
Abstract

Introduction
Prevention Before Day 1
Before proceeding into the breastfeeding content of the article, it is necessary to briefly note that "day 1” is too late. A life-course perspective is required, wherein the goal is to "position for prevention" well before day 1. Not only is prevention during the prenatal period, such as a healthy weight gain throughout pregnancy, extremely important to the health of the future baby, but actions during the preconception period are important as well—for example, folic acid supplementation to prevent neural tube defects. Indeed, events in the mother's life experience that occur well before her child-bearing years may have significant impact on the health outcomes of her future children, such as receiving adequate nutrition during the mother's own childhood development. Assuming that pregnant women are well nourished and non–substance abusing and have adequate folic acid levels, we are free to focus on the earliest post-birth prevention, where breastfeeding has an essential and definitive role. When we focus on prevention, we are most concerned about outcomes, but we are also concerned about costs.
Epidemiology of Breastfeeding as Prevention
This article provides a very brief summary of the vast body of epidemiologic evidence that demonstrates the health benefits of breastfeeding. Throughout the examples presented, one pattern continually emerges: Although some breastfeeding is better than none, the best results are achieved when breastfeeding is done exclusively and for longer duration.
One of the most comprehensive systematic reviews of available evidence associating breastfeeding with disease prevention was done for the Agency for Healthcare Research and Quality (AHRQ) in 2007. 1 The review assessed the relationship between breastfeeding and health outcomes in developed countries. Several acute and chronic conditions showed significant risk reductions, ranging from about a 20% decreased risk for child leukemia to a nearly 65% risk reduction for gastrointestinal infections (Fig. 1 1 ). A few of these conditions will be discussed in more detail.

Risk reduction for various conditions in breastfed infants versus infants never breastfed. GI, gastrointestinal; SIDS, sudden infant death syndrome. Data are taken from Ip et al. 1
Breastfeeding decreases the risk of various infections, including acute otitis media. It is assumed that the mechanism for this protection relates to immunoglobulins against common bacteria as well as other factors in the breastmilk that interfere with bacterial attachment to the nasopharynx. Of significance is the difference in degree of risk reduction between ever breastfeeding, which reduces the risk of otitis media by 23%, compared with exclusive breastfeeding for at least 3 months, which demonstrates a 50% risk reduction, a protective effect more than twice as large. 1
Two-thirds of American adults are overweight or obese. Having been breastfed reduces the risk of being obese later in life. As such, breastfeeding is becoming widely accepted as a component of a broader multipronged strategy to battle the obesity epidemic. Various theories have been proposed regarding the mechanism that explains how breastfeeding reduces the risk of obesity. There are hormones in breastmilk involved in satiety and appetite control: Leptin, ghrelin, and adiponectin. 2 Also, babies who are breastfed maintain more control over how many calories they consume compared with those who are formula fed. Early control may translate into better control later in childhood. Research findings confirm that mothers who breastfeed their children exhibit less controlling food behaviors when their children are 1 year of age. Finally, babies who are breastfed are at lower risk for overfeeding and early growth acceleration, which is associated with obesity. 3
As with otitis media, the data show that ever breastfeeding is good, but longer duration of exclusive breastfeeding is associated with improved protection against obesity. Although the size of the protective effect does show variation from study to study and when attempts are made to control for other confounding variables, the effect size does not seem to depend on the age of the study subjects. Whether a study was investigating young children, older children, adolescents, or adults, the protective effect of breastfeeding seemed fairly consistent. In the meta-analysis performed by AHRQ, 1 ever breastfeeding showed a risk reduction for obesity of 24% compared with never breastfeeding. The increased effect of longer duration of exclusive breastfeeding was also quite consistent. From 2 months of exclusive breastfeeding up through 9 months, each additional month decreased the risk of later obesity by an additional 4%, up to a total risk reduction of 30%.
The relationship between breastfeeding and postpartum weight gain for the mother is unclear, and in terms of return to prepregnancy weight within 1–2 years postpartum, the effect of breastfeeding seems fairly negligible. Other factors have a much larger effect on postpartum weight loss than breastfeeding, including annual household income, baseline body mass index, ethnicity, gestational weight gain, and energy intake.
