
Abstract
Abstract
Objective:
This study compares maternal milk volumes (MMVs) of Ugandan mothers whose infants were in a special care nursery and who used one of three maternal milk expression techniques: double electric breast pump, single non-electric manual breast pump, and hand breastmilk expression.
Subjects and Methods:
A convenience sample of 161 Ugandan mothers of infants who were either too immature or ill to independently feed from the breast yet healthy enough to survive in an environment without ventilator support (birth weights, 0.84–3.8 kg) were assigned to one of three maternal milk expressions: Group 1, double electric breast pump (n = 55); Group 2, single non-electric manual breast pump (n = 59); and Group 3, hand breastmilk expression (n = 47). Data were collected over a 7-day period (from day 1 postpartum to day 7 postpartum), and mean MMVs were measured and compared among the groups.
Results:
The mean daily MMVs were as follows: Group 1, mean = 647 mL (SD = 310); Group 2, mean = 520 mL (SD = 298); and Group 3, mean = 434 mL (SD = 291). Results from one-way analysis of variance revealed significant differences in the mean MMV based on the method of maternal milk expression (p = 0.0019). Further analysis using Tukey's HSD Test revealed significant differences in the MMV between Groups 1 and 3 (p < 0.01), but not between Groups 1 and 2 or between Groups 2 and 3.
Conclusions:
Electric breast pumps provided the highest mean MMV; however, many mothers obtained adequate feeding volumes for their infants' daily nutritional needs with the single non-electric manual breast pump and hand breastmilk expression.
Introduction
The premature or sick term infant is often unable to feed directly at the breast and is at the greatest risk for infections and other neonatal illnesses. Therefore, this group receives the greatest benefit from exclusive breastmilk feeding. It is crucial to find ways to feed these infants exclusive breastmilk while in the special care nursery and beyond. Collecting mother's own breastmilk in adequate volumes to support the growth of premature and sick infants is a challenge even in developed countries with state-of-the-art equipment and resources. Mothers in developing countries often face additional challenges in providing adequate breastmilk volumes for their premature or sick infants. With limited access to equipment and resources such as adequate food, breast pumps, refrigeration, transportation, and electricity, mothers in developing countries may have difficulty providing enough breastmilk to support the needs of their infants who cannot feed directly at the breast.10,27 In earlier studies the authors observed mothers hand expressing only 5–10 mL of milk per expression session. The expressed volume was adequate for initial trophic feeds, but as feeding volumes advanced, mothers were unable to express the larger volumes needed. Maternal milk storage is limited by lack of refrigeration in most nurseries in developing countries, which further reinforces expressing only the volume necessary for feeding. Therefore, supplemental feeding with milk from other sources often becomes necessary, potentially further compromising infant health.
Breastmilk production is determined by hormonal stimuli, which is dependent on infant suckling, regular and efficient milk extraction or breast emptying, and, to some extent, the health of the mother. 1 The most common method of obtaining breastmilk for infants unable to suckle in developing countries is hand breastmilk expression, 10 which involves massage and compression of the breast to express milk into a container. 11 While it is recognized that hand expression is a low-cost method of obtaining breastmilk, there are concerns that long-term use of hand breastmilk expression may result in incomplete emptying of the breast and insufficient maternal milk volumes (MMVs) necessary to achieve optimal infant growth and development. 12 It is thought that some mothers feel discomfort during any type of milk expression, which then becomes a barrier for long-term use.13,14 Additionally, specific types of breastmilk expression may be more tedious for some mothers and may take longer than other expression methods.15,16
This study introduced Ugandan mothers of premature or sick term neonates to evidence-based milk expression techniques. One such technique is the double electric breast pump, which may help the mother stimulate milk production in the early postpartum days and provide efficient breast emptying with less discomfort. This option may be feasible in large referral nurseries with consistent electricity. However, the feasibility of electric breast pumps in areas of the world that most need them has been questioned for lack of consistent electric supply, cultural barriers, and the cost of obtaining and maintaining them. Therefore, the less expensive single non-electric manual breast pumps may be a viable alternative to double electric breast pumps. In addition, many mothers, with coaching and support, can comfortably provide adequate MMV by hand breastmilk expression alone. Where possible, this latter option should be considered and supported. However, when MMV is not adequate for appropriate weight gain in the infant, other methods of breastmilk expression need to be considered. The objective of this study was to compare MMVs of Ugandan mothers whose infants were in a special care nursery using three maternal milk expression techniques: double electric breast pump, single non-electric manual breast pump, and hand breastmilk expression.
