaiKrystalM.D., MPH*BriarsLesliePharmDCochranKelly A.PharmD
University of Illinois Medical Center at Chicago, Chicago, IL
13. Case Series of Sjogren's Syndrome and Poor Milk Supply
Background: Sjogren's syndrome (SS) is an autoimmune chronic inflammatory and lymphoproliferative disease that is characterized by cellular infiltration of the exocrine glands. Affected individuals typically complain of dry eyes and mouth. Insufficient milk supply has not been a documented feature of SS. Hydroxychloroquine is a mild anti-inflammatory commonly used in patients with autoimmune diseases.
Objective: This case series describes two women with known SS and poor milk supply.
Method: Observational study.
Results: Two mothers with known diagnosis of SS at the time of delivery of newborn infants. One mother (M1) was primagravida; the second mother (M2) had had one previous child. M1's baby lost 11% of body weight by day 3 of life and had no bowel movements for greater than 24 hours, resulting in start of supplemental feeds. Conventional methods of increasing milk supply started with limited improvement. M2 did not have difficulty with milk supply in the early postpartum period. M1 and M2 presented at 8 and 6 weeks, respectively, with complaint of being unable to keep milk supply up with the baby's demand. They reported nursing every 2–3 hours with additional episodes of milk expression with an electric pump. Both mothers reported a maximum of 2 oz of milk over a 30-minute period of expression. Each mother was prescribed 200 mg of hydroxychloroquine, which resulted in improved milk supply. M1 had increased breast size and volume of expressed milk in 2 days; M2 reported improvement within 2 weeks.
Conclusions: Women with SS may have poor milk supply partially responsive to hydroxychloroquine.
SmillieChristina M.M.D., FABM12*NelsonAntonia M.Ph.D.3
Breastfeeding Resources, Stratford, CT
Bridgeport Hospital, Yale New Haven Health System, Bridgeport, CT
St. Anselm College, Manchester, NH
14. Testing a Theory of Slow Weight Gain Among Breastfeeding Infants
Background: Breastfeeding infants who gain weight slowly present a management challenge to both parents and providers. The breastfeeding infant's appetite and ability to self-regulate intake to growth and energy needs appear compromised in the infant with slow weight gain (SWG), creating a vicious cycle of low energy, poor appetite, poor feeding, poor weight gain, and decreased maternal milk production.
Objectives: The purpose of this preliminary qualitative study was to test a specific theory of SWG, to introduce and assess an associated approach to clinical management, and to describe how this approach to SWG is experienced.
Methods: A naturalistic, multiple case study design was utilized based on established methodological guidelines for qualitative studies. A purposeful sample of 12 SWG cases was solicited from a private breastfeeding medicine practice. A synopsis of each case was written utilizing data from chart review and audiotaped interviews. Common themes and factors were then identified, and cross-case assertions were developed.
Results: All mothers initially described their SWG infants as “sleepy,” and, after intervention, all noted behavioral changes consistent with the proposed theory. Three cases had poor outcomes. Cross-case assertions suggest that: mothers take personal responsibility for SWG; mothers must “buy into” the suggested plan for it to work; pediatricians were perceived to differ from lactation consultants in their evaluation of SWG; and addressing SWG is intense for mothers and professionals.
Conclusions: Cross-case analysis largely supported the theory. Further quantitative and qualitative research of this clinical syndrome and its management is needed.
Funding: Southern Connecticut State University School of Health and Human Services.
ChungYoo-MiM.D., FABM*LeeMiraM.D.
The Academy of Breastfeeding Medicine Korea, Seoul, Korea
15. Analysis of Online Consultations on the ABMK Website
Background: Despite the urgent need of mothers, breastfeeding medicine practices are time-consuming and hard to be reimbursed.
Objective: To analyze actual needs of Korean breastfeeding mothers, which vary depending on their nursing conditions and babies' ages using the consultation data on the The Academy of Breastfeeding Medicine Korea (ABMK) website (www.bfmed.co.kr/) and to set up targeted breastfeeding medicine practices in a primary care model.
Methods: A descriptive study, reviewing all the online consultations on the ABMK website from December 2005 to March 2010.
Results: We analyzed 10,164 online questions from 6,100 parents during the 51-month period. The age distribution of the babies was as follows: newborn (10.9%), 1 month (20.6%), 2 months (17.4%), and 3 months (13.2%). The exclusive breastfeeding rate was 67.4%, which increased with the babies' age until 6 months. Of the mothers who initiated first breastfeeding within 6 hours, 46.1% had a normal delivery and 16.6% had a cesarean section. The rooming-in rate in obstetric wards was 37.9%. The most commonly asked question was if the amount of breastmilk was sufficient for babies' needs (18.4%). Questions on the effect of mothers' medication on milk supply or on infants' health were the next common ones (13%). The concern about babies' growth velocity was ranked as third (10.2%). This order varied depending on babies' ages.
Conclusions: Physicians' active and effective participations in online breastfeeding consultations would help them identify actual needs of breastfeeding mothers and set up targeted breastfeeding medicine practices.
BordersAnn E.B.M.D., M.Sc., MPH1*PatykMagdalynM.S.2ChayPamela2ReyesBrenda3WolfeKaitlin1HudsonLakisha3AbramsonRachelM.S.3
Institute for Healthcare Studies, Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Northwestern University Feinberg School of Medicine, Chicago, IL
Department of Women's Programs & Education, Northwestern Memorial Hospital, Chicago, IL
Health Connect One, Chicago, IL
16. Successful Initiation of Breastfeeding Peer Counselor Program in a Teaching Hospital Affiliated Prenatal Clinic
Background: The Northwestern Prentice Ambulatory Care Clinic provides prenatal care to 500 low-income patients annually (60% African-American, 30% Hispanic, 10% Caucasian) and has historically low rates of breastfeeding.
Objective: The goal of this project was to initiate a breastfeeding peer counselor program in a large academic prenatal clinic and analyze change in breastfeeding rates after 1 year.
