
Abstract
Abstract
Breast stimulation can produce contractions in a contraction stress test and has been considered for the augmentation of labor and prevention of postpartum hemorrhage. We present a case of intravenous access of a mammary vein in an obstetric patient that led to uterine hyperstimulation. Potential dangers of mammary vein intravenous access are discussed.
Introduction
Possible side effects of breast stimulation include uterine tachysystole, prolonged contractions, uterine hyperstimulation, and premature rupture of membranes. 5 These side effects are more common in postdated pregnancies, with reports of hyperstimulation varying from 24% to 46%.2,6 Factors believed to affect uterine response to breast stimulation include parity, gestational age, presence of underlying contractions, and stage of labor. 5
Other common uses of breast stimulation include contraction stress tests and prevention of postpartum hemorrhage. The use of breast stimulation to produce contractions in a contraction stress test has been shown to be safe, effective, and cost effective when compared with oxytocin administration. 2 When proper technique is used, episodes of hyperstimulation are common but not associated with adverse maternal or fetal outcomes.2,6
Breast stimulation during the third stage of labor effectively decreased blood loss compared with control patients, although still less than that with oxytocin. 4 Therefore it can be an effective option to reduce postpartum hemorrhage in cases where oxytocin or trained technicians are not readily available. The following case report demonstrates that mammary vein intravenous access causing breast stimulation can lead to strong uterine contractions and rapid labor.
Case Report
A 30-year-old woman, gravida 5 parity 1212, was admitted from the clinic to the labor and delivery suite at 35.4 weeks of gestation by last menstrual period consistent with a 17-week ultrasound for evaluation of worsening hypertension. Pregnancy was complicated by chronic hypertension on multiple medications, class B diabetes, history of intrauterine fetal demise at 30 weeks, body mass index of 47 kg/m2, group B Streptococcus positivity, and asthma. The patient was ruled out for superimposed pre-eclampsia with a 24-hour urine protein level of 280 mg. On hospital day 5, the patient's blood pressure remained in the severe range despite treatment with three oral antihypertensives. The decision was made to proceed with induction of labor at 36.2 weeks.
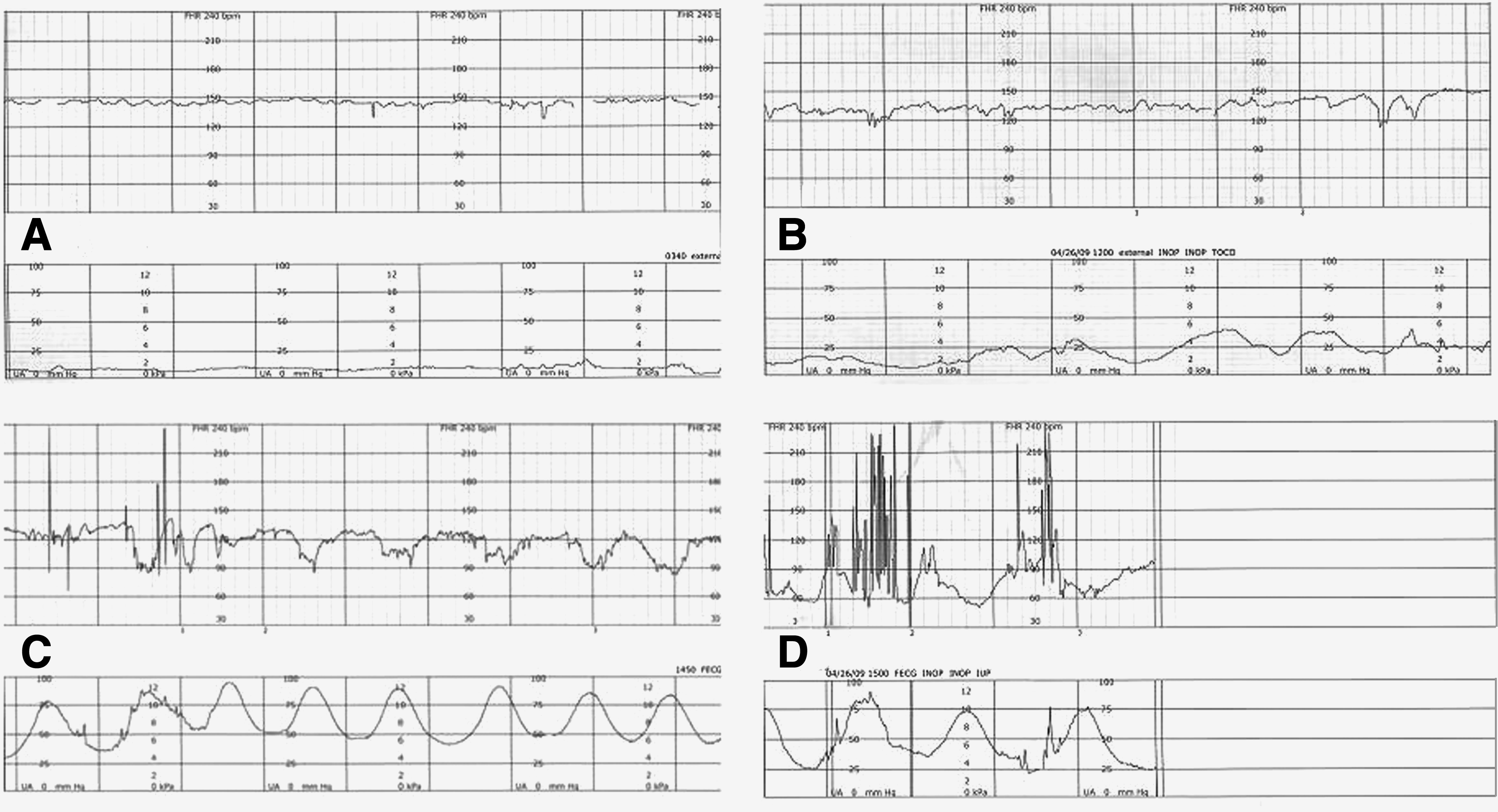
Dinoprostone was used for cervical ripening. Over the following 12 hours, the patient's cervix went from tight fingertip, 25% effaced, and −3 station to 1 cm, 50% effaced, and −3 station. She reported no contractions (Fig. 1A). The dinoprostone insert was removed from her vagina. Although we planned on proceeding with Foley bulb mechanical dilation, the patient was not treated with any further mechanical, prostaglandin, or oxytocin stimulants. Management of her labor, diabetes, hypertension, and eventual need for antibiotics required additional intravenous access. Multiple attempts were made at obtaining peripheral intravenous access, including a peripherally inserted central catheter. However, given the patient's morbid obesity and other co-morbidities, these attempts were not successful. In order to avoid the morbidity associated with a subclavian central line, further opportunities for peripheral access were pursued. Intravenous access was eventually obtained using an 18-gauge needle in a prominent mammary vein, 1 cm medial to the left nipple. Only normal saline was infused through this intravenous site.
(