Subjects and Methods
This study used a quasi-experimental research design. This design was used to determine MMV based on method of maternal milk expression.
The study participants included a convenience sample of 161 Ugandan mothers whose neonates were in the Special Care Baby Nursery, Mulago Hospital, Kampala, Uganda. Mulago Hospital is a national referral hospital. The Special Care Baby Nursery is a level II nursery with about 3,000 admissions per year, about half of whom are preterm. Any mother of an infant, regardless of weight, who was too ill to independently feed from the breast yet healthy enough to survive in an environment without ventilator support was eligible to be included in this study. Infants enrolled in the study had gestational age assessed upon admission to the Special Care Nursery, utilizing the New Ballard Scale of Gestational Age Assessment. 17 However, this was a new tool for the nurses working in this developing country's Special Care Nursery. Because the inter-rater reliability of the assessment was poor or the score was omitted in the data entry process, specific gestational age assessment data was not used in the data analysis.
Of the 292 mothers who were initially enrolled in the study, 131 were excluded because of death of the neonate (n = 88), death or illness of the mother (n = 3), the neonate was able to breastfeed directly from the breast prior to the end of the data collection period (n = 26), or other (n = 14). With a total of 161 study participants (≥47 in each of the three groups), a power of >0.99 was achieved, with an effect size of 0.30, at the 0.05 level of significance. 18
Forty-eight percent (n = 77) of the mothers were primigravidas, and 52% (n = 82) were multigravidas; gravida was not reported for two of the mothers. Table 1 gives a summary of demographic characteristics of the study participants, including maternal age, number of previously breastfed infants, and birth weight of the neonates. The mean birth weight of the infants was 1.46 kg, with a range of 0.84 to 3.8 kg. No significant difference was found among the three groups based on gravida, maternal age, or number of previously breastfed infants; however, a significant difference was found based on the birth weights of the neonates between Groups 1 and 2 (p < 0.01) and Groups 1 and 3 (p < 0.01) (Table 1).
Approval to conduct the study was obtained from the University of Louisville Institutional Review Board and the Makerere University Faculty of Medicine Research and Ethics Committee. Participation was voluntary, and written informed consent was obtained from the study participants prior to data collection. The consent form was available in both the Luganda and English languages. Data were collected in the language of each mother's preference.
The study participants were assigned to one of three maternal milk expression groups, using non-random, sequential assignment: Group 1, double electric breast pump (n = 55); Group 2, single non-electric manual breast pump (n = 59); and Group 3, hand breastmilk expression (n = 47). Non-random, sequential assignment was used so that all mothers were using the same method of maternal milk expression at any given point during the data collection period, reducing potential bias from study participants observing other study participants using a different method. Mothers were enrolled sequentially in groups of 20 into their assigned method of milk expression until the required number of mothers was enrolled. Each group of 20 completed their milk expression prior to enrolling another group to assure that mothers' observing another method of milk expression did not influence the results.
The electric breast pumps used in this study were Medela (McHenry, IL) Lactina® electric breast pumps with double collection kits, and the single non-electric manual breast pumps were Medela Harmony™ breast pumps with single collection kits. Medela, Inc. donated the breast pumps and milk collection kits. The electric breast pumps were registered with the U.S. Food and Drug Administration and the Underwriters Laboratories.
The nursery nurses were educated on the methods of maternal milk expression and how to measure and record MMV prior to their initiation of data collection. All study participants were taught to use their assigned method of maternal milk expression by nursery nurses. Mothers were instructed to begin milk expression within 2 hours of delivery and to continue to express milk every 2 hours for a duration of at least 15 minutes or until 2 minutes beyond the time the mother stopped seeing milk. Study participants were taught to completely empty each breast at each pumping or expression session.
MMV were measured to the nearest milliliter and recorded at each pumping session. Data were collected for each study participant over a 7-day period, beginning on postpartum day 1 and extending through postpartum day 7.
Data were analyzed using the Statistical Analysis Software version 9.1 package (SAS Institute, Cary, NC). Data analysis included descriptive statistics (e.g., means, SDs, ranges, percentages) and inferential statistics (e.g., one-way analysis of variance, Tukey's HSD Test). The level of significance for the inferential statistics was 0.05.