Methods: A breastfeeding peer counselor (prior clinic patient with peer counselor training) was hired in January 2009 part-time and expanded to full-time in January 2010. She provided: breastfeeding counseling to new prenatal patients, hands-on post-delivery support in the hospital, phone triage for postpartum patients with questions, and support to breastfeeding patients at the postpartum visit. She also initiated a free monthly breastfeeding class. Chart reviews of 100 serially delivered patients were completed prior to program initiation and again after 1 year. The peer counselor recorded counseling visits and breastfeeding outcomes for all patient interactions.
Results: Chart reviews found overall breastfeeding initiation rates improved from 38% at baseline to 57% after 1 year with a part-time counselor. In 14 months, the peer counselor provided breastfeeding counseling to 531 prenatal patients and completed 135 postpartum hospital visits, and 14 breastfeeding classes were held with 172 patients and partners. Of the 531 patients who received prenatal breastfeeding counseling, 280 have delivered, and 237 initiated breastfeeding (85%).
Conclusions: A breastfeeding peer counselor program can improve breastfeeding rates in an underserved population and can be effectively initiated in a prenatal clinic associated with an academic teaching hospital.
Funding Source: The Evergreen Invitational Grand Prix Women's Health Grant Initiative 2009 and 2010 and NIH/NICHD grant 1K12 HD050121-02, Women's Reproductive Health Research Program.
Bunker-AlbertsMicheleMSN*KayLilyanMSN, MPHRouxJoanM.D.
Alameda County Medical Center, Oakland, CA
17. Whether to Supplement
Background: In order to support exclusive breastfeeding in the hospital setting, an algorithm was developed to assist hospital staff in the decision-making process concerning supplementation of breastfeeding infants.
Objective: To avoid unnecessary supplementation through implementation of a standardized, evidence-based strategy.
Methods: The Supplement Decision Tool is being implemented as a quality improvement project related to the hospital's Baby-Friendly certification process. It consists of (1) a set of questions the nurse should have the answers to before consulting the pediatric provider and (2) a flow chart representing the decision process followed by the pediatric provider in deciding whether to supplement. Following implementation in the clinical setting after the final class (June 10, 2010), a prospective chart review will be completed during the ensuing 90 days to determine whether there is a significant difference in the rate of supplementation, compared with retrospective review of charts from a year ago prior to the first class.
Results: It has been evaluated favorably by nurses in the classroom as well as with pediatricians and lactation consults in the clinical setting. The results of the data analysis are pending the prospective review as described above.
Conclusions: The Supplement Decision Tool is adaptable and easily implemented. There will be data on clinical outcomes by the end of September, as mid-September will mark the 90 days following the final nurses' training, the designated time period during which data collection can be completed.
HerrineGailM.D.1*McCarthyMary2ValeggiaClaudiaPh.D.2
Temple University Hospital, Philadelphia, PA
University of Pennsylvania, Philadelphia, PA
18. Breastfeeding Attitudes and Intentions: Positive Effects of a Small-Scale Intervention
Background: The population in northeast Philadelphia is mainly composed of inner-city, low socioeconomic status people. Despite the numerous nutritional, immunological, psychoemotional, and economic benefits of breastfeeding, baseline survey data from this population found extremely low prevalence of breastfeeding, particularly among Puerto Rican mothers.
Objective: The purpose of this study was to explore the extent to which a small-scale intervention intended to promote breastfeeding affected the breastfeeding attitudes and intentions of the women who received pre- and postnatal care at the Woman's Care at Northeastern Hospital in Philadelphia, PA.
Methods: This intervention, part of Programa Lactar, was relatively simple and economical: It included posters for the waiting room and DVDs supporting breastfeeding, a discussion by the doctor of the benefits of breastfeeding with each patient, and a weekly support group held lead by a lactation consultant at the clinic. Data were gathered through a survey and a questionnaire from 118 prenatal and 79 postpartum women prior to implementation and then from 168 prenatal and 98 postpartum women who had been exposed to these changes.
Results: The results indicated there was a significant increase in positive attitudes and in intention to breastfeed after the intervention. There was still a low prevalence of breastfeeding. However, those women who did breastfeed tended to do so for a longer duration of time.
Conclusions: The results of this study demonstrate that small, educational breastfeeding programs such as Programa Lactar can help to increase acceptance and improve rates of breastfeeding in a target population.
Funding: Pennsylvania Department of Health and University of Pennsylvania Research Funds.
OlenickPatriciaPh.D.1*BerensPamelaM.D., FABM2
Texas A&M, Corpus Christi, TX
University of Texas–Houston Medical School, Houston, TX
19. The Effect of Structured Group Prenatal Education on Breastfeeding Confidence, Duration, and Exclusivity to 12 Weeks Postpartum
Background: Breastfeeding exclusivity and duration remain below U.S. 2010 goals. Self-efficacy literature supports the premise that increased maternal confidence promotes improved exclusivity and duration.
Objective: (1) To determine if group prenatal education can improve breastfeeding outcomes in a private practice population. (2) To identify the relationship between maternal confidence (measured with the Breastfeeding Self-Efficacy Scale) and breastfeeding outcomes.
Methods: A randomized, controlled prospective trial on whether one class based on breast-feeding self-efficacy theory improves outcomes.
Results: Of n = 182 mothers, 168 completed data collection. The sample was largely Hispanic, married, and low-income. Breastfeeding confidence was associated with higher rates of full breastfeeding at weeks 1, 6, and 12. High confidence scores were associated with longer duration (10 weeks vs. 5 weeks, p < 0.0001). The group class (intervention) was not associated with significant differences in outcomes with “intent to treat” analysis. However, in analysis by compliance to protocol, there were consistent differences in subgroups. For example, at 12 weeks, the “any breastfeeding class” group had higher “full breastfeeding” rates for cesarean mothers (35% vs. 8%) and mothers without prior breastfeeding experience (35% vs. 11%). Both subgroups also had longer duration (9 vs. 6 and 5 weeks, respectively) with breastfeeding class attendance. In multivariate analysis, positive effects for actual attendance to any breastfeeding class were seen on breastfeeding exclusivity at 1 week postpartum. Breastfeeding confidence scores consistently predicted both exclusivity and duration.
