
Abstract
Abstract
Background and Aims:
Human milk bank is a source of human milk supply in many neonatal intensive care units. However, there are some hospitals without this facility because of financial or religious impediments, such as the Muslim community.
Methods:
We introduced human milk donation as an alternative to human milk banking based on Islamic principles. The suitable donor is a healthy rooming-in mother whose expressed breastmilk is in excess of her baby's demand. The milk is used after 72 hours of freezing at −20°C. The donor must fulfill the criteria for selection of donors and be nonreactive to human immunodeficiency virus and syphilis. Once the recipient's family and the donor state their desire for the human milk donation, a meeting with both parties is made. Unpasteurized frozen–thawed donor's milk will be provided to the recipient after written consents are obtained from both parties.
Results:
This study was carried out in the Duchess of Kent Hospital (Sandakan, Sabah, Malaysia) between January 2009 and December 2010. A total of 48 babies received donated breastmilk. Forty-two infants were from the special care nursery, and the remaining six were from the pediatric ward. Eighty-eight percent of the donors and 77% of the recipients were Muslims. Sixty percent of the infants who received donated human milk were premature. Two infants died because of the underlying nature of their disease.
Conclusion:
Human milk donation is an option for hospitals without a human milk bank or in the Muslim community.
Introduction
Necrotizing enterocolitis (NEC) and late-onset septicemia remain the two most important causes of death and morbidity among premature infants. In preterm and low birth weight infants, feeding with formula milk compared with donor breastmilk results in a higher risk of developing NEC. 2 NEC affects close to 10% of infants who weigh less than 1,500 g, with mortality rates of 50% or more depending on severity. 3 In addition, a meta-analysis found that infants who received donor human milk were three times less likely to develop NEC and four times less likely to have confirmed NEC than infants who received formula milk. 4
Some studies also reported that the incidences of any infection, sepsis/meningitis, and retinopathy of prematurity are significantly reduced in human milk–fed very low birth weight infants compared with exclusively formula-fed very low birth weight infants.5,6
Moreover, the developmental outcome of an extremely low birth weight premature breastmilk-fed baby is better than that of an infant formula-fed baby. 7 Preterm infants fed solely on standard formula had significantly lower developmental scores at 18 months than those fed on donor breastmilk. 8
Wet nursing is not a widespread practice in Malaysia as it once was, especially since the introduction of commercial formula. It is difficult to practice in neonatal intensive care unit settings. Also, there is no established human milk bank in Malaysia as such a practice is considered to be unethical in a predominantly Muslim society because of the concept of “Mahram.”
According to the Holy Quran, wet nursing makes one a “Mahram”; this means that the woman who provides her breastmilk for a baby is considered to be maternally related to the baby. The baby, therefore, would be considered the donor's child. Marriage between the recipient of the donor milk and the offspring of the donor is forbidden.
However, human milk banks as practiced in most western countries use pooled donor milk. The anonymity of both the donor and recipient is maintained. This indicates there is a possibility of marriage between the recipient and the donor's offspring in the future, which is strictly prohibited in Islam.
The Council of Islamic Fiqh Academy prohibited the establishment of milk banks in the Islamic world or of feeding a Muslim child with milk from a milk bank. 9 No “Fatwa” (religious edict) in Malaysia supports setting up of such institution or even with pasteurization. Consequently, we introduced human milk donation in the neonatal Special Care Unit (SCN) of the Duchess of Kent Hospital, a district hospital in Sandakan, Sabah, Malaysia. We conducted this study to assess the feasibility of human milk donation in a predominantly Muslim society.
Subjects and Methods
The practice of human milk donation in the SCN of the Hospital was approved by the Ethic Committee of the Duchess of Kent Hospital. Signed written consents were obtained from both the donor and the recipient's parents.
There are 6,000 deliveries a year in this hospital. The population served by the SCN of the Duchess of Kent Hospital comprises 65% Malaysians and 35% non-Malaysians, immigrants mainly from the Philippines and Indonesia. About 23% of the Malaysians in Sabah and most of the non-Malaysians fall below the poverty line.10,11
The majority of the sick infants were able to receive their mother's breastmilk in the SCN. However, there was still a small group of premature or sick babies whose mothers were unable to provide enough breastmilk owing to various reasons such as insufficient milk, the mother was receiving chemotherapy, or maternal death.
Collection of human milk
All mothers whose babies are admitted to the SCN are encouraged to stay in rooming-in wards. In order to minimize bacterial contamination, mothers are asked to wash their hands before expression of milk. Milk is expressed directly into autoclaved glass bottles and used for only one expression. They are covered up with plastic wrap and secured with a rubber band. The mother is asked to label each bottle with her name and date of expression.