The incidence of sudden infant death syndrome (SIDS) has decreased significantly in many developed countries with the implementation of a "back to sleep" campaign in the 1990s that educated parents and caregivers about the importance of placing infants in a supine position to sleep. Nevertheless, one of the worst tragedies we can conceive of is having a young child die, and SIDS continues to claim too many lives; breastfeeding can further reduce that risk. The actual cause of SIDS or how breastfeeding protects against it has yet to be deciphered. One plausible theory relates to the fact that breastfed babies are more easily arousable from sleep. Another theory involves the immunologic protection from infection noted earlier; many SIDS cases suffered from a minor infection shortly before their death.
The earlier AHRQ study 1 showed an impressive protective effect for breastfeeding against SIDS (Fig. 1 1 ). However, a newly published meta-analysis uses more recent data and indicates a larger effect size than previously established. 4 These results continue to show a familiar pattern. Ever breastfeeding provides impressive protection against SIDS (risk reduction, 60%), whereas increased duration of any breastfeeding provides better protection (63% risk reduction after breastfeeding duration of at least 2 months), and exclusive breastfeeding of any duration is better still than either of the previous two categories (73% risk reduction).
Breastfeeding not only protects the baby from various diseases and conditions but also significantly reduces maternal risk for several serious health conditions as well. A few of these are listed in Figure 2, 1 including certain cancers and type 2 diabetes.
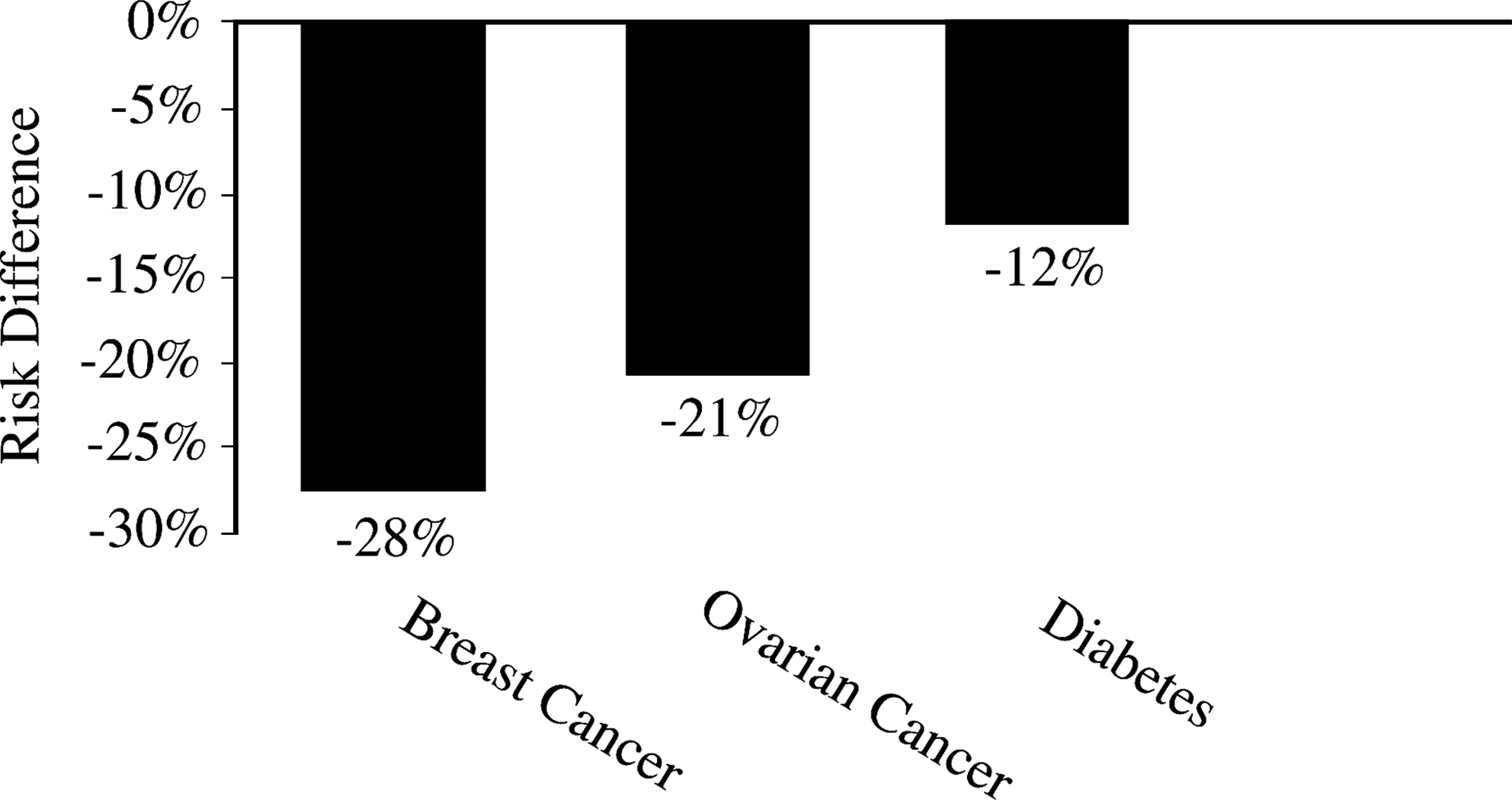
Risk reduction for various conditions in women who breastfed their infants versus women who did not breastfeed. Data are from Ip et al. 1
Because the health benefits of breastfeeding have been well established for several years, it is naturally included in the health objectives for the nation, Healthy People 2020 (Table 1 5 ). Objectives for initiation, exclusivity, and duration of breastfeeding have been carried over from Healthy People 2010 with baselines and targets adjusted. In addition, three newly added objectives reflect recognition of effective strategies for increasing each of these measures. 5 Worksite lactation support allows mothers to return to work while continuing to nurse their infants, increasing breastfeeding duration. Reducing use of formula to supplement diets for breastfed infants promotes more exclusivity of breastfeeding. Lastly, increasing the number of birthing facilities that provide recommended care for lactating mothers improves breastfeeding initiation, as well as promotes exclusivity and duration. In the case of this last objective, "recommended care" refers to a facility that provides all the recommended elements contained in the Ten Steps to Successful Breastfeeding for Hospitals, promoted by the Baby-Friendly Hospital Initiative. 6