Conclusions: Breastfeeding education shows potential for improving breastfeeding outcomes, especially in high-risk subgroups. Increased maternal confidence improves exclusivity and duration.
Funding: Eta Omicron chapter of Sigma Theta Tau International.
SattariMaryamM.D.12*SerwintJanetM.D.1LevineDavidM.D.1
Johns Hopkins University School of Medicine, Baltimore, MD
University of Florida College of Medicine, Gainesville, FL
20. Physician Mothers: How can we Practice what we Preach?
Background: Despite high breastfeeding initiation rates, physician mothers in the United States are at risk of premature breastfeeding cessation. Return to work, work schedule, diminishing milk supply, and lack of adequate time and space for milk expression have been identified as obstacles to breastfeeding maintenance by physician mothers.
Objective: We explored possible solutions to premature breastfeeding cessation by physician mothers.
Methods: Physician volunteers were interviewed in person or by phone, using a breastfeeding questionnaire. Criteria for participation were being a female physician and having had at least one biological child. Open-ended questions were asked to explore participants' infant feeding intents and actions, enablers and obstacles of breastfeeding initiation and maintenance, and perceptions as far as changes and interventions to encourage and improve physician mothers' breastfeeding behavior after return to work.
Results: The study included results of interview with 50 physician mothers (12 in training and 38 had completed training at the time of study). Solutions offered by study participants can be classified into four major categories: space dedicated to milk expression (88%), adequacy of time for milk expression (56%), sufficient milk supply (46%), and supportive health policy (44%).
Conclusions: The suggested workplace changes analyzed in this study indicate that physician mothers are well aware of their main obstacles to breastfeeding maintenance after return to work. Many of the suggested solutions are simple and practical interventions that merit further considerations in residency programs and medical practices. Improving breastfeeding success of physician mothers would strengthen their clinical breastfeeding advocacy and, therefore, improve their patients' breastfeeding rates.
AlvarezRebeca1*SattariMaryamM.D.12
University of Florida College of Medicine, Gainesville, FL
Johns Hopkins University School of Medicine, Baltimore, MD
21. Breastfeeding Practices of Professional Women—Urban Legend?
Background: Although breastfeeding rates have increased in the United States, most mothers wean before 6 months because of perceived difficulties rather than maternal choice. While full-time employment is negatively associated with breastfeeding duration, women employed as professionals are thought to breastfeed longer than other working mothers.
Objective: We sought to examine existing literature to investigate relationship of maternal work-type and breastfeeding.
Methods: A literature search was conducted, using the keywords “breastfeeding,” “lactation,” “maternal work-status,” and “maternal employment” in the PubMed database. Relevant articles from 1976 to 2009 were selected, and their bibliographies were reviewed for identification of additional important articles.
Results: A total of 34 relevant articles were identified, two of which concluded that mothers employed as professionals or in managerial positions breastfeed longer than other working women. However, these manuscripts did not examine breastfeeding intentions of mothers, nor did they define “professional.” Only nine manuscripts addressed breastfeeding among specific occupations (eight among physician and one in Navy mothers). While physician mothers have excellent breastfeeding initiation rates, their continuation rates are lower than the general population.
Conclusions: When examined specifically, physician mothers (a group of “professionals”) seem at risk for premature breastfeeding cessation. While it is conceivable that other professional mothers have similar challenges as far as breastfeeding continuation, existing literature does not convincingly support this hypothesis. More importantly, this study brings into question the earlier claim that professional mothers breastfeed longer than other working mothers. Given the prevalence of mothers in the workforce, the impact of specific maternal occupations on breastfeeding should be explored further.
BoiesEyla G.M.D., FABM*LawsonTerryVaucherYvonne E.M.D., MPH
Divisions of General Academic Pediatrics and Neonatology, Department of Pediatrics, University of California, San Diego, CA
22. Breastfeeding Premature Multiples after NICU Discharge
Background: The University of California, San Diego (UCSD) Premature Infant Nutrition Clinic (PINC) was established to provide premature infants and their mothers with lactation support after discharge from the neonatal intensive care unit (NICU).
Objective: To describe maternal goals, adequacy of breastmilk production, and transition to breastfeeding in mothers of preterm multiples.
Methods: Observational data were prospectively collected on 20 consecutive mothers of premature multiples (three triplet sets, 17 twin sets) seen in PINC from November 2008 to March 2010 and analyzed with SPSS (version 16.0) software.
Results: Mean gestation at birth was 32 weeks (25–36 weeks). Seventy-nine percent of mothers intended to provide breastmilk exclusively. Most (68%) planned to use both breast and bottle; 11% planned to breastfeed only, and 20% to bottle feed only. At 1–2 weeks after discharge (mean 39 weeks adjusted age) mothers were pumping five times per day, producing a mean of 830 mL/day; 79% were providing 100% breastmilk using a combination of fresh and frozen milk. Mothers were directly breastfeeding twice a day. At 2–4 weeks after discharge (40 weeks adjusted age) mothers were pumping five times per day, producing a mean of 1,110 mL/day, although only 60% were able to provide 100% breastmilk. Galactogogue use increased slightly from 21% to 27%. Mothers continued to breastfeed only twice a day. Many mothers found providing expressed breastmilk in a bottle easier and less time consuming.
Conclusion: By 1 month after discharge with lactation support, these mothers of preterm multiples were able to provide a substantial proportion of breastmilk, although only 60% were able to give breastmilk exclusively.
Funding: UCSD Medical Center and Division of Neonatology, Rest Haven Children's Health Fund.
BurtonVera JoannaM.D., Ph.D.*FalckAlisonM.D.
University of Maryland, Baltimore, MD
23. Current Practices and Perceptions of Breastfeeding Support in a Neonatal Intensive Care Unit
Background: There are known barriers to initiation of breastfeeding in the hospital and additional barriers in preterm infants. Establishment of consistent breastfeeding in our neonatal intensive care unit (NICU) has not been very successful.
