
Abstract
Abstract
Background:
The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) has provided free infant formula while simultaneously attempting to promote breastfeeding. This article analyzes the cost structure of WIC food packages in relation to breastfeeding.
Methods:
The analysis provides 2010 estimates for the cost and utilization of each of the WIC food packages for pairs of infants and their mothers. New food packages were introduced in all states by 2009 and were intended to promote breastfeeding. The analysis accounts for the composition of the new food packages, although utilization projections predate the implementation of those packages, so current rates of breastfeeding may be understated.
Results:
The projections suggest that just under 74% of infant participants are estimated to receive food packages associated with exclusive formula use. Relative to food packages for mother–infant pairs who exclusively breastfeed, the exclusive formula packages are around 25% more expensive for infants in the first 6 months of life but 64% cheaper during the second 6 months.
Conclusions:
Simulations suggest that the achievement of the Healthy People 2020 breastfeeding targets among WIC participants would have a minimal effect on food package costs. Simulations for extreme cases (e.g., all fully breastfeeding for 1 year) suggest that food package costs could be reduced by 18% if all WIC mother–infant pairs engaged in exclusive breastfeeding for the first 6 months, followed by exclusive formula use in the next 6 months. A 38% reduction could be achieved if all mother–infant pairs received the partial breastfeeding packages.
Introduction
WIC has recently provided between 57% and 68% of all infant formula sold in the United States, 3 suggesting that the program may be at least partially responsible for the low rates of breastfeeding found here relative to other nations. 4 Given substantial evidence of the health benefits of breastfeeding, 5 efforts have been made to improve rates of breastfeeding among WIC participants. The analysis below provides evidence regarding the likely food cost effects for WIC in light of possible changes in rates of breastfeeding.
Breastfeeding promotion in the United States dates to the 1979 Surgeon General's report on “Healthy People” 6 and the subsequent U.S. Department of Health and Human Service's “Healthy People 2010” initiative 7 and current “Healthy People 2020” initiative. 8 Each of these initiatives included national breastfeeding targets, and a host of additional efforts are intended to promote breastfeeding as well.4,9,10
From its inception, mothers of infants could choose whether or not to receive infant formula through WIC. Although WIC was likely not the only factor involved, mothers of infants participating in WIC were engaging in breastfeeding when the child was 6 months of age at less than half the rate of non-participating mothers as of 1990 (8.6% compared with 17.8%, respectively). 11
Whether because of national initiatives, changing norms around breastfeeding, or relatively continuous attempts to promote breastfeeding among WIC participants,1,12 rates of breastfeeding at 6 months among WIC recipients climbed steadily throughout the 1990s, from the 8.6% rate in 1990 to 20.3% in the year 2000. 11
In 2005, the National Academy of Medicine's Committee to Review the WIC Food Packages recommended new guidelines for WIC food packages. Among other suggested revisions, they recommended enriching the food packages provided to breastfeeding mothers and their infants and scaling back the amount of infant formula provided to infants who were either partially breastfed or not breastfed. 13 The new food packages were introduced nationwide by 2009.1,3
The new food packages include separate packages for mothers and their infants, but these are combined here because mothers' decisions regarding breastfeeding simultaneously determine both mother and infant packages. Although slightly inaccurate, the terms applied here to the different food packages include “exclusive formula use,” “partial breastfeeding,” and “exclusive breastfeeding.” The inaccuracy stems from the fact that for months 6–11.9, all infant packages are supplemented with foods in addition to formula and breastmilk.
Reauthorization of WIC in 2010 included intensive efforts to promote breastfeeding. 14 These efforts responded to continued low rates of breastfeeding among WIC recipients. Figure 1 provides evidence from the Centers for Disease Control and Prevention (CDC) of this “WIC gap” in rates of breastfeeding. It is important that, although rates of breastfeeding among WIC recipients are low, they show relatively continuous improvement over time.

Breastfeeding and Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) receipt. Data were obtained from the National Immunization Survey, 2000–2007. 15
Methods
To understand WIC food package costs requires an understanding of infant formula rebates. In 1987, the state of Tennessee requested that formula producers bid for an exclusive contract to supply infant formula to the state's WIC program. In exchange for the exclusive contract, the state received a rebate from the producers for each unit of formula sold through WIC. The contracts quickly spread to other state programs, and, by the mid-2000s, the rebates were such that WIC programs receiving the rebates paid an average of 9% of the wholesale price, 3 plus the retail markup.