Data are from the 2020 Healthypeople.gov website. 5
Evidence-Based Strategies to Improve Breastfeeding Rates
The basic epidemiology clearly demonstrates that exclusive and sustained breastfeeding is a health behavior that reduces risk of numerous diseases and conditions in both mother and child. The next question is: What is needed to successfully promote that practice and increase breastfeeding rates and duration? This requires that one look at a different type of evidence: The effectiveness of various interventions.
The U.S. Preventive Services Task Force evaluates evidence for effectiveness of preventive services delivered in the clinical setting, generally a primary care setting. Primary care interventions to promote breastfeeding received a grade of B, which means the service is recommended. 7 Several effective interventions are suggested, including formal breastfeeding education for mothers and families, direct support of mothers during breastfeeding, training of primary care staff about breastfeeding and techniques for breastfeeding support, and peer support. Although the review did not separate out the relative effectiveness of each strategy, the Task Force did recommend that multiple strategies are preferable to one and that targeting both the prenatal and postpartum periods would be most effective at improving breastfeeding duration.
One of the most comprehensive guides to effective interventions for promotion of breastfeeding was published by the Centers for Disease Control and Prevention (CDC) in 2005. 8 This resource not only provides the rationale and a review of the evidence for the various interventions listed, it also includes sections on existing quality model programs for each type of intervention and some suggested action steps that an organization or community can take to begin implementation. The guide addresses evidence-based interventions of the following types: Maternity care practices, support for breastfeeding in the workplace, peer support, educating mothers, professional support, and media and social marketing. In addition, there is thorough discussion of interventions for which effectiveness has not yet been established, including countermarketing and the World Health Organization International Code of Marketing of Breast-Milk Substitutes, professional education, public acceptance, and hotlines and other information resources. Despite the current inability to demonstrate the effectiveness for these interventions, they may still be considered promising practices. Saying that effectiveness has not been established is quite different from saying an intervention is not effective. That may indeed be the case, but it is also quite possible that the intervention has yet to be evaluated in a fashion that allows a definitive conclusion to be reached, or that data have been collected but analysis is not yet sufficient to answer this question.
