
Abstract
Abstract
Background:
During medical school and residency training, physicians are taught that breastfeeding is the preferred feeding for all infants, with rare exceptions. But evidence is accumulating that while physician mothers have a high rate of breastfeeding initiation, they face significant obstacles to sustained breastfeeding.
Methods:
In our academic medical center, we conducted a brief survey of physicians who have young children, to explore their own experiences with breastfeeding. The survey explored the physician-as-parent's own experiences with breastfeeding—prenatal intentions, postnatal difficulties, ability to meet goals, emotions if goals were not met, resources for support pre- and postnatally, and ideas about what would have helped her breastfeed longer.
Results:
Two-thirds of the physicians who initiated breastfeeding had difficulties. Among those with difficulties, about three-fourths were able to resolve them.
Conclusions:
Even mothers who are medical professionals experience, and often cannot overcome, difficulties with breastfeeding. Women in medicine need enhanced breastfeeding support and services/resources. Advocacy is needed, in our work environments, for better breastfeeding support not only for our physician colleagues, but also for all lactating employees within our institutions.
Introduction
“
The United States Breastfeeding Committee notes that “among employed women with children under age 3, approximately 70% work full time.” 1 As a percentage of medical school graduates, women have increased from 7% to 49% over the past 45 years. 2 During residency and the first several years of practice, many of these women are themselves mothers of children whom they breastfeed. Medical students are taught that breastfeeding provides numerous advantages to a developing infant and is important for the mother's health. 3 However, as a resident, how can a mother find time to fulfill the breastfeeding recommendations that the rest of us preach? Even beyond the severe time constraints imposed by residency, physician mothers also face the other obstacles to breastfeeding faced by the general population.
Given the central role that pediatricians' enthusiastic support and involvement play for their breastfeeding dyad patients, 3 , it would be enlightening to describe pediatricians' (and other physicians') experiences in breastfeeding their own children amidst the hustle and bustle of life in the medical workforce. Reports since 19964,5 from the United States4–8 and Canada9,10 have documented that although physician mothers have a high rate of breastfeeding initiation, they face significant obstacles to sustained breastfeeding and have 6-month breastfeeding rates well below Healthy People 2020 goals. Key obstacles include the return, after maternity leave, to the rigorous work schedule of residency or primary care practice, as well as inadequate support for milk expression in the workplace.4–7
Describing physicians' experiences is important from two perspectives. First, physicians' own experiences in breastfeeding their children may adversely affect their future interactions with breastfeeding mothers who are patients.11,12 Second, from a systems perspective, breastfeeding physician mothers work in settings that are encouraged by national and international guidelines to be supportive of breastfeeding.3,13–15 Geraghty et al. 16 outlined strategies—in outpatient, inpatient, maternity, and emergency department settings—that we as clinician and administrative leaders in pediatrics can implement to improve breastfeeding support for the mothers of our patients. But how supportive are these same settings for our own colleagues who breastfeed their children? We conducted a brief survey, focused on pediatric residents, in 2007, not long after the release of the American Academy of Pediatrics policy statement, “Breastfeeding and the Use of Human Milk.” 3
Subjects and Methods
In 2007, in an academic medical center in Indianapolis, IN, we conducted a 20-item internet-based survey of 42 resident and staff physicians who are parents. The survey was offered to residents in pediatrics and family medicine and to faculty members in pediatrics. After six basic descriptive items (gender, age, ethnicity, level of training, number of children, and age of youngest child), the respondents were asked in the survey (Table 1) about prenatal intentions, postnatal difficulties, ability to meet goals, emotions if goals were not met, resources for support pre- and postnatally, and ideas about what would have helped them breastfeed longer. Based on both the literature cited above and anecdotal experiences recounted by colleagues, we anticipated that the physicians surveyed may have breastfeeding rates lower than some of the Healthy People goals. The purpose of this study was primarily descriptive, to suggest hypotheses as to factors that limit breastfeeding support for physicians—individuals who, in their professional roles, are encouraged to actively support breastfeeding dyads. The survey included multiple choice and open-ended questions. The duration of breastfeeding item had multiple-choice answers (<1 month, 1–3 months, 4–6 months, 6–12 months, >1 year, and currently breastfeeding). This study was approved by the Office of Research Administration of Indiana University Purdue University Indianapolis (as an Exempt application).
Results
Among 42 respondents, 88% were women, 91% were white, and 95% were 21–40 years old. Forty-one percent had one child, 36% two, 14% three, and 9% four. Ninety-eight percent had initiated breastfeeding (Fig. 1), a rate higher than both the Indiana average (71%, based on the Centers for Disease Control National Immunization Survey data 17 ) and the Healthy People 2020 goal 18 (82%). At 6 months, 68% were breastfeeding (a rate higher than the Indiana average of 38% and the Healthy People 2020 goal of 61%), and at 1 year, 12% (below the Indiana average of 17% and the Healthy People 2020 goal of 32%).