Storage of human milk
All expressed breastmilk is stored in a freezer at −20°C. The freezer does not have a self-defrosting cycle. The temperature of the freezer is monitored every 8 hours. The freezer has an immediate back-up power supply during a power outage. All frozen milk is thawed before use.
Human milk donation process
Mothers who are not able to produce sufficient milk for their babies would be counseled on human milk donation prior to introducing breastmilk substitute.
Counseling
The parents of the recipient are provided evidence-based information about the benefits of feeding with human milk as well as the risks associated with infant formula feeding, including a higher rate of NEC, late-onset sepsis, retinopathy of prematurity, and poorer development outcomes. The risks of using donated human milk, the process of donor screening, and the use of frozen–thawed milk are explained thoroughly. During the counseling, the religious implications of human milk donation in Islam and a brief background of the potential donor will be provided. Only after this extensive counseling session is done will the parents make an informed choice with regard to their child's feeding.
Selection of donor
The donor is identified as a rooming-in mother whose expressed breastmilk is in excess of her baby's demand. The milk will only be used after being frozen at −20°C for a minimum of 72 hours. The donor will undertake the screening tests for human immunodeficiency virus (HIV) and syphilis. Once the results are known to be negative, the donor will be asked for approval to participate in human milk donation.
A woman who smokes, ingests alcohol, or is receiving medication that is contraindicated in breastfeeding is refused as a donor. The donor must (a) be healthy and well nourished, (b) have no history of blood transfusion, tattoo, jaundice, or chronic cough, (c) have no history of high-risk behavior, (d) have no history of cracked nipples, and (e) be nonreactive for HIV and syphilis (screening is not done for cytomegalovirus [CMV], human T-cell lymphotrophic virus-1 [HTLV-1], and hepatitis B and C viruses).
A meeting with both parties
Once the donor and the recipient's parent agree to human milk donation, a meeting for both parties will be arranged. This meeting fulfills the religious obligation that the donor knows the parent of the recipient. The religious implications are once again reinforced to both parties.
Consent and documentation
As soon as both parties agree to the donation and understand the religious implications, they will be asked to provide a signed consent giving their authorization for the human milk donation to proceed. The names and religion of both parties will be documented in the infant's medical record and in the human milk donation chart. The chart enables us to trace the donor to the recipient and from the recipient back to the donor. There is no compensation given or collected for this process.
When all the processes are completed, the unpasteurized frozen–thawed donor's milk will be provided to the recipient.
Results
There were 2,415 infants admitted to the SCN between January 2009 to December 2010. Of these admitted infants, 97.82% were exclusively fed with their mother's milk, 1.72% (n=42) received human milk donation, 0.29% (n=7) were given mixed feeding with infant formula when there was no available donor, and 0.17% (n=4) were fed with breastmilk substitute because the mother was HIV-infected as per the Malaysia HIV infant feeding policy.
One mother of very low birth weight premature triplets rejected human milk donation because of religious reasons at the early phase of the program. However, she was subsequently able to produce sufficient amounts of milk following lactation support.
Figure 1 illustrates the total number of human milk donors and recipients. Of the 50 human milk donors, 44 were healthy rooming-in mothers, and six were relatives of recipients as requested by the recipient's parent. All fulfilled the criteria for selection of donor. In total, 48 babies received donated breastmilk: 42 infants were from the SCN, and the remaining six were from the pediatric ward. Two infants died because of the underlying disease, which was not related to human milk donation. One had drowned and had no signs of life on arrival at the hospital. He was revived following resuscitation but pronounced dead 1 week later after he was certified to be brain dead. The other deceased infant had severe pneumonia with Acinetobacter septicemia.
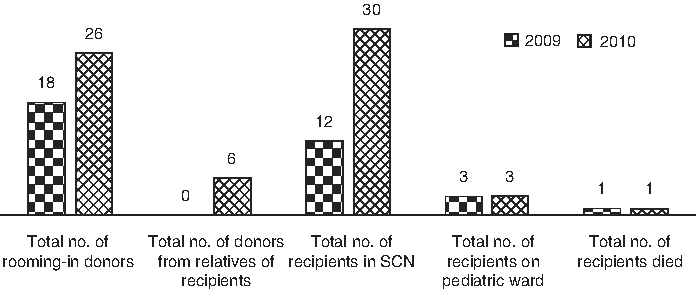
Total numbers of human milk donors and recipients. SCN, Special Care Nursery.
As shown in Figure 2, the majority of the donors or recipients were Muslims.

