
Abstract
Abstract
Aim:
This study investigated if a maternally reported, immediate improvement in breastfeeding following division of tongue-tie is due to a placebo effect.
Methods:
This randomized controlled trial was conducted at Southampton General Hospital, Southampton, UK, in 2003–2004. Sixty breastfed babies 5–115 days old (mean, 32 days; median, 23 days) were randomized to division (Group A) or non-division (Group B). The mother and a trained observer were blinded and assessed breastfeeding before the intervention. Fifty-seven babies were analyzed because blinding failed in three of the babies in Group A. Following the intervention, the mother's and observer's views were noted, and then those infants allocated to non-division had their tongue-tie divided.
Results:
Seventy-eight percent (21 of 27) of mothers in Group A reported an immediate improvement in feeding following the intervention, compared with 47% (14 of 30) in Group B (two-tailed χ2 p<0.02; 95% confidence interval, 6–51%). At 1-day follow-up, 90% (54 of 60) reported improved feeding following division. At 3-month follow-up, 92% (54 of 59) still reported improved feeding, with 51% (30 of 59) continuing to breastfeed.
Conclusions:
There is a real, immediate improvement in breastfeeding, detectable by the mother, which is sustained and does not appear to be due to a placebo effect.
Introduction
Tongue-tie is a common condition with a reported incidence of 3–4% (range, 0.02–10.7%).5–8 The difficulties in breastfeeding attributed to tongue-tie include difficulty in latching and maintaining latch, an inefficient feeding cycle, maternal pain or the sensation of chomping, and reduced milk supply.5,9–12 Although less affected, bottle-fed babies may also experience problems such as very slow feeding, excess dribbling, or excess wind. 4 Feeding difficulties have been reported in 25–44% of infants with tongue-ties.5,6,12
Several studies have found division of tongue-tie to be simple, safe, and successful. The largest prospective study (n=215) found no serious complications in any of the infants. 12
To the best of our knowledge there is only one published, randomized, controlled trial looking at tongue-tie division and feeding; this found that division of tongue-tie improved feeding in 96% compared with 3.4% of those referred to a lactation consultant. 5 Eighty percent of the mothers reported an immediate improvement in feeding after knowing that the tongue-tie had been divided. The study was not blinded.
In addition, a previous study 12 suggested that 57% of mothers claimed that the feeding improved immediately, but they also knew that the tongue-tie had been divided.
Statisticians know that this lack of blinding is associated with an overly optimistic estimate of the effect of an intervention, in our case, tongue-tie division, especially if the outcome is subjectively assessed. 13
More recently, there has been a randomized, prospective study investigating nipple pain following tongue-tie division, in which mothers and investigators were blinded as to whether division had been performed or not. The authors found a significant decrease in maternal pain in the group that had had division but did not comment on whether there was a change in feeding in either the divided or sham division groups. 14
We designed a randomized controlled trial in order to investigate whether the maternally reported, immediate improvement in feeding was a real or placebo effect by blinding both the mother and an independent observer. We also attempted to add objective measurements of feeding outcomes. This research is relevant because it assessed both immediate and medium-term feeding outcomes in 60 breastfed infants. It aimed to investigate if there is a real, immediate improvement in breastfeeding following division of tongue-tie and if this improvement is sustained. It would also add to the evidence, requested by the National Institute for Health and Clinical Excellence, 2 that division of tongue-tie without an anesthetic in infants is safe, successful, and acceptable to parents.
Subjects and Methods
This ethics committee approved research was conducted at Southampton General Hospital, Southampton, UK, between October 2003 and April 2004 (follow-up completed July 2004). The mothers and babies were recruited from the referrals to one author (M.G.) for division of tongue-tie. Inclusion criteria were age less than 4 months old, symptoms of a breastfeeding problem, and that a tongue-tie was present. Parents were given written study information on arrival and had the usual consultation with either M.G. or C.W. where the tongue-tie and feeding difficulties were confirmed and the nature of the procedure was explained. If the parents still requested division and the inclusion criteria were met, they were then invited to take part in the study by J.B., and written, informed consent was obtained. Consultation and tongue-tie division were conducted by either M.G. or C.W., and to standardize the objective measures the trained observer was always J.B.
Infants were randomized to immediate division (Group A) or non-division (Group B). The University of Southampton Medical Statistics and Computing Department provided the computer-generated randomization for 60 babies, and an independent helper then placed the randomization into sealed envelopes. The envelope was only opened by M.G. or C.W. after the consent form had been signed.