Seventy-six percent of the physicians who initiated breastfeeding had difficulties. Among those with difficulties, 73% were able to resolve them, but 27% were unsuccessful. Eighty-eight percent of those who did not resolve the difficulties did not meet their breastfeeding goal. Overall, 24% (10 of 41) did not reach their breastfeeding duration goal. Eight of these 10 experienced negative emotions, which they described in a free-text item as “inadequate,” “sad,” “disappointed,” “frustrated,” “bad,” “like I had failed,” “a bit depressed,” or “disappointed, failed badly.”
Some (13 of 38 [34%] who answered the question “What influenced your decision to stop breastfeeding?”) stopped because they had to return to work, because of difficulties associated with pumping or breastfeeding while at work, or because the child had reached a certain age (14 of 38 [38%]). The work-related reasons included that pumping was too stressful, that things were too busy at work to have time to pump, or “the inability to keep up with demand” for expressed milk once back at work. Starting a “demanding rotation” was cited by one respondent. Inadequate pumping among a few respondents led to decreased milk production and premature weaning by the infants. Some physicians mentioned that formula feeding was easier for childcare facilities.
When questioned in an open-ended item about what would have allowed them to lengthen the duration of breastfeeding, 17 (61%) of 28 respondents who answered this item (and 41% of the 41 total subjects who were breastfeeding) described improvements that could be made in the workplace. Thirteen of these 17 specifically mentioned the need for a pumping location or improved facilities, and four others mentioned more flexible work hours and/or on-site child care. One resident answered as follows:
I'm still breastfeeding, but it would be a lot easier with more/better pumping facilities (especially rooms with phones in case you get paged) and better understanding from colleagues about the need for regular and frequent pumping sessions.
Before delivery, 76% of respondents obtained information about breastfeeding from books, 62% from family members or friends, 43% from other sources such as prenatal classes and lactation consultants, 32% from obstetricians, and 27% from pediatricians. After delivery, the respondents also sought advice from lactation consultants, books, and family and friends more than from other physicians (Fig. 2).
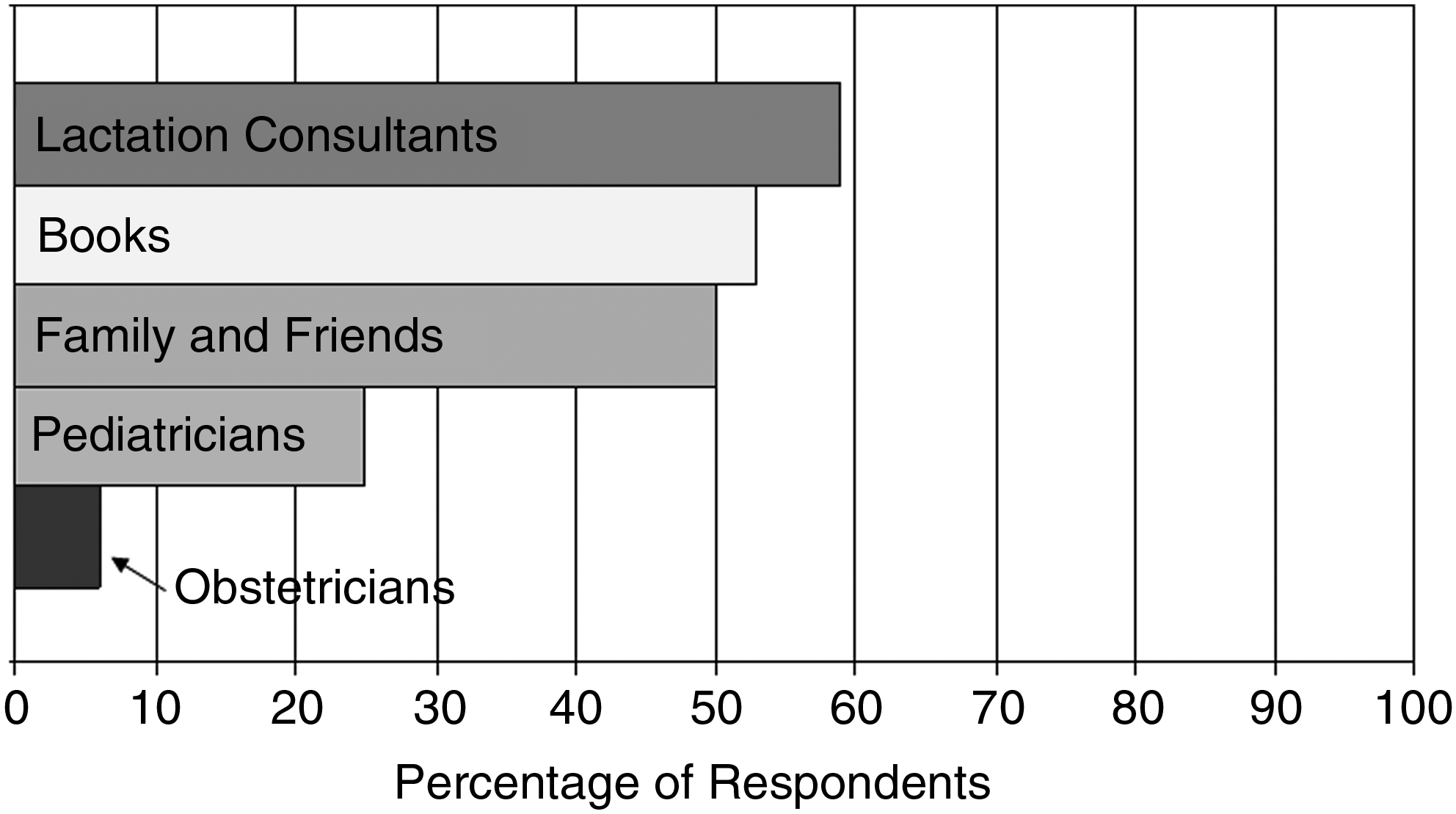
Physician mothers with breastfeeding difficulties sought advice from these sources.