An asymmetry regarding breastfeeding and formula use is also crucial for understanding the utilization of WIC food packages and resulting costs: Mothers who stop breastfeeding a child at any point are not likely to breastfeed that child again. 16 As a result, it is assumed here that the proportion of mothers of infants participating in WIC who select food packages for exclusive breastfeeding will tend to fall, and will never rise, between the time a child is born and the time the child reaches 1 year of age.
The 2010 cost of the new WIC food packages is estimated using 2006 prices 17 and food prescription amounts, 18 which are corrected for inflation using the 2007–2010 food item-specific annual Consumer Price Index-Unadjusted, 19 with three exceptions. In terms of prescription amounts, during implementation of the new food packages, it was decided that all mothers of infants (and not just those who are exclusively breastfeeding) would receive a $10 voucher for fruits and vegetables, and the maximum allowable amounts of formula were reduced slightly. 18 In addition, the current cost of infant formula to WIC is treated differently. Most WIC infant formula contracts hold for 4-year periods with prices constant for the period. According to a recent report from the U.S. Department of Agriculture, comparing prices in contracts effective in December 2008 with those in prior contracts revealed an increase of 73% in real net wholesale prices. 3 However, infant formula costs to WIC include both the wholesale price post-rebate and a retail markup. To avoid overstating the inflationary effects of the increase in real net wholesale prices, it is assumed that they accounted for only 30% of formula costs to WIC as of 2006, a figure that is reasonably cautious given available state-level figures. 20 All cost calculations are for powdered infant formula, which is reasonable given that both liquid milk-based formula and liquid soy-based formula are small and shrinking components of the WIC program. 3 Furthermore, part of the 73% increase had already occurred by 2006, 3 so the increase is reduced to 50% for the analysis. Under these assumptions, the 2006 price of formula to WIC is inflated by a factor of 15% to generate 2010 figures. Note that the 15% figure is cautious because it does not account for any increase in the retail markup during the period. The analysis is also simplified by ignoring food packages prescribed as a result of certain medical conditions (i.e., food package 3), following the practice of the National Academies committee. 13
Estimates of current food package utilization are for the 2010 fiscal year starting October 1, 2009 and ending 1 year later. 18 However, the projections were generated for a report released in 2007, so the figures do not account for any subsequent shift in breastfeeding behavior—including any changes generated by the introduction of the new WIC food packages.
The information on per-participant food package costs is combined with projected monthly participation figures to obtain total monthly WIC costs for mother–infant pairs. It is not known precisely how many infants enrolled in WIC are breastfed across each month of age, so those figures are estimated as follows.
CDC data for 2007 show that 25.5% of WIC infants are exclusively breastfed up to 3 months of age, a figure that falls to 9.2% by 6 months of age. 21 At least partial breastfeeding after birth occurs at a rate of 67.5% among WIC participants, with the figure falling to 33.7% at 6 months and 17.5% at 12 months. 22 It is estimated (see Table 2 for figures) that 42.3% of infants aged 0–3.9 months engaged in at least partial breastfeeding, with the figure falling to 23.6% for 4–5.9 months and to 15.5% for 6–11.9 months. By extension, the percentage of infants exclusively breastfed is 27.0% in months 0–3.9, 15.1% in months 4–5.9, and 9.9% in months 6–11.9.
For the final 6 months of the WIC coverage period for each infant, the figures for WIC utilization and breastfeeding among WIC participants in the CDC data are very close. The CDC figure for exclusive breastfeeding at 6 months is 9.2%, whereas the comparable WIC utilization figure for months 6–11.9 is 9.9%. The CDC figure for at least partial breastfeeding is 17.5% at 1 year, whereas the comparable WIC utilization figure is 15.5%. Given these similarities, it is assumed that rates of partial and exclusive breastfeeding are constant over the 6–11.9-month age range.
Because the CDC data find a marked drop-off in breastfeeding rates between birth and 3 months and 6 months, it is assumed that there is a linear, negative relationship between the infant's age and rates of exclusive breastfeeding through month 5. Given the mean rate of exclusive breastfeeding is 27.0 during months 0–3 and 15.1 in months 4–5, rates per month can be estimated by substituting in those figures as mean rates for months 1.5 and 4.5, respectively, to solve the following equation: Breastfeeding rate=Constant – X(Months of Age). For exclusive breastfeeding, the constant term is 32.96, and the slope X is 3.97 (implying that rates of exclusive breastfeeding decline by around 4% per month), yielding the exclusive breastfeeding figures reported below.