The latest guidance document to emerge is The Surgeon General's Call to Action to Support Breastfeeding, released earlier this year. 9 It goes beyond only reviewing evidence of effectiveness to identify 20 specific actions recommended in various areas for intervention: Mothers and their families, communities, health care, employment, research and surveillance, and public health.
The last several documents cited form a continuum of resources that build on each other in a stepwise fashion, from the basic epidemiology of risk factors and protective factors associated with disease to effectiveness of interventions to mitigate the risks or enhance the protections and then to specific policies and programs one might implement to actualize those effective interventions. That continuum is truly the practice of preventive medicine and public health at its most fundamental level.
Breastfeeding Promotion in Los Angeles County
We have followed the evidence to arrive at the set of recommended actions to increase breastfeeding rates, and the final question is: How are we doing? Let's look at Los Angeles as an example.
Los Angeles is the largest County in the nation in terms of total population, with nearly 10 million residents, larger than 41 states. It is also geographically quite expansive, at over 4,000 square miles, with 88 distinct incorporated cities in addition to unincorporated County areas. Los Angeles has an incredibly diverse population measured in several domains: Racial and ethnic, number of primary languages spoken, and socioeconomic. Some of the wealthiest individuals in the nation live in Los Angeles, whereas approximately 15% of the population (and one-quarter of those under 18 years of age) live below the Federal poverty line. Responsibility for the overall health status of this very diverse population is a multidimensional challenge shared among many public and private sector partners.
Figure 3 10 illustrates an important indicator of future health status: Rates of breastfeeding. Los Angeles County is only slightly under the average for the state of California in terms of breastfeeding initiation in the hospital but continues to fall far short in rates of exclusive breastfeeding compared with our neighboring counties around the state. Los Angeles ranks 43rd out of 58 California counties when it comes to this key indicator. 10 Despite the current low ranking, Los Angeles County is making significant forward progress and has had several policy and program successes the past few years in the area of breastfeeding promotion.
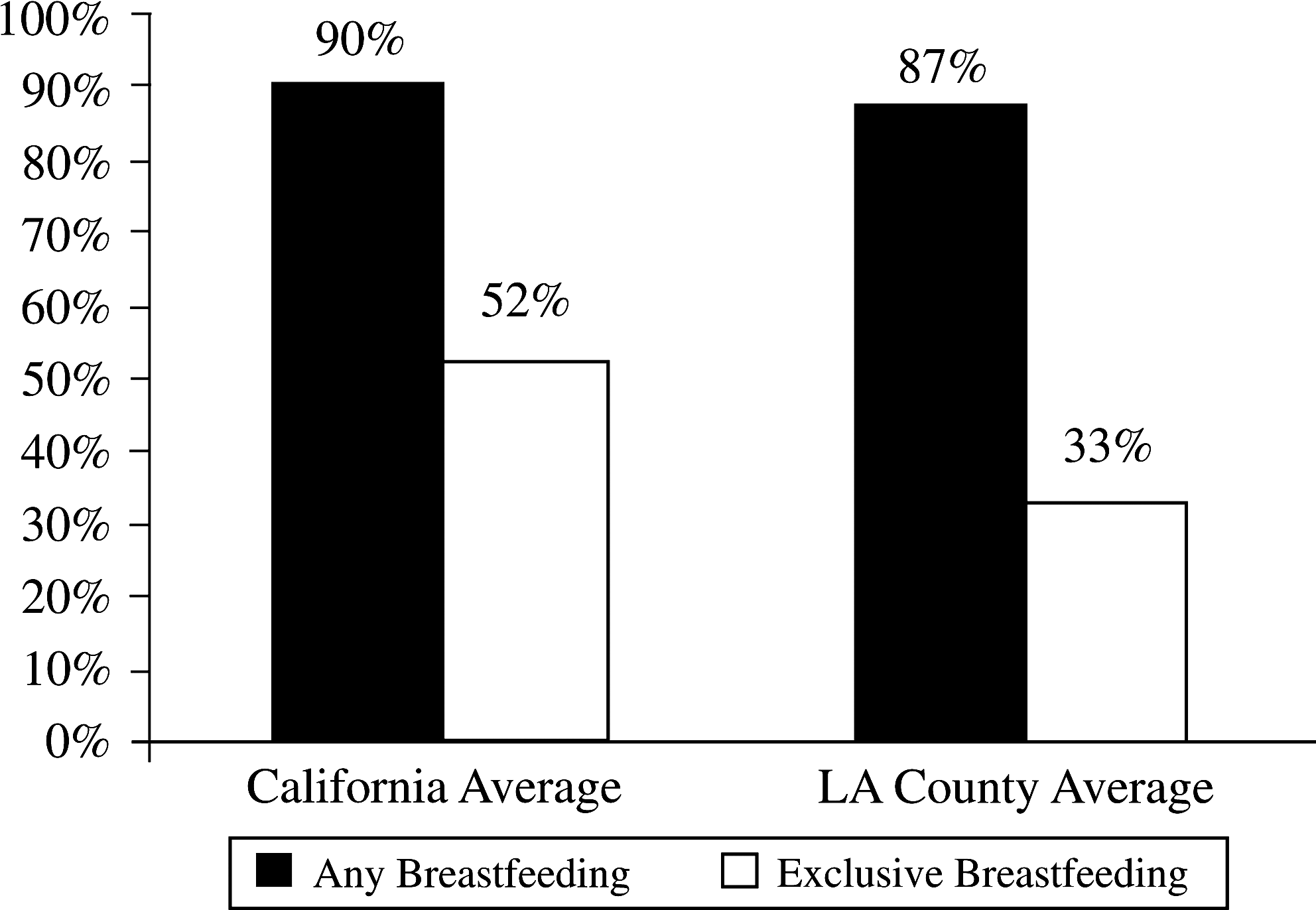
In-hospital breastfeeding rates for California and Los Angeles County, 2009. Data are from the California Department of Public Health. 10
Hospital maternity care practices
There are multiple efforts occurring simultaneously to promote the Baby-Friendly Hospital Initiative in Los Angeles birthing facilities. As this article was being written, there were six hospitals in Los Angeles County that had successfully received Baby-Friendly designation from Baby-Friendly USA, but this is a small percentage of our almost 60 birthing hospitals, and there are multiple efforts occurring simultaneously in various sectors of the local healthcare community in order to boost that number.
