
Abstract
Abstract
Objectives:
This study was conducted to determine prevalence of exclusive breastfeeding during the first 6 months of life and to identify factors that interfere with this practice in the study area.
Methods:
A retrograde cross-sectional study included 1,059 mothers who attended the rural health unit to immunize their young children (6–24 months old) in Al Der village in Kaliubia Governorate, Egypt.
Results:
We found 95.8% of mothers (1,015 of 1,059) breastfeeding their babies, whereas only 9.7% (103 of 1,059) were exclusively breastfeeding their infants for 6 months. Among the different sociodemographic, maternal, and infant factors studied, only antenatal care (four or more visits), early breastfeeding initiation after delivery, male infant, and absence of breastfeeding difficulties were the significant predictors associated with higher chance for exclusive breastfeeding.
Conclusions:
This study indicates that the prevalence rate of exclusive breastfeeding is low in Egypt and that interventions are needed to bridge the gap between the current practices of breastfeeding and the World Health Organization recommendations.
Introduction
Exclusive breastfeeding reduces infant mortality related to common childhood illnesses such as diarrhea or pneumonia and helps achieving a quicker recovery during illness. 5 Several studies intended to define determinant variables in the success or failure of breastfeeding, which could ease the planning of promotional strategies.6,7 Most infants today still do not receive the full benefits of breastfeeding, leaving millions at unnecessary risk of illness and death, and most health workers lack the skills and knowledge needed to help mothers improve their feeding practices. 1 Planning, implementation, and evaluation of programs to promote appropriate infant feeding practices require detailed current information about these practices in the target population.
Subjects and Methods
Study objectives
A cross-sectional descriptive design was adopted to estimate the prevalence of exclusive breastfeeding in the first 6 months of life, to identify factors associated with this practice, and to study the effect of this practice on the nutritional status of these infants.
Population and sampling
A convenience sample was taken from the mothers of infants 6–24 months old who attended the rural health unit for vaccination of their children. The setting was the vaccination room in the rural health unit of Al Der village in Kalubia Governorate, Egypt. The study was conducted over a period of 6 months from January to June 2010. The calculated sample size was 1,048 mothers using the Epicalc2000 program (Brixton Health [www.brixtonhealth.com/]) (using the prevalence of exclusive breastfeeding in Egypt [12.3%], 8 significance level at 0.05, and study power of 80%). Our data were collected from 1,059 mothers.
Data collection
Data collection was carried out using a field-pretested interviewing questionnaire covering the following elements: Sociodemographic status of the mothers and their families and socioeconomic score, which contained social variables including fathers' education (range 2–10), mothers' education and work (range 1–10), and crowding index (range 1–5). The total score was calculated as follows: A score from 19 to 25 means high social class, a score from 12 to 18 means middle social class, and a score below 12 means low social class. 9 Also, the questionnaire included the type of foods given in the first 6 months (water, herbal drinks, yogurt, artificial milk, animal milk, and others), the exact duration of exclusive breastfeeding, the number of antenatal visits, assessment of proper position of the baby while breastfeeding (i.e., facing the mother, the whole body is supported, the neck is straight or slightly extended), assessment of proper latch on (i.e., chin is touching the breast, mouth is widely open, the lower lip is turned outward), 10 assessment of breastfeeding regulation (i.e., at fixed time intervals), and assessment of infants' weight for age. Analysis of anthropometric data was done by creating weight/age Z scores using the Epi Info™ 6 EPINUT module (Centers for Disease Control and Prevention, Atlanta). 11
Data analysis
Data obtained from the study were coded and entered using Statistical Package for Social Science version 15.0 software (SPSS, Inc., Chicago, IL). Data were summarized using mean, SD, and range for quantitative variables and percentage for qualitative variables. Comparison between groups was done using χ2 and Fisher's exact test for qualitative variables. Logistic regression analysis was done to test for significant predictors for exclusive breastfeeding. A value of p < 0.05 was considered statistically significant.
Ethical consideration
All the included subjects were treated according to the Helsinki Declaration of biomedical ethics. 12 Verbal consent was obtained after proper orientation of the subjects regarding the objectives of the study. Our study was provided ethical approval by the Institutional Review Board of the Department of Pediatrics at Fayoum University.