Objective: Concerned with the low number of infants receiving breastmilk in our NICU at time of discharge, we worked to gain insight into practices regarding initiating human milk feedings.
Methods: A Likert scale survey was distributed to all neonatal nurses twice, 6 months apart. Means and SDs were calculated. A checklist demonstrating various supports was also collected.
Results: Initial survey results indicated that the staff provides moms with information and encouragement to initiate human milk feeding. Fewer nurses endorsed statements regarding knowing contraindications to breastfeeding, providing kangaroo care, and timeliness of lactation consults. Nurses endorsed variation in support provided by the residents, attending physicians, nurse practitioners, and nurses. Checklist showed that of the 14 mothers who indicated desire to breastfeed, 12 initiated pumping within 48 hours. Results from the subsequent survey were very similar to the initial survey.
Conclusions: NICU nursing perception did not change substantially over the 6 months between the two surveys. Responses to both surveys indicated that the staff feels we provide breastmilk whenever possible. Overall, the staff felt that the NICU supported human milk feedings; however, there were differences in both surveys regarding level of support provided. Other areas where nurses were less comfortable were the contraindications to breastfeeding, kangaroo care, and timing of lactation consults. Practices continue to be evaluated for areas to improve.
FoglemanApril DanielleM.S.1*AllenJonathan C.Ph.D.1SakamotoPaulineM.S.2CohenRonald S.M.D.23
Food, Bioprocessing and Nutrition Sciences, North Carolina State University, Raleigh, NC
Mothers' Milk Bank, San Jose, CA
Department of Pediatrics, Stanford University School of Medicine, Palo Alto, CA
24. Calcium and Phosphorus Supplementation in Human Milk
Background: Infants born prematurely are at risk for metabolic bone disease and may need increased minerals for normal bone mineralization. In these situations, supplementation of human milk with calcium and phosphorus is common in the United States. The bioavailability of these additives has not been proven. Additionally, researchers from Denmark found that mineral supplementation in premature infants does not significantly improve long-term bone mineralization in term infants fed 200 mL/kg/day human milk.
Objectives: To study the effect of calcium and phosphorus supplementation on the digestability of protein, free fatty acids, and calcium in preterm donor human milk.
Methods: An in vitro model of the premature infant's gastrointestinal tract was developed to simulate digestion and absorption. Protein, free fatty acids, and free calcium were measured before and after in vitro digestion in milk with and without added calcium glubionate and sodium/potassium phosphate.
Results: Calcium and phosphorus supplementation did not negatively impact total protein, protein breakdown, protein digestibility, or fat breakdown. Supplemental calcium increased ionized calcium, which may replace ionized calcium lost during milk expression, storage, and processing.
Conclusions: Donor milk contains less ionized calcium than fresh human milk because it loses CO2 during expression and processing. Adding supplemental calcium increases ionized calcium in donor milk.
Funding Sources: Mothers' Milk Bank, San Jose, CA.
25. Evaluation of Breast Milk Composition using the Near Infrared Analyzer (NIRA)
Background: Data suggest that expressed breastmilk (EBM) provided to preterm infants should be fortified with human milk fortifier to improve short-term growth and long-term development. Meanwhile, it was demonstrated that composition of EBM varies by (not exclusive) maternal diet, gestational age, time of the day milk is expressed, and fore versus hind milk.
Objective: This ongoing study aims at finding out whether the near infrared analyzer (NIRA) (Unity Scientific) provides a fast (25 seconds) and reliable method to measure fat, protein, carbohydrates, and caloric content of EBM.
Methods: Mothers delivering prematurely signed consent and were asked to bring 4 mL of breastmilk expressed on the day of complete gestational age. The milk was divided by the mother into AM and PM, with each sample further divided to fore and hind milk. The following parameters were measured: fat, carbohydrates, protein, and calories/ounce.
Results: We found that only 20% of the samples contained 19–21 calories/ounce, with few containing more but most (56%) containing less than 18 calories/ounce. Concomitant measurements of samples using conservative methods confirmed that the NIRA results were within SD, which enables using the results for adjusting the fortification of EBM. The accuracy applied to all parameters tested.
Conclusions: Measuring composition of EBM with NIRA is reliable, fast, and inexpensive. Using NIRA in the neonatal intensive care unit will enable fortifying EBM according to the milk's composition at each feeding, adjusting it to the specific needs of each infant. This will enable to provide adequate nutrients even before deficiency is suspected by delayed growth.
LussierMary1*MarinelliKathleen A.M.D., FABM12
Neonatology, Lactation, Connecticut Children's Medical Center, Hartford, CT
University of Connecticut School of Medicine, Farmington, CT
26. Donor Milk in the First 28 Days of Life in Very Low Birth Weight (VLBW) Babies: How Much is Really Needed?
Background: Recent data demonstrate an entirely human milk diet provides best protection against necrotizing enterocolitis in the very low birth weight (VLBW) population. Since not all these mothers provide all needed milk, supplemental donor milk (DM) is required to provide this exclusive human milk diet. Concern continues over cost of DM as supplement or replacement to mothers' own milk (MOM).
Objectives: Compare enteral feedings in VLBW babies to neonatal intensive care unit (NICU) feeding protocol; determine amount of DM needed to provide all-human milk diet in the first 28 days of life.
Methods: From October 1, 2009 to March 31, 2010 (6 months), all babies admitted to Connecticut Children's Medical Center NICU ≤1,500 g were entered into this observational study. Daily enteral intake, weight, and nothing by mouth (NPO) status were recorded.
Results: Thirty-six babies ≤1,500 g admitted (four excluded—two died, two out-born); n = 32; mean gestational age 27.2 ± 2.5 weeks; mean body weight 0.976 ± 0.28 kg. Per protocol, first feeds to begin <48 hours, unless meeting specific NPO criteria. Mean time to first feed: 79 ± 62 hours; held for two babies “waiting for MOM.” Forty-seven percent received only MOM; 9% only formula; 37.5% mixed (50% of “mixed” received ≥89% MOM); 12.5% DM. Twenty-two of 27 mothers expressing milk with no contraindications provided an average 91% of MOM. Estimated cost to supplement DM to 70 VLBW babies born per year for these and entire feeds for those with no MOM, through 10 weeks of age, is $20,932/year ($4/oz).