Distribution of religions among human milk donors and recipients.
Figure 3 shows that premature infants (25 of 44) were the leading group of babies received donated milk.

Distribution of disease among human milk recipients. MAS, meconium aspiration syndrome.
Seventy percent (32 of 46) of the recipients were discharged being exclusively breastfed or breastfed with cup feeding of expressed mother's milk, whereas 30% (14 of 46) were discharged with infant formula or mixed feeding. No donated milk was provided after discharge.
Discussion
Banked human milk is an important alternative for the care and treatment of premature and sick babies. However, feeding with raw human milk has raised the concern of infection. Two methods have commonly been used in order to reduce the risk of infection: pasteurization and/or donor screening for HIV, syphilis, hepatitis B virus, hepatitis C virus, CMV, and HTLV-1, which are currently being practiced in North America, Kuwait, 12 India, 13 and Norway. 14
Other herpesviruses, parvovirus, hepatitis A, B, and C viruses, and rubella virus are often demonstrated in breastmilk, but transmission is very rare. The highest risk is during an acute infection at the time of birth. 15
Most human milk banks use Holder pasteurization to pasteurize human milk. However, heating expressed human milk to 62.5°C for 30 minutes significantly reduces its protective effect. 16 The immunomodulatory proteins in human milk are reduced by pasteurization, resulting in decreased antibacterial capability. A stringent procedure to minimize bacterial contamination is essential during handling of pasteurized milk. 17 In our hospital, we use unpasteurized human milk not only because we do not have pasteurization facilities but also because we have difficulties in controlling the process well enough under routine clinical conditions.
Syphilis and HIV co-infection is now increasingly common. The World Health Organization recommends all wet nurses be screened for HIV as it can be transmitted through breastfeeding. 18 Therefore, all donors must undergo the screening tests for HIV and syphilis.
A CMV-seropositive mother can transmit CMV via breastfeeding. Hamprecht et al. 19 reported the transmission of CMV from mother to preterm infant by breastfeeding; four had sepsis-like symptoms. In their unit, the raw milk was refrigerated at 4–10°C for a maximum of 12 hours before feeding. However, a study by Friis and Anderson 20 has shown that freezing of breastmilk at −20°C for more than 72 hours reduces CMV titers by 99%. No evidence has yet been found in preterm neonates with neurologic sequelae and mortality related to CMV infection via breastmilk.21–24 Furthermore, Hayashi et al. 25 have reported a group of 27 extremely low birth weight premature infants fed with frozen–thawed breastmilk from CMV-seropositive mothers; CMV infection was confirmed in only one infant who displayed almost no clinical symptoms.
Freeze–thaw processing can also eliminate the HTLV-1 infectivity of breastmilk. 26
There was a span of 1 month before the CMV and HTLV-1 results became available in our hospital. During the waiting period, there might be a shortage of milk for the baby. The same problem was faced in Kuwait breastmilk donation. 12 Therefore, we use freeze–thawed human milk to reduce the risk and the severity of CMV and HTLV-1 infection.20,26
Breastfeeding does not carry any additional risks to infants of hepatitis B virus carriers even before the availability of hepatitis B vaccine.27,28 Active immunization with hepatitis B vaccine can prevent development of the persistent carrier state.29,30
Conflicting results about the transmission of hepatitis C virus via breastmilk have been reported.31–33
However, there are no data to suggest that hepatitis C virus is transmitted via breastmilk. The Centers for Disease Control and Prevention recommend continuation of breastfeeding to infants of hepatitis C virus–infected mothers. In spite of that, we have limited resources for screening CMV, HTLV-1, hepatitis B virus, hepatitis C virus, and herpesvirus.
The benefits of human milk donation far outweigh the much higher risk of complications from the use of infant formula and the risk of disease transmission, which can be reduced by donor screening and the freeze–thaw process.
Human milk donation follows the principle of wet nursing by introducing both parties who are made aware of the religious implications. This study shows that human milk donation is feasible and is accepted within the Muslim community. Human milk donation is also cost effective.
The total number of recipients over a 2-year period was 48. Further study and follow-up of the recipients are needed in order to monitor for evidence of disease transmission via human milk donation.
In conclusion, human milk donation is an alternative for countries without a human milk bank or in the Muslim community.
Footnotes
Acknowledgments
We wish to thank the Director General of Health, Malaysia for permission to publish this article and Dr. Wan Pauzi Wan Ibrahim for providing the note of the interview with Mufti Kelantan, Tuan Haji Datuk Mohammad Shukri Mohamad regarding the “religious implications of milk donation.”
Disclosure Statement
No competing financial interests exist.