One such effort has been funded by the First 5 Los Angeles Commission, on which the Public Health Director sits. The First 5 Commission was established in a California ballot initiative to tax tobacco sales and reinvest the funds to improve the health, safety, and school readiness of young children. Each county has an independent commission. First 5 Los Angeles funded a Baby-Friendly initiative in 2009, making individual grants of nearly $500,000 each available to hospitals with exclusive breastfeeding rates below the County average. The money may be used for training and other administrative costs necessary for the hospital to transform its systems and practices to achieve the Baby-Friendly designation. In order to achieve this designation, the hospital must demonstrate to the Baby-Friendly USA organization its ability to provide all the recommended elements of care as outlined in the Ten Steps to Successful Breastfeeding in Hospitals. Currently 17 hospitals have been awarded grants, with funding available for three more institutions. The hospitals are funded for 3 years and are expected to complete their pathway to certification in that time period. The 17 currently funded hospitals combined account for approximately 50,000 live births per year, or slightly over one-third of all live births in the County, so the potential impact on health outcomes from seeing all these institutions succeed in improving their breastfeeding rates is enormous. Furthermore, 80% of those 50,000 births are paid for by Medicaid; in other words, the large majority of those births are occurring in low-income families who will receive more relative health benefit from improved breastfeeding practices compared with middle- and higher-income Angelenos.
In 2010, the Los Angeles County Department of Public Health (DPH) was fortunate to receive Communities Putting Prevention to Work (CPPW) grants from the CDC, made possible as part of the American Recovery and Reinvestment Act of 2009. The Department received over $30 million total for tobacco and obesity prevention efforts and as part of the local obesity initiative, named RENEW LA County, has committed to assisting the three County public hospitals toward achieving Baby-Friendly designation. Funds are being used to provide intense, tailored, on-site technical assistance through consultants who have experience with the Baby-Friendly process. Top-down support was garnered, beginning with commitment from the County Board of Supervisors and the Director of the Department of Health Services, which administers the three public hospitals that provide obstetric services, and moving onward to include the three hospital Chief Executive Officers. Prior to obtaining these commitments, despite a great deal of education to hospital staff and some consultation from lactation experts over previous years, these hospitals had not significantly increased their breastfeeding rates.