Results
Descriptive data analysis was used to calculate the MMV for each of the three groups: Group 1, double electric breast pump; Group 2, single non-electric manual breast pump; and Group 3, hand breastmilk expression. The mean MMVs in milliliters per day averaged over the 7-day study period were as follows: Group 1, mean = 647 mL (SD = 310); Group 2, mean = 520 mL (SD = 298); and Group 3, mean = 434 mL (SD = 291) (Table 2). Figure 1 shows a graph of the daily mean MMV for each group. Results from the one-way analysis of variance revealed significant differences in the mean MMV based on method of maternal milk expression (F = 6.52, p = 0.0019) (Table 3). Further analysis using Tukey's HSD Test revealed significant differences in the mean MMV between Groups 1 and 3 (p < 0.01) but not between Groups 1 and 2 or between Groups 2 and 3.
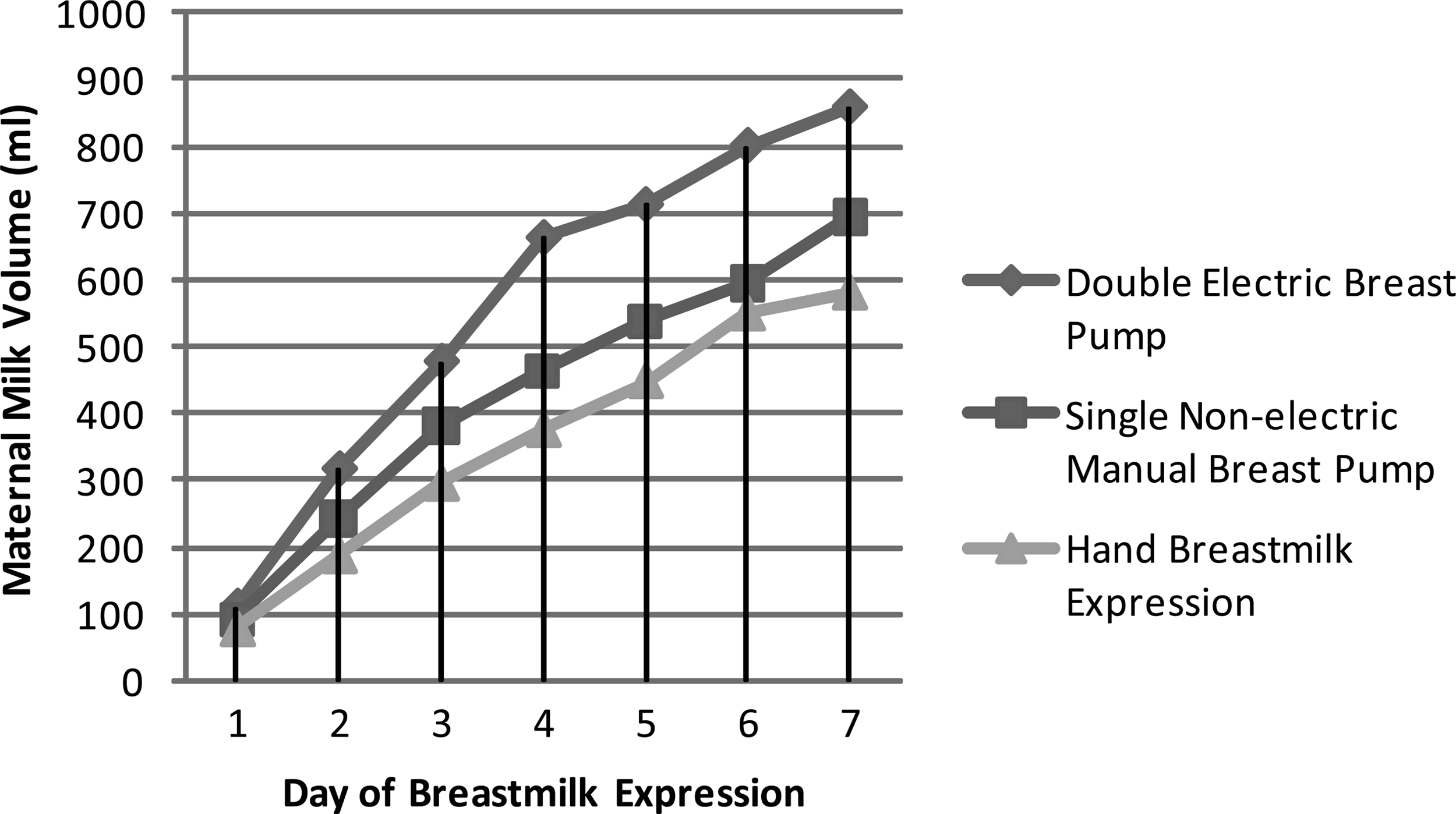
Maternal milk volume by day of breastmilk expression in the three maternal milk expression groups.