Discussion
This brief survey highlights that even mothers who are physicians experience, and often cannot overcome, difficulties with breastfeeding. Almost all of the physicians surveyed initiated breastfeeding, and their breastfeeding rate at 6 months (68%) exceeded the Healthy People 2020 goal (61%). However, the breastfeeding rate at 12 months (12%) was substantially below both the Healthy People 2020 goal (32%) and the rate recently reported for 50 physician mothers at The Johns Hopkins University (41%). 19 Even mothers who are physicians receive inadequate support in the workplace. As a first step, we must advocate for better breastfeeding support not only for our physician colleagues, but also for all lactating employees within our institutions.
A negative personal experience also may adversely affect how a physician advises her own patients down the road.11,12 This phenomenon has also been observed in focus groups involving pediatric and obstetric nurses and allied health professionals, public health nurses, 24-hour telephone triage personnel, employees of the Supplemental Nutrition Program for Women, Infants and Children, and lactation consultants. 20
Women in the medical profession need enhanced breastfeeding support, services, and resources. An ideal pumping environment would include a designated room with a sink, comfortable chair with arms, and breastfeeding supplies. Access to a hospital-grade electric pump and educational and reference materials would also help to promote continued breastfeeding once back to work. 5 Additional workplace requirements are defined by federal guidelines and state laws. In Indiana, the General Assembly passed, and the Governor signed, a Breastfeeding in the Workplace law, effective July 1, 2008: Employers with 25 or more employees must allow women adequate time and a private location (not a bathroom) for breastfeeding. 21 Twenty-four U.S. states have similar laws, 22 and a workplace breastfeeding support provision is part of the new federal healthcare reform bill.
There may be other factors, in addition to those in the workplace, that help explain the breastfeeding patterns observed in this study. Cessation of breastfeeding earlier than recommended by national guidelines may reflect complex interactions between workplace factors and earlier prenatal and postpartum breastfeeding support that the physician parents had, both at home and as patients at healthcare encounters. This possibility, along with the fact that successful breastfeeding promotion and support require effective and collaborative work by healthcare professionals across the spectrum from obstetrics to pediatrics, 20 reminds us that a supportive environment for healthcare professionals who wish to breastfeed should be in place before their infants are delivered—long before the return to work after maternity leave. In this context, the fact that respondents sought advice from lactation consultants, books, and family and friends more than from other physicians (Fig. 2) is worthy of additional study. It may be that the physicians as patients did not think to ask a physician about breastfeeding or did not think that a physician would be able to advise them. Some may not have known a physician to ask or may not have felt comfortable asking.
Conclusions
Workplace support recommendations are listed in the Health Resources and Services Administration publication “The Business Case for Breastfeeding” 23 and the United States Breastfeeding Committee's publication “Accommodations for Breastfeeding in the Workplace.” 24 Unfortunately, if healthcare settings in which physician mothers work do not provide supportive environments for breastfeeding, there are direct adverse effects for the physician mothers and their infants, as well as for the breastfeeding dyad patients in that system. In addition, there may be indirect adverse effects for future breastfeeding dyads, if negative personal experiences among breastfeeding physician mothers affect their subsequent counseling of patients. Physicians are key contributors to supporting guideline-recommended breastfeeding duration among patients, particularly among the underserved. As a study of breastfeeding support among adolescent mothers summarized, “breastfeeding initiation is the result of effective breastfeeding promotion, whereas breastfeeding continuation is the result of continued support.” 25 For these reasons breastfeeding support of physicians, by physicians, for physicians, is worth preserving and strengthening.
Footnotes
Disclosure Statement
No competing financial interests exist.