The process in the three County hospitals has been highly successful. One of the hospitals received their site visit from Baby-Friendly USA in June 2011, only a little over a year since the CPPW grant cycle started. Approximately 2 weeks later the hospital was informed that it passed the site visit, becoming the sixth birthing facility in Los Angeles County to achieve Baby-Friendly designation and the first public hospital to do so. The other two County hospitals are on schedule to be ready for site visits in late 2011 or early 2012. All three should complete the process within the 2-year grant cycle, significantly compressing the usual 3-year period. The three County hospitals do not account for a large proportion of live births in the County, although almost all those births occur in low-income families. What makes this achievement significant is it demonstrates the benefit of providing technical assistance not only on lactation issues, but also on systems change, program planning and management, and quality improvement projects. The latter areas are often where the facility is most lacking expertise and where obstacles to continued progress develop. Providing assistance in these areas specifically is what allowed the project to move forward at an accelerated pace.
RENEW LA County focuses on the three County Hospitals, but DPH is also collaborating with a local community coalition, the Breastfeeding Task Force of Greater Los Angeles, to create Regional Hospital Breastfeeding Consortiums so that all hospitals in the County that wish to can participate in a local learning collaborative and get much of the support and assistance they need to navigate the pathway to Baby-Friendly certification. One consortium has been operating for over a year, and two others have been recently launched in other regions of the County.
Outpatient community healthcare settings
Moving beyond the hospital to the community clinic setting, a pilot project has been launched that has already shown encouraging results. The Comprehensive Perinatal Services Program (CPSP) is a state-administered enhanced set of services available to clinicians providing obstetric care to women enrolled in Medicaid. The enhanced services include education and support in the areas of nutrition, lactation, and mental health. Education and training for all professional office staff are included as part of the program. Public health nurses in DPH who administer CPSP locally noted one clinic linked to a community hospital had very low rates of exclusive breastfeeding, even among those women who had expressed their intent to exclusively breastfeed during prenatal visits. Ironically, the clinic staff had very little knowledge about the support services offered by the Women, Infants, and Children (WIC) program, despite the fact that there was a WIC site across the hall from the clinic. Similarly, WIC staff did not know that personnel at the adjacent clinic were already knowledgeable about breastfeeding and enthusiastic about helping their patients breastfeed, including offering their patients a prenatal breastfeeding class. Unaware of these efforts at the clinic, WIC staff had even been referring clients to another community hospital further away from the home institution that supported more Baby-Friendly practices. As a result of this assessment, the clinic instituted a two-part pilot intervention. First, clinic staff focused on bringing women back early for their initial postpartum visit: Within 1–2 weeks instead of the usual 6 weeks. As a CPSP provider, the clinic can be reimbursed for the additional visit as long as it is focused on CPSP-enhanced services. The early visit gave the clinic staff the opportunity to reinforce the importance of exclusive breastfeeding and identify patient needs for further support. Second, clinic staff collaborated closely with the nearby WIC office and were encouraged to refer clients to WIC for any breastfeeding problems and to assist in maintaining exclusive breastfeeding.
How did this approach work? The baseline rate in the pilot sample was 24% exclusive breastfeeding. The post-intervention measurement was 55%. The community hospital affiliated with the clinic was so impressed with these results that it plans to expand the program to its other four outpatient clinics, and the public health nurses look to recruit clinics associated with other hospitals.