Results
The study included 1,059 mothers with infants ranging in age from 6 to 24 months. Table 1 shows different sociodemographic and obstetric characteristics of the study group: The mean age of the mothers was 24.7 ± 4.2 years, ranging from 17 to 42 years, and the current age of the children studied was 10.4 ± 4.3 months, ranging from 6 to 24 months. Birth weight of the infants studied was available for 907 infants, with a mean of 3.0561 ± 0.4368 kg, ranging from 1.9 kg to 5 kg.
High level of education means university level or higher.
Last interdelivery interval was only available for multiparous females.
Birth weight was only available for 987 infants, while the number of infants studied was 1,059.
Table 2 shows some feeding characteristics of the group studied: 95.8% of the mothers (1,015 of 1,059) breastfed their infants, and only 9.7% (103 of 1059) exclusively breastfed their infants, whereas 44 mother either did not start (nine mothers) or stopped their breastfeeding early, within a week after birth. Table 2 also shows the starting times of different foods in the first 6 months: Of the 1,059 mothers studied, 248 (23.4%), 794 (75%), 157 (14%), 219 (20.7%), and 435 (41%) started to give water, herbal drinks, artificial milk, animal milk, and yogurt, respectively, in the first 6 months.
Nine mothers were missed, as they did not start breastfeeding.
Some mothers had more than one problem.
The total number was 1,015 (i.e., exactly 44 mothers did not breastfeed.)
No means that the infants were not receiving the food in question.
Table 3 shows the relation between different sociodemographic characteristics and exclusive breastfeeding; only the infant's sex being male showed significant positive association with exclusive breastfeeding. Boys were found to be 1.8 times more exclusively breastfed than girls. On the other hand, no associations were found between exclusive breastfeeding and maternal age, education of the mother and father, maternal working status, place and mode of delivery, parity, social class, last interdelivery interval, and birth weight.
Table 4 shows a highly significant association between exclusive breastfeeding and antenatal care where mothers having four or more antenatal care visits were 1.9 times exclusively breastfeeding their infants more than the others. Table 4 also shows a highly significant association between exclusive breastfeeding and early initiation of breastfeeding after delivery, absence of breastfeeding difficulties, and no use of teats and pacifiers.
Last interdelivery interval was only available for multiparous women (447) out of 1,015 mothers that breastfed their infants (the total of exclusively breastfed was 48).
Birth weight was only available for 872 infants out of 1,015 breastfed infants (the total of exclusively breastfed was 83).