Conclusions: First month actual feeding times/volumes vary significantly from protocol. The majority of VLBW mothers provide most of the milk needed in first 28 days. Feedings are held “waiting for MOM.” Cost of DM as bridge for mothers expressing and as sole source of milk for remaining is not prohibitive.
GeraghtySheela R.M.D., M.S., FABM1*HeierJulie E.2RasmussenKathleen M.Sc.D.2
Center for Breastfeeding Medicine, Cincinnati Children's Hospital Medical Center, Cincinnati, OH
Division of Nutritional Sciences, Cornell University, Ithaca, NY
27. Got Milk? Sharing Human Milk Via the Internet
Background: Women in the United States extract milk from their breasts by mechanical means. A woman with extra milk may sell it via the internet.
Objective: To recognize the practice by which raw, unpastuerized human milk has become a valued commodity and readily can be obtained via the internet.
Methods: A variety of easily accessible internet links can be found by entering “breast milk” or “human milk” into an internet search engine along with another descriptor such as “buy, purchase, sell, want, for-sale, or share.”
Results: Multiple internet sites exist in which human milk is available to purchase. For example, the site www.onlythebreast.com/ boasts itself as “A Community for Moms to Buy and Sell Natural Breast Milk.” The site milkshare.birthingforlife.com/ advertises itself as an “informational resource” connecting families. The site www.breastmilkdonations.com/ describes how to pasteurize milk in one's kitchen, and breastmilkmonger.com/ provides a primer entitled “How to Avoid Legal Issues” when selling human milk. Searches through classified advertising such as www.isell.com/, www.bst.com/, www.oodle.com/, and www.sell.com/ yield multiple opportunities to buy and sell human milk. The buyer simply assigns the milk into the “Add to Cart” function and pays by credit card or PayPal™ payments. Shipping costs are included. There are no options for “returns.”
Conclusions: The public health implications of human milk buying/selling are entirely unknown. The “milk” that the buyer gets is an unregulated, untested commodity. This practice is not advocated by any health organization. Collaboration between clinicians and researchers is essential to understand the risks involved in this practice.
Funding: NIH K23ES014691 (S.R.G.) and USDA/Hatch 399-7427 (K.M.R.).
WachmanElisha M.M.D.1*ByunJohnB.A.2PhilippBarbara L.M.D., FABM3
Boston Combined Residency Program at Boston Medical Center and Children's Hospital Boston, Boston, MA
Boston Medical Center, Boston, MA
Boston Medical Center, Boston University School of Medicine, Boston, MA
28. Breastfeeding Rates among Mothers of Infants with Neonatal Abstinence Syndrome
Background: Women who struggle with drug addiction during pregnancy are perhaps the most vulnerable of new mothers and may particularly benefit from all that breastfeeding has to offer.
Objective: To determine breastfeeding rates among opioid-dependent women giving birth in a Baby-Friendly hospital.
Methods: We performed a retrospective chart review of infants born at Boston Medical Center with a diagnosis of neonatal abstinence syndrome between July 2003 and January 2009. Breastfeeding eligibility was determined by negative human immunodeficiency virus status, no illicit drug use in the third trimester, and a negative urine toxicology screen on admission to labor and delivery. Feeding information was extracted from the bedside flow sheets. Breastfeeding was defined as the consumption of any amount of breastmilk within a 24-hour period.
Results: Of 276 mother–infant dyads were identified, 92% of the mothers were taking methadone (average daily dose 84.2 mg); 8% were on buprenorphine (12.6 mg). Forty percent of mothers carried one or more psychiatric diagnoses; 24% were taking two or more psychiatric medications. The average length of stay for the babies was 22.8 days. Sixty-eight percent (187 of 276) of the mothers were eligible to breastfeed. Of that group, 24% (n = 45) breastfed to some extent during the hospitalization. Eighteen of the 45 (40%) were still breastfeeding on the day of discharge. The 27 who stopped before discharge breastfed for an average of 5.88 days.
Conclusions: Breastfeeding rates among a cohort of opioid-dependent women were low, with three-quarters of those eligible electing not to breastfeed. Of those who did initiate, 60% stopped within 1 week.
BetzoldChristineMSN12*DeNicolaGreggM.D.34
The Breastfeeding Institute of Caduceus Medical Group, Yorba Linda, CA
Children's Hospital of Orange County, Orange, CA
California Faculty, University of Irvine, Irvine, CA
Caduceus Medical Group, Laguna Beach, CA
29. Microbial Evaluation of Nipple and/or Burning Breast Pain During Lactation: A Review of the Evidence
Background: Despite over 50 years of case reports of mothers experiencing burning breast pain, controversy about the etiology persists. One reason for the controversy is the lack of objective finding associated with deep breast pain.
Objective: To review the literature, summarize the results, and identify possible explanations for the etiology and lack of objective findings.
Methods: Medline was searched using multiple terms in conjunction with breastfeeding and lactation, including burning pain, breast pain, ductal infections, thrush, moniliasis breast, Candida, mammary candidosis, candidiasis, mastitis, ductal candidiasis, nipple pain, and mammary ducts. Reference lists were also reviewed. Case control, cohort, and randomized studies were included with retrospective and prospective designs. Study results for nipple and breast infections were sorted and placed in tables with their results.
Results: Seven studies were identified, and all except one had findings in the symptomatic group that indicated higher levels of microbes in the milk and/or nipple irrespective of the method used for detection. Higher levels were also found irrespective of the type or number of microbes (bacterial, fungal, or candidal) being studied. Explanations for the lack of objective findings included a case report that suggests small-colony variants may be responsible and the recent evidence that mixed-colony biofilms can occur on mucous membranes. Small-colony variants and biofilms present similarly and cause chronic low-grade infections that are difficult to detect.
Conclusions: Studies persistently find evidence consistent with infection when mothers complain of deep breast pain and/or nipple pain. Explanations exist for the lack of objective findings.