Worksite lactation support
In the area of workplace lactation accommodations, legislation in California has long supported nursing mothers in the workplace. In fact, the California legislature passed a law in 2001, well before the Patient Protection and Affordable Care Act of 2010 established Federal law requiring worksite accommodations for breastfeeding employees. In addition, the California statute provides greater protections than the newer Federal law. The Federal language applies only to non-exempt employees and allows employers with fewer than 50 employees to opt out if they can demonstrate a financial hardship to compliance. The California law applies to all employers and all employees. The Federal law extends rights up to 1 year after the infant's birth, whereas California has no such age limit. Fortunately, the Federal language explicitly states that it does not preempt state law that provides greater protection. Despite these successes in the legislature, adoption of the requirements by all workplaces remains a long, arduous process. As part of the aforementioned CPPW grant, DPH committed to goals related to workplace lactation. One objective is to assist at least eight of the 37 departments in the Los Angeles County government to adopt and implement workplace lactation policies. Again, support was initially garnered from the County Board of Supervisors. As a result, the County Department of Human Resources is currently finalizing a policy that will apply to all County departments simultaneously. The County government is the largest employer in Los Angeles County, with nearly 100,000 employees, and its policies often influence other large public employers. In addition to County government, a second objective was adopted to find at least two other large local employers that would also adopt and implement similar policy. This effort, too, has been successful. The City of Los Angeles (50,000 employees) has signed a letter of intent to adopt a workplace lactation policy, as has Associated Students at California State University Northridge (CSUN), an independent employer at the University involved in student governance. Associated Students has adopted a lactation policy for their 400 employees and by extension may adopt a student policy ensuring lactation rights for the 30,000 students on campus. This is also a first step toward influencing the state employment arm at CSUN, which includes another 5,000 employees, and ultimately the entire 23-campus statewide California State University system, which encompasses approximately half a million faculty, staff, and students.
Peer support
In addition to its large-scale investment to promote Baby-Friendly hospitals, First 5 Los Angeles has also recently approved a proposal to allocate up to 2 million dollars for mini-grants to community-based organizations to be used toward establishing up to 100 neighborhood peer support groups for new mothers. These peer groups can focus on multiple needs for parents of infants and young children, including breastfeeding support, perinatal mental health needs, healthy child development, and parenting skills.
Continuing Challenges: Breastfeeding Disparities