Table 5 shows the significant predictors for exclusive breastfeeding by logistic regression analysis: Maternal age 20–30 years, antenatal care (four or more visits), early breastfeeding initiation after delivery, male infant, and absence of breastfeeding difficulties were the significant predictors associated with higher chance for exclusive breastfeeding with odds ratios of 2.9, 2.8, 2.2, 2.1, and 1.8, respectively. On the other hand, social class, parent education, and mother's work were not found to be significant predictors for exclusive breastfeeding.
Figure 1 shows the relation between exclusive breastfeeding and nutritional status of infants in the first 6 months of life. Infants who were not exclusively breastfed had nearly four times the risk of being underweight than exclusively breastfed infants (17.2% and 4.7%, respectively).
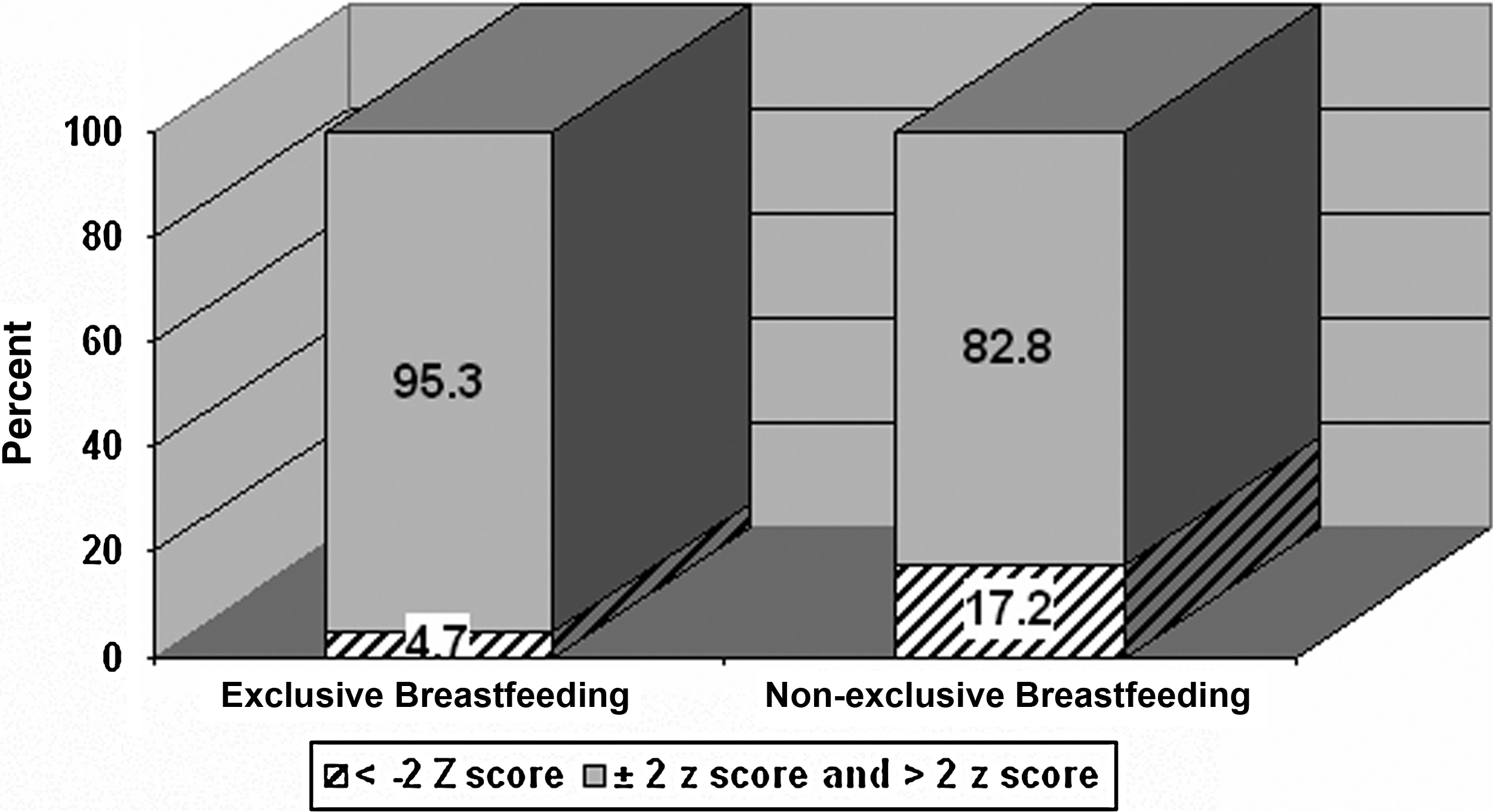
Association between exclusive breastfeeding and nutritional status of children in the first 6 months of life in Al Der village in Kaliubia Governorate, Egypt. Statistics: χ2 = 6.67, p = 0.01; odds ratio with 95% confidence interval = 4.2 (1.2, 17.3).
Discussion
Egypt is one of the developing countries in which we need to support correct feeding practices. Exclusive breastfeeding is a safe, economical, and emotionally satisfying means of feeding babies. The present study aimed to evaluate the rate of exclusive breastfeeding and to determine factors associated with cessation of exclusive breastfeeding within the first 6 months of life. Although ever breastfeeding was 95.8%, only 9.7% of the mothers remained exclusively breastfeeding for 6 months, compared with 91.3% and 12.3%, respectively, in the Egyptian Demographic Health Survey (EDHS) in 2008. This could be due to the fact that the EDHS is representative of both rural and urban areas, which is not true for the current study, which represents only rural areas. 8
WHO defined the goal as 6 months of exclusive breastfeeding, that is, the infant only receives breastmilk without any additional food or drink, not even water. 4 As regards the Egyptian 6 months exclusive breastfeeding rate compared with other countries, in Canada the prevalence of exclusive breastfeeding at 6 months was 13.8%, 13 whereas it was 11.3% in the United States, 14 10.1% in Sweden, 15 and 7% in Norway. 16 Also, exclusive breastfeeding rates by U.N. regions are 25% in Africa, 45% in Asia, and 31% in Latin America. 17 However, Chudasama et al. 18 reported a prevalence rate of 62% due to better health services available under the Integrated Management of Neonatal and Childhood Illness in India. This could give us an idea about exclusive breastfeeding rates all over the world and the needs for national organized support for that issue.
Regarding the pattern of breastfeeding, 80.3% of the mothers reported breastfeeding on demand, which is recommended by the WHO for the child to have adequate nutrition. 3 This is similar to the value reported from a developed country like Sweden, where most of the mothers reported that they breastfed on demand. 19 In contrast, proper position during breastfeeding was 18.4%, and proper latch on was 7.6%, because of the lack of health workers having the skills and knowledge needed to help mothers.