Partial breastfeeding rates can be estimated in the same fashion, using the fact that 15.3% of infants are partially breastfed during months 0–3 and 8.5% are during months 4 and 5. In the partial breastfeeding equation, the constant term is then 18.7, and the slope X is 2.27, yielding the partial breastfeeding rates described below.
Rates of exclusive formula use are estimated as the remainder after accounting for partial and exclusive breastfeeding.
Five simulations are performed to better understand the effects of any changes in breastfeeding behavior, most of which address potential increases in breastfeeding. The first concerns the projected effects of WIC participants meeting the Healthy Families 2020 breastfeeding target rates. The other four simulations address extreme cases.
The Healthy Families 2020 simulation requires some discussion. The Healthy People 2020 objectives for breastfeeding 23 include breastfeeding initiation rates of 81.9% and at least partial breastfeeding at the rates of 60.6% at 6 months and 34.1% at 1 year. Targets for exclusive breastfeeding are 46.2% at 3 months and 25.5% at 6 months. For exclusive breastfeeding, the 3-month figure can be applied to month 2 of WIC, and the 6-month figure to month 5. Plugging these into the breastfeeding rate equation for months 0–5 yields a constant term of 60 and a slope X of 6.9, which, in turn, yield exclusive breastfeeding targets described below.
To achieve the target for at least partial breastfeeding at a rate of 81.9% in the first month, the sum of partial and exclusive breastfeeding must equal the 81.9% figure, yielding a target partial breastfeeding rate of 21.9% in month 0. Similarly, the target at 6 months (applying to WIC month 5) for any breastfeeding of 60.6% requires that partial breastfeeding occur at a rate of 35.1%. Note that it is reasonable to suppose there is a rising rate of partial breastfeeding because mothers who were exclusively breastfeeding may switch to partial breastfeeding. Applying these figures to the breastfeeding equation yields a constant term of 21.9 and a slope X of −2.64. To achieve the target of 34.1% for at least partial breastfeeding by the end of the first year, again assuming a uniform distribution of breastfeeding between months 6 and 11, the partial breastfeeding rate would need to be 24.2%.
Results
The estimated 2010 cost of WIC food packages for mother–infant pairs is provided in Table 1. The most expensive package combinations are for exclusive breastfeeding during infant months 6–11.9 and for partial breastfeeding during months 6–11.9. The least expensive packages are for exclusive formula use across months 6–11.9 and for exclusive breastfeeding during months 0–5.9.
Note that formula is restricted for partially breastfeeding infants during month 0, bringing the cost down to $43.12 during that time. Data are from Institute for Women's Policy Research calculations using 2006 food package prescriptions and food item costs from the U.S. Department of Agriculture Food and Nutrition Service in 200717,18 and archived Consumer Price Index-Unadjusted inflation rates from the Bureau of Labor Statistics in 2007–2010. 19
It has been projected that a total of 1.2 million mothers of infants and 2.2 million infants participated in WIC during FY2010 (Table 2). For partial and exclusive breastfeeding, the numbers of participating mothers are similar to, although slightly lower than, the numbers of infants. It is possible for low-income, single fathers to enroll in WIC. However, it would seem reasonable for them to select the exclusive formula packages, leaving the difference between mother and infant enrollment with partial or exclusive breastfeeding an open question. It may be that accounting errors are involved, or that some mothers (perhaps with limited literacy) believe that their infant qualifies but that they, themselves, do not. For full formula packages, the total number of participating mothers is less than half as large as for infants because they are not provided with a mother package beyond 5.9 months.
Data are from the U.S. Department of Agriculture Food and Nutrition Service in 2007. 18
When the information on per participant cost provided in Table 1 is combined with projected monthly participation figures from Table 2, total monthly WIC food costs for mother–infant pairs follow, as in Table 3.
Data are from Institute for Women's Policy Research calculations using 2006 food package prescriptions and food item costs from the U.S. Department of Agriculture Food and Nutrition Service in 200717,18 and archived Consumer Price Index-Unadjusted inflation rates from the Bureau of Labor Statistics in 2007–2010. 19
The largest source of expenditures is for infants aged 6–11.9 months who are exclusively formula feeding, at over $35 million per month, which is partly a function of the large age range included (6 months) as well as the large number of infants on the exclusive formula package at that time. The smallest figure is for partially breastfed infants aged 4–5.9 months, which is partly a function of the small age range included (2 months) and the small proportion of infants receiving the package.