Over the next 30 minutes, the patient began complaining of strong contractions and had spontaneous rupture of membranes with clear fluid. Fetal scalp electrode and intrauterine pressure catheter were placed, antibiotics were started, and her cervical exam at this point was 2 cm (Fig. 1B). The patient continued having contractions every 1–2 minutes over the following 3 hours and progressed to 7 cm, 100% effaced, 0 station. The fetal heart tracing began having deep variable decelerations, and two subcutaneous doses of 0.25 mg of terbutaline were administered without response (Fig. 1C). An emergent cesarean section was performed for category 3 fetal heart tracing (Fig. 1D). The fetal cord pH at delivery was 7.18, and a nuchal cord was noted at delivery. The placenta was inspected at the time of delivery and by pathology afterward, with no evidence of retroplacental hematoma or other evidence of abruption. The patient's postoperative course was uneventful. Mammary vein intravenous access was terminated in the post-anesthesia care unit.
Comment
Breast stimulation for the augmentation of labor has been reported in the medical literature since the 18th century but in the last 20 years has fallen out of favor.5,7 The small body of literature that has been produced offers no standard definition of terms or technique, but all forms of stimulation tested thus far have produced results better than controls. 2 As more complicated clinical scenarios arise on labor and delivery, especially with obesity, it is important to be cognizant of the struggle for intravenous access and the potential risks of mammary vein access.
To our knowledge, there are no other reports of obtaining peripheral vascular access in a mammary vein in an obstetric patient. In the case presented, we believe that the placement of the intravenous catheter with subsequent infusion in a mammary vein resulted in breast stimulation and led to hyperstimulation that was refractory to tocolysis with terbutaline. Although this specific reaction has not previously been described in the literature, local reactions to infusions have been well documented to cause neural stimulation in the area of placement. 8 Herein, we propose that neural stimulation secondary to placement of an intravenous catheter or subsequent infusion of a mammary vein may result in endogenous oxytocin release via a similar mechanism to nipple stimulation. Based on this observation, it may be prudent for clinicians to avoid the use of mammary intravenous infusions given its potential to stimulate premature labor, spontaneous rupture of membranes, tachysystole, prolonged uterine contractions, or hyperstimulation of the uterus. 5
The resulting uterine hyperstimulation is predictable in retrospect, but during the management of this patient the healthcare team did not make the association between mammary vein intravenous access and oxytocin release. Despite the potential theoretical benefits of mammary vein intravenous access, we caution against this practice, as the oxytocin release would be unpredictable. This case report should serve as a warning for other healthcare providers to be aware of this complication. The intravenous access team at our hospital had used mammary veins for access in the past, but they no longer attempt mammary vein access on pregnant patients.
Intravenous drug users are another subset of patients who may utilize mammary veins for access. There is a paucity of research in this area; however, preterm labor, preterm premature rupture of membranes, or antepartum mastitis in an intravenous drug-using patient may be, in part, explained by mammary vein access.
Although breast stimulation has been shown to be relatively safe compared with oxytocin, breast stimulation has demonstrated a greater incidence of uterine hyperstimulation. 5 Factors known to increase the incidence of uterine hyperstimulation and therefore risk to the mother and fetus include postdated pregnancy, nulliparity, and spontaneous contraction prior to the beginning of breast stimulation. 5
In the present case, the mammary vein stimulation resulted in rapid dilation from 2 cm to 7 cm in 3 hours. The hyperstimulation eventually necessitated an emergent cesarean. Previous reports using traditional nipple stimulation techniques contradict this course. These investigators report a slower progression to active labor compared with that after oxytocin and no increase in adverse fetal or maternal outcomes, including need for cesarean section. 9
Footnotes
Disclosure Statement
No competing financial interests exist.