Both the parents and the observer were blind to the group. All infants had a short sample feed (approximately 2 minutes) to allow the observer to assess feeding using a scoring sheet adapted from the LATCH scoring system 15 and the Infant Breastfeeding Assessment Tool 16 in an attempt to add objective assessment to any change in feeding. A maternal pain numeric score (scale of 1–10, with 1 being least and 10 being most pain) was recorded during the sample feed. The feed was interrupted, and the infant was taken away for the intervention. Division was performed by separating the baby from the parents and wrapping the child securely in a towel. An assistant (a member of nursing staff) then held the baby's shoulders firmly with the palms of his or her hands while his or her wrists fixed the head. The person dividing the tongue-tie then put the tongue-tie on the stretch with their left index finger, while holding the lower lip clear with his or her left thumb. The tie was divided completely with sharp, blunt-ended sterile scissors, and the floor of the mouth was compressed with sterile gauze swab. The baby was promptly unwrapped, cuddled, and returned to the mother.5,12 The only difference between the groups was whether the tongue-tie was or was not actually divided. Care was taken to ensure that there were no visual clues (e.g., blood) or unusual delays that might suggest to the mother or the observer which group the baby was in. All infants were returned to their mothers with a gauze square held under their tongue (whether divided or not), and feeding resumed. First, the observer recorded any change in feeding on the score sheet and whether they felt the tongue-tie had been divided or not. The observer then asked the mother whether she felt feeding was “better, worse, or just the same.” The observer then used an open question to ask the mother how feeding had changed (if at all) and recorded the mother's reply on the scoresheet. The mother was then asked to answer whether the tongue-tie had been divided or not. A second maternal pain numeric score was recorded. This usually took around 1–2 minutes. The mother was then informed whether or not the division had been performed. Those infants who had been allocated to non-division were then taken to have the procedure performed in the usual manner and were again returned to their mothers for feeding to resume. The mothers' views on any change in feeding were again noted, although they were no longer blinded.
The outcome measures were as follows: Primary outcome, subjective and objective improvement in feeding; secondary outcome, maternal pain score.
Follow-up was performed by telephone call at 1 day to record any subjective change in feeding (on a scale of worse, no improvement, improved, big improvement, or full resolution of feeding problems) and any complications. A second phone call at 3 months after the tongue-tie division again recorded subjective change in feeding on the same scale as above, breastfeeding rates, and the acceptability of the procedure to the parents.
Sample size was calculated (by the University of Southampton Medical Statistics and Computing Department) that a two-group χ2 test with a 0.05 two-sided significance level will have 80% power to detect the difference between a divided success (feeding improved) proportion of 69% and a not-divided success (feeding improved) proportion of 30% when the sample size in each group is 25.
Statistical analysis was conducted using SPSS for Windows version 11 (SPSS, Inc., Chicago, IL) and Analyse-it® (Analyse-it Software, Ltd., Leeds, UK) for Microsoft (Redmond, WA) Excel. The confidence intervals were calculated using Confidence Interval Analysis (CIA) software. 17
Results
Of 100 infants seen during the study period, 14 were bottle-fed and therefore excluded. Sixty-nine infants were consented to participate. Of these, nine were withdrawn from the study by the researchers (because the infant would not feed). Figure 1 shows a diagram of the consort flow of participants. Blinding was unsuccessful for three mothers in Group A because of visible blood.
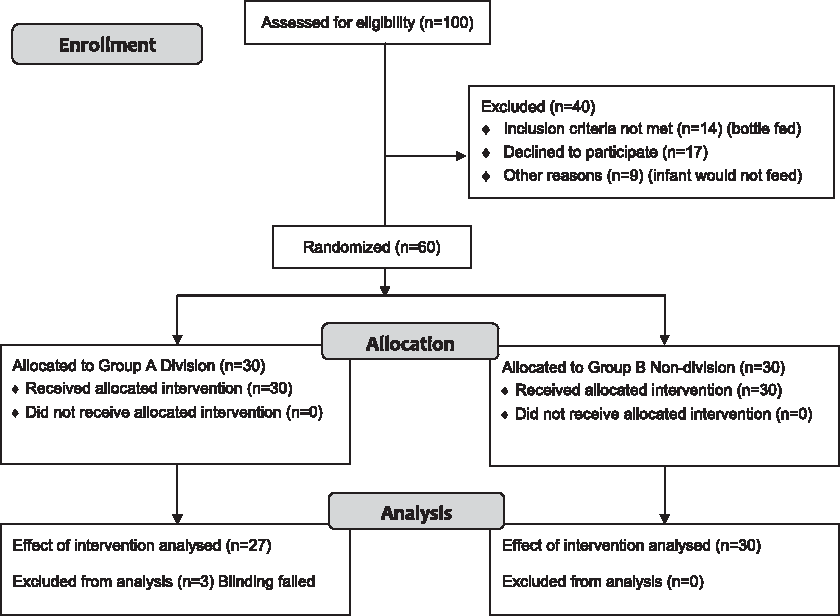
CONSORT 2010 flow diagram for this double-blind, randomized, controlled trial of tongue-tie division and its immediate effect on breastfeeding.