Averaged over the 7-day study period.
By day 7, 73% (n = 40) of the mothers in Group 1, 75% (n = 44) of the mothers in Group 2, and 68% (n = 32) of the mothers in Group 3 were producing a mean MMV of 576 mL/day. There was no significant difference between the number of mothers in each group producing at least 576 mL/day by day 7: 73%, 75%, and 68% in Groups 1, 2, and 3, respectively (p = 0.75).
Discussion
The use of the double electric breast pump produced a greater mean MMV and earlier production of adequate MMV for support of infant growth and development than the use of hand breastmilk expression, as currently practiced in Uganda and many developing countries. This finding of increased MMV is supported by several other studies.10,19 However, some studies suggest that there is a role for hand breastmilk expression, especially in the initial 48 hours 12 and beyond. 20 Although in this study MMV in mothers using the double electric breast pump was higher, it is important that the single non-electric pump and hand expression yielded adequate volumes for many mothers.
In the first few days after the birth of a premature or sick infant, a mother may only be able to express a teaspoonful of colostrum with each milk expression session. Over the next few days, the MMV obtained through breastmilk expression generally increases significantly. The estimated mean MMV according to Ingram et al. 21 is 576 mL by day of life 7 for term infants feeding at the breast, with a range of 200–1,013 mL. However, larger volumes are preferred for mothers of preterm infants on day 7 of life in order to ensure a sustained milk production supporting the nutritional demands of the growing premature or ill infant.21–25 For the three groups in this study, the double electric breast pump group exceeded 576 mL by 71 mL, whereas the single non-electric manual breast pump group averaged 56 mL less than 576 mL, and the mothers hand expressing yielded 142 mL less than the recommended 576 mL. Nevertheless, the majority of the mothers in the hand breastmilk expression group produced greater than 576 mL/day by day 7. This finding supports the idea that hand breastmilk expression should continue to be taught, encouraged, and supported in developing world nurseries, but also supports the need to have a double electric breast pump available for those mothers who have inadequate MMV with the use of hand breastmilk expression alone. As recently suggested by Morton et al., 26 the best option for many mothers may be a combination of methods of maternal milk expression. In their study, the combination of the double electric breast pump and hand breastmilk expression gave the best yield.
Conclusions
The use of the double electric breast pump produced significantly more breastmilk than hand breastmilk expression. However, a significant difference was not found between the mean MMV obtained with the double electric breast pump and single non-electric manual breast pump, or between the MMV obtained with the single non-electric manual breast pump and hand breastmilk expression. Although the double electric breast pump provided the highest mean MMV, many mothers obtained adequate MMV for their infants with the use of the single non-electric manual breast pump or hand breastmilk expression.
Electric breast pumps are important adjuncts in making exclusive breastmilk feedings possible for sick and premature infants in the developing world. However, future studies in the developing world should be done to further explore hand breastmilk expression and its potential to achieve adequate MMV when used alone and/or in combination with either single non-electric manual breast pumps or double electric breast pumps. As supported by studies done in the developed world, but not yet in resource-poor settings, combined methods of breastmilk expression may provide the greatest benefit to the most vulnerable infants worldwide.
Footnotes
Acknowledgments
The authors are grateful to Medela, Inc., McHenry, IL, for the grant money, breast pumps, and equipment donated in support of this study. Additionally, the authors thank Michelle Smith, Ph.D., Assistant Professor, Director of Statistical Consulting Center & Department of Mathematics & Statistics, Eastern Kentucky University, Richmond, KY, for her help with data analysis. The authors also thank the dedicated staff in the Special Care Nursery at Mulago Hospital, Kampala, Uganda, for their tireless efforts in the care of the sick and premature infants: specifically, Margaret Musoke, Rebecca Beene, Ruth Tazimuza, Jane Malwa, Rehema Nabuwufu, Florence Nakirijja, Harriet Namusobya, Regina Namakula, Grace Ariokot, Margaret Adokorach, Sophia Lubowa, Joyce Nanyonjo, and Christine Ondoru. Finally, the authors would like to thank Dr. Yvonne Vaucher, M.D., M.P.H., for her review of the article.
Disclosure Statement
No competing financial interests exist.