We found that 73.3% of mothers initiated breastfeeding soon within the first day of birth, but only 10.4% initiated breastfeeding within 1 hour of birth, which is lower than the findings of the 2008 EDHS, which showed 88% of the mothers breastfed within the first day after delivery and 56% within the first hour; 8 this is because they were given some type of liquid until the mother's breastmilk flowed freely. 8 Haroun et al. 20 found that the majority of mothers initiated breastfeeding after 1 hour from delivery, whereas 54.2% and 39.7% of them initiated breastfeeding during the period from 2 hours to 24 hours, respectively; only 6.0% of the mothers initiated breastfeeding after 1 day.
Although breastfeeding is initiated early for the majority of children, use of prelacteal glucose and herbs is common practice (58.4% and 53.3%, respectively). This is consistent with EDHS results, where 47% received prelacteal feeds during the first 3 days after birth. 8
The present study showed no association between parental education, mother's employment, maternal age, parity, and social class with exclusive breastfeeding. The latter result is different from the study of Agampodi et al., 21 which associates influence of parental education and women's employment on breastfeeding practices. Sheehan et al. 22 found that vaginal deliveries increased the odds of exclusive breastfeeding at 6 months. Pain and discomfort associated with cesarean section may prevent the mother from breastfeeding. Mothers giving birth at home were five times more likely to exclusively breastfeed than others giving birth at hospitals. This relationship can be attributed to the negative influence of formula supplementation and the availability of prelacteal glucose and herbs.
After multivariate analysis by adjusted logistic regression, significant association was found with maternal age, antenatal care (four or more visits), early breastfeeding initiation after birth, male infant, absence of breastfeeding difficulties, and no use of teats and pacifiers. This agrees with Righard and Alade, 23 who concluded that to promote successful breastfeeding and to reduce nursing problems, an incorrect sucking technique should be prevented or corrected, and the use of pacifiers should be avoided or restricted. Also, Wojdan-Godek et al. 24 found that the factors associated with cessation of exclusive breastfeeding were use of a pacifier, mothers' acceptance of short duration of total breastfeeding and exclusive breastfeeding, first child in the family, primary education of parents, mother working in farming and unemployed father, maternal smoking, and maternal age over 34 years. This is in opposition to the study of Al-Sahab et al., 13 who found that years of education was the only significant socioeconomic predictor of 6-month exclusive breastfeeding. In another study conducted in Egypt to examine social and medical factors affecting breastfeeding, El-Mougi et al. 25 also found that antenatal care promoted breastfeeding practices, whereas early start of breastfeeding had no effect. Haroun et al. 20 in the Sudan confirmed the important role of antenatal care, and their study recommended encouraging breastfeeding and educating mothers, especially during pregnancy.
Other studies found that low birth weight was negatively associated with initiation and continuation of exclusive breastfeeding. 26 In our study, there was no association between exclusive breastfeeding and birth weight.
Non-exclusively breastfed infants have more than four times as much risk for becoming underweight than exclusively breastfed infants. This is in accordance with Giashuddin et al., 27 who found that exclusively breastfed infants were nutritionally better off.
Our study has the limitation of being representative of only rural areas and hence cannot be generalized for the entire population of Egypt. Also, the cross-sectional nature of the study and the inability to measure the duration of exclusive breastfeeding longitudinally stand out as other limitations. Furthermore, our Governorate has no Baby Friendly Health facility to promote proper breastfeeding practices and to provide the rural health units with well-trained personnel.
Conclusions
In summary, the results of the present study constitute the basis for designing targeted interventions by policy makers and health professionals in order to bridge the gap between the current practices of breastfeeding and the WHO recommendations. Three of the five significant predictors for exclusive breastfeeding were variables that are changeable by interventions. These three variables are antenatal care, early initiation of breastfeeding, and absence of breastfeeding difficulties. This could be done by supporting the Baby Friendly Hospital Initiative, which promotes, protects, and supports breastfeeding through “The Ten Steps to Successful Breastfeeding for Hospitals,” as outlined by UNICEF/WHO, 4 and also by increasing public as well as the medical community's awareness of proper infant feeding practices. In other words, promoting exclusive breastfeeding rates for the first 6 months of life is highly warranted.
Footnotes
Acknowledgments
The authors thank Dr. Wael Lotfy for revision and useful comments on the manuscript.
Disclosure Statement
No competing financial interests exist.