LunneyKevin M.M.D., Ph.D., MHS12*IliffPeterM.D.2MutasaKuda2NtoziniRobert2MagderLaurence S.Ph.D., M.S.3MoultonLawrence H.Ph.D.4HumphreyJean H.Sc.D., MSPH14
Department of Emergency Medicine, University of California, San Francisco, Fresno, CA
ZVITAMBO Project, Harare, Zimbabwe
Department of Epidemiology & Preventive Medicine, Maryland School of Medicine, Baltimore, MD
Department of International Health, Bloomberg School of Public Health, Baltimore, MD
30. Mastitis Increases Risk of HIV Breastfeeding-Associated Transmission, But only when Maternal Plasma HIV Load is High
Background: Exclusive breastfeeding is protective against postnatal transmission of human immunodeficiency virus (HIV) compared to mixed breastfeeding. Accordingly, exclusive breastfeeding for 6 months is the World Health Organization's recommendation to HIV-infected mothers for whom exclusive replacement feeding is not acceptable, feasible, affordable, safe, or sustainable. The mechanism of exclusive breastfeeding protection is unknown, but is hypothesized to be mediated through reduced mastitis.
Objective: To test the hypothesis that the association of exclusive breastfeeding with reduction of transmission is mediated through a reduction in subclinical mastitis.
Methods: We compared breastmilk and plasma specimens of exclusive breastfeeding and mixed breastfeeding HIV-positive mothers archived from the ZVITAMBO trial in which mixed breastfeeding was associated with a twofold increased risk of postnatal transmission at 18 months. Plasma HIV load, breastmilk HIV load, and sodium/potassium ratio as a proxy for (subclinical) mastitis were measured.
Results: Mixed breastfeeding was not associated with mastitis or breastmilk HIV load. Mastitis was associated with breastmilk HIV load, and this effect increased with increasing maternal plasma HIV load; mastitis was associated with postnatal transmission only when maternal plasma HIV load was high (>3.7 log10). Initiation of breastfeeding within an hour of delivery was associated with exclusive breastfeeding (adjusted odds ratio 1.62; confidence interval 1.02–2.58).
Conclusions: Exclusive breastfeeding is associated with reduced postnatal transmission of HIV from mother to child, but this protection is not mediated by reduced mastitis or breastmilk HIV load. The deleterious effect mastitis increases as the mother's plasma HIV viral load increases.
McLeodKathrynM.D.*McCullenTeresaWilsonDonnaWoodSallyRichardsonDeborahPh.D.
Department of Pediatrics, Medical College of Georgia, Augusta, GA
31. Interdisciplinary Development of a Breastfeeding Curriculum for First- and Second-Year Pediatric Residents
Background: An increasing body of literature indicates that pediatric residents are underexposed to breastfeeding encounters, resulting in a lack of preparedness and the inability to promote breastfeeding in new mothers.
Objective: This study seeks to create a breastfeeding curriculum that teaches breastfeeding skills to residents using real breastfeeding mother–baby dyads as standardized patients.
Methods: A new curriculum was created based on the American Academy of Pediatrics residency breastfeeding curriculum and Wellstart International modules. An education intervention for first-year pediatric residents was developed using an actual breastfeeding mother–baby dyad to teach breastfeeding skills. Objective structured clinical examination (OSCE) cases were created for the second-year residents to model three of the most common breastfeeding problems pediatricians encounter: sore nipples, jaundice, and perceived poor milk supply. The curriculum will be assessed by testing pre-intervention knowledge and attitudes and post-test attitudes (i.e., comfort with providing breastfeeding guidance to new mothers). Standardized patients will use a communication checklist to give general feedback to residents, and videotaped OSCE sessions will be evaluated by breastfeeding experts. Specific case-related checklists were created to give more informative feedback to residents about their ability to assess and interact with breastfeeding mothers.
Results: The breastfeeding curriculum used by the pediatric residency including three breastfeeding-specific OSCEs will be presented.
Conclusions: This breastfeeding curriculum can be adapted for use by other institutions to teach breastfeeding skills to all levels of physicians and nursing staff. Participation in the curriculum will lead to improved knowledge about breastfeeding and the ability to more actively promote breastfeeding in new mothers.
Funding: Educational Discovery Institute (MCG start-up grant).
ShockleyRachelD.O.
Community Health Network Family Medicine Residency, Indianapolis, IN
32. Assessing Our Learners Concerning Lactation: An Osce
Background: Education on breastfeeding is often limited during a family medicine resident's training. Healthy People 2010 sets breastfeeding goals that we nationally do not reach. A longitudinal lactation curriculum that uses an objective structured clinical examination (OSCE) as an evaluation tool was created to help assess family medicine resident education in lactation.
Objective: The resident will show improved knowledge on a post-test compared to a pre-test after completing a lactation OSCE.
Methods: A 12-question pre-test and post-test were given in conjunction with the OSCE to assess the knowledge acquisition of residents concerning lactation.
Results: Nineteen residents completed the pre-test and post-test. Eighteen of the nineteen improved their scores from the pre-test to the post-test.
Conclusions: OSCEs provide a way to assess resident skills in counseling a breastfeeding patient and in the process teach basic lactation knowledge. OSCE is as a good method to measure curricular outcomes and can be implemented into a lactation curriculum. Using OSCE in resident education has several benefits and challenges.
BetzoldChristineMSN12*DeNicolaGreggM.D.34
The Breastfeeding Institute of Caduceus Medical Group, Yorba Linda, CA
Children's Hospital of Orange County, Orange, CA
California Faculty, University of Irvine, Irvine, CA
Caduceus Medical Group, Laguna Beach, CA
33. Progestin-Only Contraception During Lactation: A Re-Analysis
Background: The progestin-only contraception during lactation research is generally of a poor quality, and the findings are inconsistent both within the body of evidence and with the persistent maternal reports of supply decreases.
Objective: To determine if applying six quality criteria to grade progestogen-only contraception during lactation research clarifies the reasons for the inconsistencies.