Certainly several challenges remain that limit the success of our local breastfeeding promotion efforts. The one that will be focused on in this final section is that of breastfeeding disparities, a great concern in Los Angeles. Figure 4 10 illustrates exclusive in-hospital breastfeeding rates in Los Angeles County stratified by race/ethnicity and demonstrates the marked disparities for all minorities of color compared with whites. The situation is rather ironic in that breastfeeding can play an important role in addressing and reducing health disparities, but is itself an example of a significant disparity. A large contributor to this dilemma is the deeply ingrained biases against breastfeeding in some communities. It is necessary to alter the social norms and battle the lack of knowledge that exists around breastfeeding throughout the population, but especially in communities with particularly low rates of exclusive breastfeeding. In addition, it is important to recognize that not all mothers have the same flexibility of schedule for breastfeeding, with lower-income women and those without partners having more barriers to exclusive high-duration breastfeeding. One aspect of addressing these disparities is making special efforts to recruit and work with hospitals in communities serving minorities and lower-income neighborhoods to adopt Baby-Friendly policies.
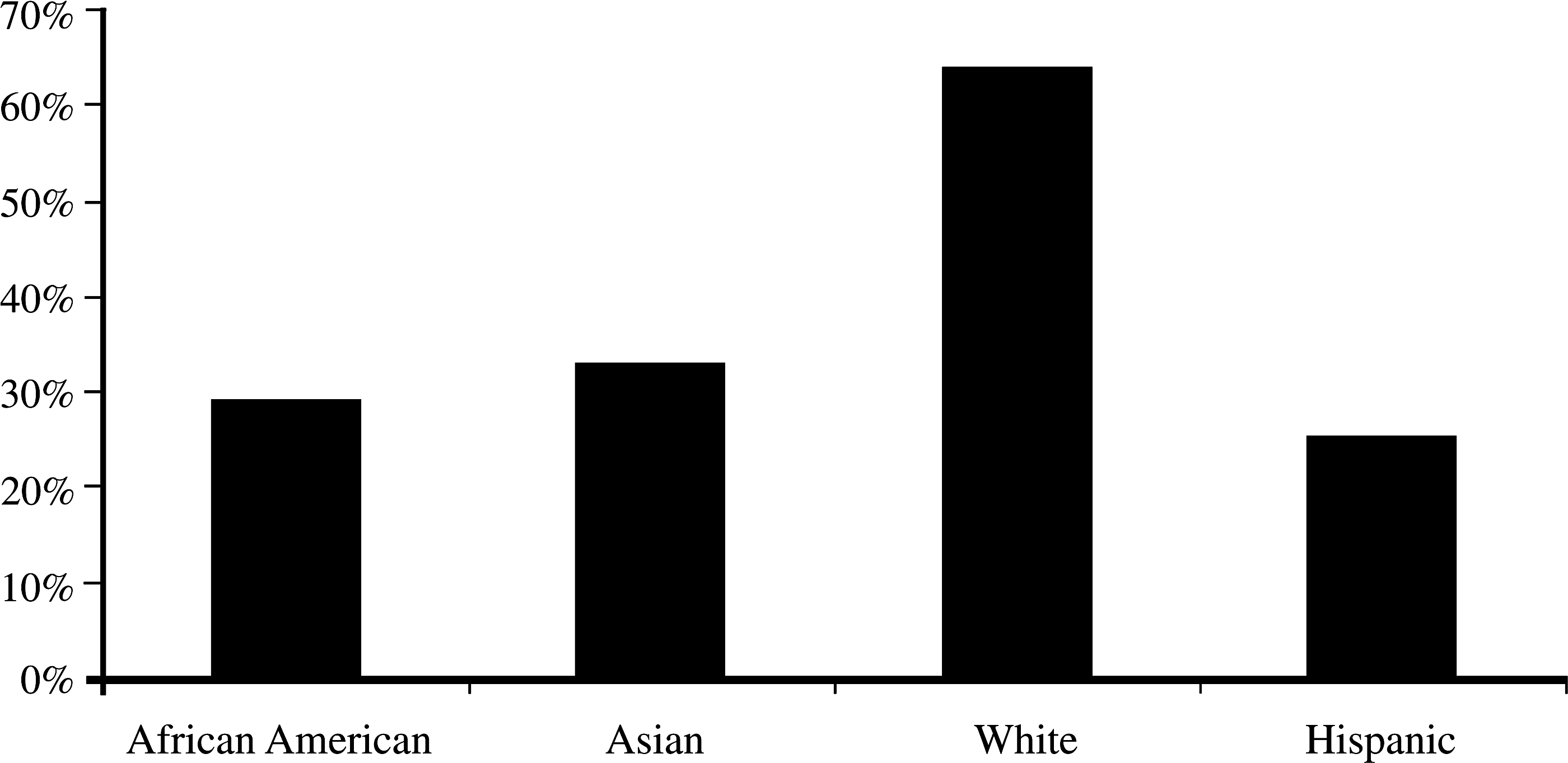
In-hospital exclusive breastfeeding rates by race/ethnicity for Los Angeles County, 2009. Data are from the California Department of Public Health. 10
Intervention is also needed directly within the communities and populations that have low breastfeeding rates. Recalling the evidence-based interventions from the CDC Guide presented earlier, 8 one of the areas deemed effective was media and social marketing. There is a social marketing program currently in development that will promote breastfeeding in the African American community called “Soul Food for Your Baby.” DPH is currently seeking funding for implementation of this project. Ideally, the project would not only educate members of the target community, but also reset the social norms that exist surrounding breastfeeding through both mass media and social media. A high priority must also be given to Latina mothers who encompass over 60% of the live births in Los Angeles. At the same time, effective ways to reach into the many different Asian communities must be identified. One size does not fit all.
Breastfeeding Evens the Playing Field
Reducing disparities in breastfeeding rates is crucial for reducing various other disparate health outcomes, which brings us full circle back to breastfeeding as prevention. The following quote provides a wonderful perspective on the mission that all breastfeeding advocates are dedicated to fulfill: 11
Breastfeeding is a natural “safety net” against the worst effects of poverty..It is almost as if breastfeeding takes the infant out of poverty for those first few months in order to give the child a fairer start in life and compensate for the injustice of the world into which it was born.
The goal is not simply about promoting breastfeeding, it is about leveling the playing field to give each newborn the right start, one commensurate with his or her full potential. We must do all we can to make this evidence-based natural practice the easy choice. Nature showed us the right way. So, let us together heed one of nature's best lessons.
Footnotes
Acknowledgments
The authors wish to thank Stephanie Caldwell, M.P.H., and Boyd Jackson for their valuable assistance in preparing the figures for this article and presentation.
Disclosure Statement
No competing financial interests exist.