Participants
There were 27 infants in Group A and 30 infants in Group B. The patient characteristics and symptoms were similar for both groups (Table 1).
Group A received immediate tongue-tie division; Group B was originally non-division.
Primary outcome
Immediately following the intervention, the only objective, observed change in feeding was a better latch. The immediate subjective changes verbalized by the mothers and recorded by the observer included a better latch, reduced pain, the baby sucking differently, feeding feeling “more effective,” and a less frantic, more relaxed feed.
Seventy-eight percent (21 of 27) of mothers in Group A stated that the feed had improved following the intervention, compared with 47% (14 of 30) of mothers in Group B. Two-tailed χ2 analysis showed this result to be significant at the p<0.02 level of significance (95% confidence interval, 6–51%).
In Group A 77% of mothers were correct in stating whether tongue-tie had been divided or not, in Group B 55% were correct, and, overall, 65% mothers were correct (95% confidence interval, 52–76%). The mother's accuracy appeared to be related to the number of children she had had (Table 2).
n=49 because the number of children was missing for eight cases and blinding was unsuccessful in three cases.
The objective observer reporting improved feeding in 50% (13 of 26) (blinding failed in n=4 for the observer) of babies in Group A compared with 40% (12 of 30) in Group B, but this difference was not statistically significant.
Secondary outcome: Maternal pain
Twenty-nine of 60 mothers had pain during the sample feed (including one mother in whom blinding failed). Results for the remaining 28 mothers are given (by chance there were 14 in each group). None had increased pain following the intervention. In Group A the average pain score decreased from 4.1 to 1.6, a change of –2.5 (SD±1.9), compared with a reduction from 4.2 to 2.9 in Group B, a change of –1.3 (SD±1.5). Two-tailed Mann–Whitney U test showed the difference in mean pain score change to be not significant at the p=0.13 level of significance (95% confidence interval, –0.3 to 2.4).
Follow-up
Day 1
The mean age of babies whose mothers reported full resolution of the feeding problems was 8 days younger than those whose mothers reported no improvement (26 days vs. 34 days). No mothers reported worsened feeding.
Complications
There were no significant complications. In 5% (n=3) mothers reported a small amount of bleeding at home following the division.
3 months
At 3 months after division 92% (54 of 59) of parents reported improved feeding, with 56% (33 of 59) reporting full resolution. There was no improvement in 8% (five of 59), and one infant was lost to follow-up. Sixty-five percent (38 of 59) of babies were being breastfed at 3 months of age, whereas 51% (30 of 59) were continuing to breastfeed at the second phone call (mean age, 4.5 months).
No mothers reported worsened feeding. All of the mothers contacted would choose to have the tongue-tie divided again if they were in the same situation in the future.
Discussion
The aim of this study was to determine whether a previously reported, immediate improvement in feeding following division of tongue-tie was a real or placebo effect and whether this improvement was sustained. It also aimed to add to the existing evidence that division of tongue-tie without anesthetic is safe and acceptable to parents.
The indications for division in this study were latch difficulties, pain, chomping, and inefficient feeding. These were the same symptoms as found in other research into breastfeeding and tongue-tie.5,9–12 The proportions of mothers presenting with each symptom were also similar to those found in previous research. 12 This suggests that our sample of infants with tongue-tie is comparable with the infants in the other studies.
Mothers in this study were blinded as to whether the tongue-tie had been divided or not when assessing any immediate changes in feeding. Seventy-eight percent (21 of 27) reported an immediate improvement in feeding following division of the tongue-tie compared with 47% (14 of 30) who reported improved feeding when the tongue-tie was not divided. The difference between the two groups of 31% is significant (p<0.02). This supports the previous reports that mothers could identify an immediate improvement in feeding following division of a tongue-tie and that this is a real, not a placebo, effect.5,12
Unlike a recently published, randomized, blinded trial, 14 our study found no significant immediate difference in maternal pain numeric scores. This may be because our babies were about 3 weeks old (compared with 2–3 days in their study), and the mothers' nipples were sore, however well the baby fed. This soreness usually takes about 2 days to heal once the baby is breastfeeding, not nipple-feeding.