Methods: Studies (n = 24/38) from a recently published systematic review were separated, categorized, and then analyzed using charts. Statistically significance evidence and the criteria were defined. Category 1 comprised studies with statistically significant evidence of milk supply decreases (a) with or without breastfeeding definitions and (b) with breastfeeding definitions. Category 2 comprised studies with statistically significant evidence of milk supply increases (a) with or without breastfeeding definitions and (b) with breastfeeding definitions. Category 3 comprised studies with breastfeeding definitions and equivalent or conflicting evidence. Inclusion criteria included evaluation of maternal milk supply and comparison to a non-hormonal control. Exclusion criteria included poor statistical analysis, duplication of data, and equivocal findings in a study without breastfeeding definitions.
Results: Mean scores in Category (1a) 4.67 (n = 6) and (1b) 5.0 (n = 5) were higher than those in Category (2a) 1.66 (n = 6) and (2b) 1.0 (n = 2) and Category (3) 2.92 (n = 12). Category 1 studies were consistently superior to Categories 2 and 3 for all six criteria.
Conclusions: Studies that scored five or six consistently found decreases in milk supply. Analysis of studies using these criteria provides an explanation for the inconsistencies. Mothers should be informed that progestins can lower milk supply.
TewariDeepaliM.D.1*TewariVirendraM.D.2BaptisteJeanM.D.1KimRogerM.D.1SakowitzSherryM.D.1SokalMyronM.D.1
Brookdale University Hospital, Brooklyn, NY
Interfaith Medical Center, Brooklyn, NY
34. Barriers to Breastfeeding in a Predominantly African-American Population
Background: A recent study conducted at our institute reported breastfeeding rates of 1.9% exclusive and 35% formula with breastfeeding among newborns.
Objective: Since breastfeeding rates were far below the Healthy People Goal of 75% we designed this study to explore why women chose not to breastfeed in our hospital population.
Methods: One hundred fifty-two new mothers and 43 healthcare providers were interviewed from March 1 to July 30, 2009 using a structured questionnaire.
Results: Responses are presented as number/percentage: against breastfeeding, inadequate for nutrition and weight gain of baby 148/97.4%, interferes with mother's physical appearance and freedom 148/97.4%, uncomfortable and weird 134/88%, breast and nipple problems 126/82.9%, interferes with partner relationship 94/61.8%; in favor of bottle feeding, convenient, baby sleeps longer with better weight gain 152/100%, healthier than breastmilk 143/94%; social barriers, enrolled in Special Supplemental Nutrition Program for Women, Infants and Children (WIC) 152/100%, cultural practice 149/98%, day care may not keep baby if breastfeeding 127/83.5%, perceived embarrassment and social isolation 108/71.1%, lack of support from male partners 31/20.4%, knowledge of breastmilk storage methods 3/1.9%; and organizational barriers, practice breastfeeding promotion daily 4/9.3%, feel unconfident in supporting breastfeeding mothers 39/90.7%, early newborn transfer to nursery interferes with breastfeeding 40/93%, need for extra staff as lactation consultant 41/95.4%, lack of structured in-hospital breastfeeding promotion 42/97.7%, feel motivating mothers for breastfeeding is too time consuming and formal, training is needed to support breastfeeding 43/100%.
Conclusions: We recommend initiating a breastfeeding promotion program addressing the major barriers identified in our study and to evaluate WIC's strategy of supplying free formula to babies without medical reasons.
WilliamsJanetM.D.GongAlice K.M.D.*GillSara L.Ph.D.
University of Texas Health Science Center at San Antonio, San Antonio, TX
35. Baby Steps: Perceptions of Breastfeeding among Low-Income Hispanic Women and their Medical Providers
Background: Although professional medical organizations recommend breastfeeding as the optimal source of infant nutrition, little is known about how clinicians provide breastfeeding information to pregnant women and their families during the prenatal period.
Objective: Explore healthcare providers' and pregnant women's perceptions of breastfeeding support during the prenatal period.
Methods: Fourteen focus groups with 63 participants from the San Antonio and Austin, TX metropolitan areas served as a convenience sample of low-income, pregnant Hispanic women. Open-ended questions guided the discussion. Data analysis involved the long-table approach of clustering similar responses to identify behavior, attitude, and belief patterns.
Results: Pregnant women received health information from clinics' medical personnel. The breastfeeding decision was made during pregnancy by 80%. Mothers were influenced by medical providers 17% of the time. Medical personnel described themselves as only information providers having a lack of time, funding, training, and resources to create a breastfeeding-promoting environment. Most providers supported providing prenatal breastfeeding education, but disagreed about when and how to educate. Prenatal clinic personnel described their confidence about providing breastfeding education as “based only on personal experience,” but desired more breastfeeding education and knowledge.
Conclusions: The medical provider role in breastfeeding promotion is not yet optimized, but should improve through comprehensive breastfeeding training, engaging prenatal care patients and families with breastfeeding-educational and supportive resources, and postpartum follow-up. Coordination with governmental agencies might influence breastfeeding rates by diminishing economic incentives promoting baby formula use. Highlighting breastfeeding benefits, providing expanded training, and including cultural context are key breastfeeding promotional strategies.
Funding: Texas Department of State Health Services.
PowersNancy G.M.D., FABM*ParhamDouglas F.Ph.D.GoldbergLynPh.D.
Wichita State University, Witchita, KS
36. Newborn Infants' First Cries During Separated and Non-Separated Conditions
Background: Despite the documented adverse effects of separation, routine childbirth practices in many hospitals continue to move the newborn away from the mother immediately following birth. The resultant crying is often interpreted as “good for the baby's lungs.”
Objective: Determine whether a distinct separation distress cry can be identified during the first 2 hours of life in healthy human neonates, as has been identified in many other animal species, objectifying the stress/distress of separation.
Methods: In an observational study, healthy women and infants were audio- and videotaped for 2 hours immediately following delivery. Differences in care were those that occurred as a routine part of hospital labor and delivery. Recording equipment placed in a standardized location was activated when the mother received the baby or when the baby was stable (if separated). Crying events could be identified as occurring during separation or non-separation and then analyzed for duration, intensity, perceptual qualities, and spectral characteristics.