The column on the far right of Table 3 provides total monthly costs for the three feeding approaches. It demonstrates that more than two-thirds of WIC mother–infant pair food costs (70%) are associated with exclusive formula packages. The total estimated cost for all three types of mother–infant food packages is approximately $112 million per month.
Given that projected food package utilization figures were generated prior to implementation of the new food packages, it is likely that current rates of breastfeeding are higher.
Meeting the Healthy People 2020 objectives
Using the simulation method described above results in monthly cost figures as reported in Table 4. The grand total is $111 million per month or approximately $1.3 billion per year, a figure that is virtually identical to current estimated food expenditures by WIC for mother–infant pairs. Behind that similarity lie dramatic reductions—by more than half—in expenditures on exclusive formula packages for the first 6 months, in tandem with proportionally smaller increases in expenditures on exclusive breastfeeding packages for the first 6 months, and an almost threefold increase in expenditures on packages for infants partially breastfeeding for a full year.
Data are from Institute for Women's Policy Research calculations using 2006 food package prescriptions and food item costs from the U.S. Department of Agriculture Food and Nutrition Service in 2007,17,18 archived Consumer Price Index-Unadjusted inflation rates from the Bureau of Labor Statistics in 2007–2010, 19 and Healthy People 2020 objectives for breastfeeding. 23
Extreme cases
Other simulations consider cases where either all of the mothers exclusively breastfeed, all partially breastfeed, or all exclusively formula feed or they switch from exclusive breastfeeding to exclusive formula use at 6 months. The resulting monthly food package costs to WIC are provided in Figure 2.
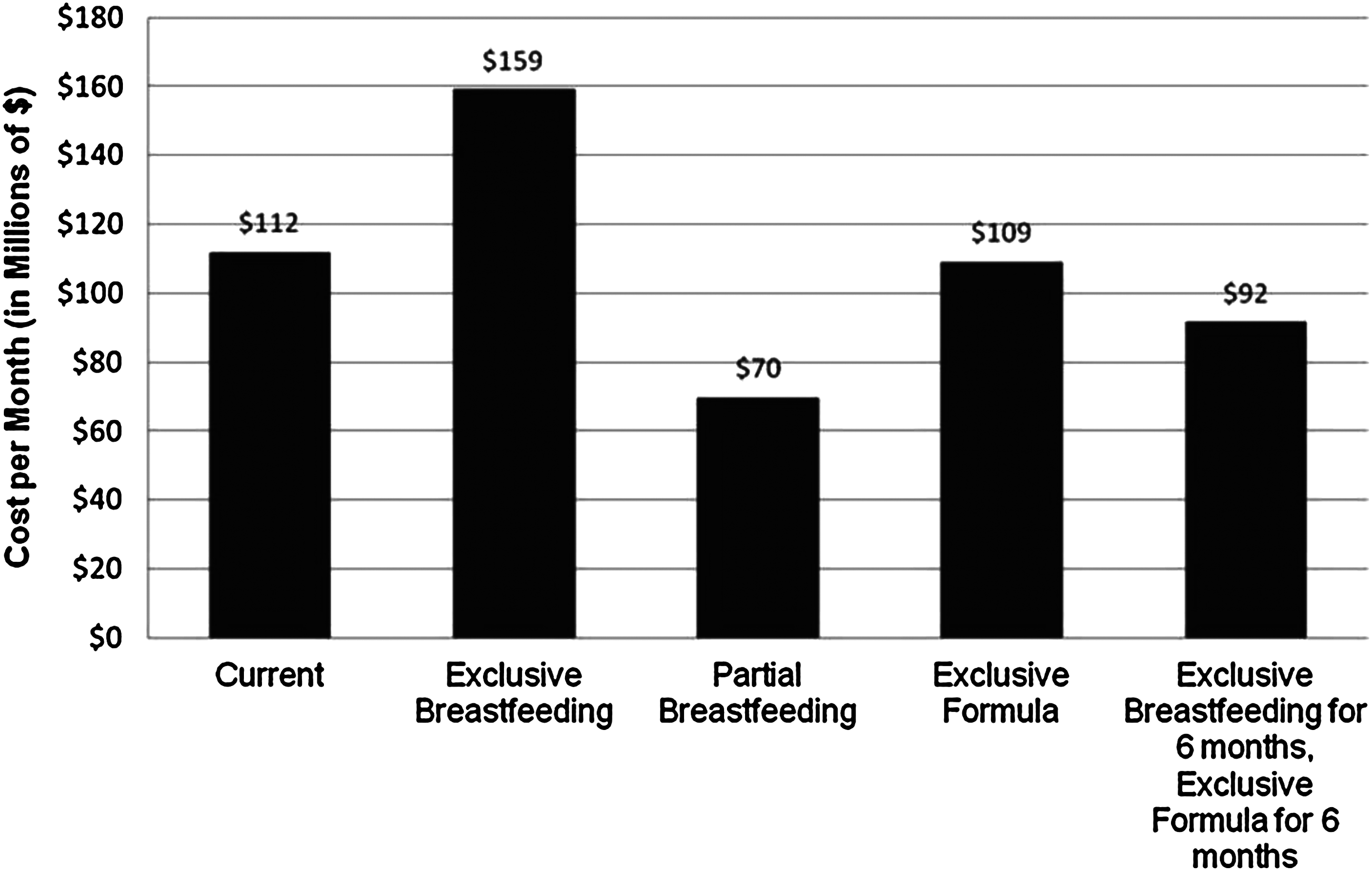
WIC food expenditures for mother–infant pairs, extreme cases. Data are from Institute for Women's Policy Research calculations using 2006 food package prescriptions and food item costs from the U.S. Department of Agriculture Food and Nutrition Survey in 200717,18 and archived Consumer Price Index-Unadjusted inflation rates from the Bureau of Labor Statistics in 2007–2010. 19
The highest amount is for exclusive breastfeeding. If all WIC mother–infant pairs were to use these packages, food costs would rise by 40%. On the other hand, exclusive formula use would result in only a minimal shift in WIC food package costs. The high cost of exclusive breastfeeding is, not surprisingly, driven by the high costs for the mother–infant pair packages in the second 6 months; indeed, if the mothers were to use exclusive breastfeeding packages for the first 6 months and then switch to exclusive formula use, costs would fall to $92 million per month, for an 18% reduction or an annualized saving of $240 million. More surprising is the finding that the low-cost option involves mothers consistently utilizing the partial breastfeeding packages. This strategy would reduce monthly costs to $70 million, generating a 38% reduction in the costs of the food packages.