The rate of complications recorded in this study (5% [three of 60]) is slightly higher than previous research (3%). 12 None of the complications were significant, and all of the infants with a recorded complication were feeding better at 1 day after division. At 3 months after division all of the parents contacted said that they would choose to have division again. This supports the previous reports that have found that division of tongue-tie is a safe procedure and is acceptable to parents.3,5,9,12,18
Further confirmation that the improvement in breastfeeding is not a placebo effect can be seen in the medium-term breastfeeding rates. If the maternally reported, immediate improvement was simply a placebo effect, then the breastfeeding rates in the study population of babies should be similar to national rates. However, at the 3-month follow-up, 51% (30 of 59) of babies were still being breastfed (mean age, 4.5 months) compared with the national average of only 29% at 4 months. 2 Although we acknowledge that we had a motivated group of mothers, in the absence of any other objective measurements, we feel that the breastfeeding rates are the best objective measure of the success of division.
A consistent limitation with previous studies was a lack of objective immediate measures of breastfeeding. To try to overcome this, an objective score sheet (like a postoperative pain score) was developed for use by the trained observer from the LATCH charting system 15 and the Infant Breastfeeding Assessment Tool. 16 These tools are designed for newborn babies as a guide for midwives. Our score sheet had been planned as a tool to give scores for before and after the intervention, allowing breastfeeding to be objectively quantified. However, the improvements in feeding reported by the observer were not significantly different between the two groups. This was because the categories used in the tool were too broad to give any difference in the “before” and “after” scores. The most important area in objectively assessing any immediate change in feeding was the quality of the latch. In many cases, although the latch improved, the baby stayed in the same category on the score sheet, and thus the score remained the same. This failure of an objective scoring system was also noted in the blinded study of nipple pain. 14 Breastfeeding is a subjective experience, and, as such, mothers are still the best judge of any change in feeding.
The ideal way to conduct this study would have been to assess the “before” and “after” scores and sensation over two normal feeds, several hours apart, that took place as the mother responded to her baby's usual cues for feeding. However, this would be time consuming for both parents and researchers, and it is almost impossible that blinding could be successful over this length of time.
The correct age for division is still a dilemma. Division “too early” risks criticism that the baby may still feed well without division, whereas division “too late” produces a worn-out mother and baby and raises the possibility that the baby may not breastfeed normally long term. Our group's two previous articles5,12 and the present report have independently, over a period of 4 years, described division in babies with a mean age of about 3 weeks who should have been established on successful breastfeeding, but were struggling. This inevitably means that some mothers have given up breastfeeding already. In addition, earlier division has been shown to allow a faster recovery of normal feeding patterns and a more successful outcome. 18 Possibly, breastfeeding advisors should be aiming for division in symptomatic babies by 2 weeks old.
Conclusions
This randomized controlled trial (in which both the mother and observer were blinded) found that the maternally reported, immediate improvement in feeding after division of tongue-tie is a real and not a placebo effect.
It found that the majority of blinded mothers were able to correctly identify when the tongue-tie had been divided through changes in the way that their infant fed, and the more experienced the mother, the more accurate they were in this.
Division of tongue-tie enabled mothers to continue to breastfeed at rates nearly twice the national average. This is the only objective measurement of success that this study found.
As in previous studies, this study found that tongue-ties are a reversible cause of breastfeeding difficulties that should be looked for by breastfeeding advisors and that timely intervention with division of the tongue-tie is simple, safe, and successful.3–5,9,10,12,14,18
What Is Already Known About This Topic?
Feeding in infants with breastfeeding problems may be improved by division of tongue-tie.
The published data suggest that division of tongue-tie without anesthesia in infants is safe and acceptable to parents.
Key Points
1. This study removes bias from the assessment of breastfeeding following the intervention and attempts, but fails, to objectively assess breastfeeding.
2. The maternally reported, immediate, subjective improvement in breastfeeding is a real, not a placebo, effect.
3. It adds further evidence to the medium-term follow-up of breastfeeding outcomes following division of tongue-tie and supports the previous findings that division of tongue-tie is simple, safe, and successful.
Footnotes
Disclosure Statement
No competing financial interests exist.