Results: Analysis of recordings of two dyads completed to date has identified distinct acoustic differences between cries occurring during skin-to-skin contact and those during separation.
Conclusions: Findings support earlier speculation regarding a separation distress cry and provide additional impetus for sustained skin-to-skin contact immediately following birth.
Funding: Supported by Office of Research Administration, Wichita State University, grants U10099 and D10978.
WatkinsStephanieMSPH, MSPT1*Meltzer-BrodySamanthaM.D., MPH2ZolnounDennizM.D., MPH2StuebeAlisonM.D., M.Sc.2
Gillings School of Global Public Health, University of North Carolina, Chapel Hill, NC
School of Medicine, University of North Carolina, Chapel Hill, NC
37. Early Breastfeeding Experience and Postpartum Depression: A Longitudinal Study
Background: Postpartum depression is a common and potentially devastating condition that is associated with shortened breastfeeding duration.
Objective: We sought to measure the association between early breastfeeding experience and maternal mood at 2 months postpartum.
Methods: We used logistic regression to evaluate the association between early breastfeeding experience and maternal mood, quantified with the Edinburgh Postnatal Depression Scale (EPDS), among women who initiated breastfeeding in the Infant Feeding Practices Survey II. Women reported their early breastfeeding experiences at 1 month, and they completed the EPDS at 2 months.
Results: In the neonatal period, 2,586 women reported ever breastfeeding, among whom 223 (8.6%) met criteria for major depression (EPDS ≥13) at 2 months postpartum. Women who reported disliking breastfeeding in the first week were more likely to meet criteria for major depression at 2 months (odds ratio [OR] 1.42, 95% confidence interval [CI] 1.04–1.93), adjusting for maternal age, parity, education, ethnicity, and postnatal Women, Infants, and Children participation. We also found that women who were depressed were more likely to report severe breastfeeding pain in the first day (adjusted OR 1.96, 95% CI 1.17–3.29, vs. no pain), the first week (adjusted OR 2.13, 95% CI 0.74–6.15, vs. no pain), and the second week (adjusted OR 2.24, 95% CI 1.18–4.26, vs. no pain).
Conclusions: Women who disliked breastfeeding or experienced severe pain in the neonatal period were more likely to have depressive symptoms at 2 months postpartum. Early breastfeeding difficulties may identify a subgroup of women at high risk for postpartum depression.
Rivera-TodaroLeaMPhil*NobleLawrenceM.D.
Mount Sinai School of Medicine, Elmhurst Hospital Center, Elmhurst, NY
38. Utility of Screening for Postpartum Depression During Lactation Support
Background: Postpartum depression is the most common problem that new mothers face, affecting 10–20%. Low-income urban mothers are at greatest risk. Although effective treatment is available, fewer than half are recognized. Current recommendations include screening at various healthcare settings.
Objective: To test the efficacy of screening for postpartum depressive symptoms at an inner-city lactation clinic.
Methods: The Patient Health Questionnaire-2 was administered to 65 women in a 4-month period at their initial visit in a lactation clinic. A low cutoff score of ≥1 was used in this study because of the brevity of time between birth and screening (mean = 10 days). This low cutoff score has a sensitivity of 98% and a specificity of 59%. Data were analyzed by χ2.
Results: Thirteen percent of the mothers (n = 9) screened positive for depressive symptoms. The incidence of depressive symptoms was greater in those who presented with breast pain than other symptoms (50% vs. 10%, p = 0.038). Depressed patients with breast pain were all Mexican.
Conclusions: We conclude that those providing lactation support can provide an additional point of access to mental health services and that, in our population, the incidence of depressive symptoms was significantly greater in those who presented with breast pain. We speculate that Mexican women may somatize emotional distress or that the stress of breast pain may cause similar symptoms as depression. Therefore, any patient with symptoms of postpartum depression and presenting with breast pain should be rescreened after the symptoms of pain resolve.
YamauchiYoshitadaM.D.1*KageyamaMisaoM.D.2NakamuraMakotoM.D.2NakamuraKazueM.D.2TadaKatsuhikoM.D.3
The Japan Breastfeeding Association, Okayama Medical Center, Okayama, Japan
Division of Neonatology, Okayama Medical Center, Okayama, Japan
Department of Obstetrics, National Hospital Organization, Okayama Medical Center, Okayama, Japan
39. Factors Affecting the Prolonged Jaundice in Full-Term, Breastfed Infants
Background: World Health Organization/UNICEF recommends exclusive breastfeeding for the first 6 months. However, it is well known that incidence of hyperbilirubinemia increases and jaundice also continues for a long period in breastfed infants.
Objective: To determine factors affecting the prolonged jaundice and also whether the prolonged jaundice has effects on weight gain and breastfeeding rate at 1 month.
Methods: Healthy, full-term, breast-fed Japanese neonates without phototherapy (n = 178) were recruited for this study. Although all infants were breastfed at time of discharge from the hospital, some infants were supplemented with 5% glucose water during the hospital stay. Infants born vaginally usually discharged on day 5–6, but infants born by cesarean section on day 10 after birth. Factors affecting the serum bilirubin levels and breastfeeding rate at 1 month were evaluated. The total serum bilirubin level was assessed using a transcutaneous bilirubinometer (TcB) (model JM-103).
Results: We found the significant correlation between peak TcB on the sternum during the first week of life and TcB at 1 month (r = 0.36, p < 0.01, n = 178). TcB in supplemented infants (n = 41) was significantly lower than that of exclusively breastfed infants (n = 137) at 1 month. TcB at 1 month also correlated significantly with gestational age (r = −0.32, p < 0.01) and supplementation (r = −0.26, p < 0.05), but not weight gain per day after discharge from hospital.
Conclusions: Exclusive breastfeeding relates to prolonged jaundice, but weight gain may not influence the bilirubin levels at 1 month. Our study also suggests that the mother's age and degree of infant's weight loss in early days of life may significantly influence the breastfeeding rate at 1 month.