Discussion
Not considered in the analysis above is the way in which food packages are viewed by participating mothers. If mothers were to purchase the WIC food packages in retail stores, the retail price of infant formula would drive up the value of relevant packages. For exclusive formula use, the value of the packages rises to approximately $129 in months 0–3, $139 in months 4 and 5, and $92 in months 6–11 (calculations are based on a retail price of $15 for 126 fluid ounces of powdered infant formula at the Washington, DC Safeway store [Columbia Road location], June 5, 2011). As a result, participating WIC mothers of infants face a choice between the exclusive formula and breastfeeding food packages wherein the retail value of the former is over 150% greater in months 0–5 (compare figures here to those in Table 1) but is then lower for the next 6 months.
The divergence between costs to the WIC program and the retail value of WIC food packages—driven by infant formula rebates—presents a quandary. If the retail value of WIC food packages for exclusive breastfeeding was driven up to figures for the exclusive infant formula packages during the first 6 months of an infant's life to enhance the incentives for participants to breastfeed, costs to WIC for the exclusive breastfeeding food packages would need to more than double (i.e., from $48 to $129 or $139 per month).
Conclusions
Figures presented here suggest that exclusively breastfeeding mother–infant pairs compared with exclusive formula-using pairs save $12 per pair for each of the initial 4 months and $15 for each of the next 2 months (see Table 1). The cost structure exhibits a dramatic shift for the next 6 months, with exclusive formula-using pairs costing $69 less per month than exclusive breastfeeding pairs.
Fortunately, the relevant incentive effects outlined above are likely modest, particularly given the historical context for the recent introduction of the new WIC food packages. That context includes the fact that rates of breastfeeding among WIC participants have been rising for decades, as mentioned above, and there is little reason to believe that trend will reverse. Additionally, the new food packages for exclusive breastfeeding are more generous than those provided previously, 13 so the incentives to avoid breastfeeding provided by differences in the value of the food packages were reduced. Furthermore, other components of the 2010 WIC reauthorization (e.g., expanded peer counseling) should improve rates of breastfeeding among participants, as will other efforts to promote breastfeeding across the United States.
Footnotes
Acknowledgments
Thanks to Youngmin Yi, Research and Program Assistant at the Institute for Women's Policy Research, and to Sarah Towne, Intern at the Institute for Women's Policy Research, for valuable assistance, to participants in the Third Annual Breastfeeding Summit for feedback, and to the W.K. Kellogg Foundation for funding.
Disclosure Statement
No competing financial interests exist.