
Abstract

Introduction
New York State (NYS) is close to meeting the Healthy People 2020 3 (HP2020) goal for breastfeeding initiation (infants fed any breastmilk), which is 81.9%. In NYS, 76% of new mothers initiated breastfeeding in 2009 (Bureau of Biometric and Health Statistics, NYS Department of Health, unpublished data). NYS, however, is far from meeting the HP2020 3 goals (>70%) for early exclusive breastfeeding. In NYS only 52% of healthy infants were fed exclusively breastmilk during the first 2 days of life (Bureau of Biometric and Health Statistics, NYS Department of Health, unpublished data). Only 16 of the 135 hospitals providing maternity services in NYS met this exclusive breastfeeding goal in 2009. The practice most responsible for reduced levels of exclusive breastfeeding in hospitals is formula supplementation of breastfed infants. NYS has one of the highest rates of formula supplementation of breastfed infants before 2 days of age in the country. 4 Formula supplementation of breastfed infants adversely affects exclusive breastfeeding, resulting in lower prevalence at both 3 and 6 months (Fig. 1).

Breastfeeding metrics: Healthy People 2020 3 (HP2020) and New York State (NYS). The sources of the NYS data are unpublished data from the Bureau of Biometrics and Statistics, NYS Department of Health, 2009, for any and exclusive breastmilk at 2 days and the National Immunization Survey, 2011, 5 for exclusive breastmilk at 3 and 6 months.
There are large disparities between NYS hospitals in their rates of breastfeeding initiation and exclusivity. Breastfeeding policies and maternal and infant care practices of hospitals have a profound effect on the breastfeeding success of their patients, even months later.5,6 A mother's in-hospital experience, and its impact on breastfeeding success, cannot be overstated. It is, however, only one component of the prenatal–perinatal–postnatal continuum experienced by mothers in the United States. Each stage presents unique barriers and challenges. NYS has made significant efforts to reduce barriers to breastfeeding, particularly concerning exclusive breastfeeding in hospitals by (1) enacting policies, regulations, and legislation that mandate mothers have the support needed to successfully breastfeed, (2) improving the monitoring, reporting, and transparency of infant feeding practices in hospitals, and (3) increasing implementation of evidence-based best practices and policies in healthcare settings.
Policies, Regulations, and Laws
NYS has a number of policies, regulations, and laws that support and protect a woman's right to breastfeed. As early as 1994, NY Civil Rights Law, Article 7, §79-e 7 was enacted to protect a mother's right to breastfeed her child in any public or private location. More recent legislation includes NY Labor Law, Article 7, §206-c 8 (2007), the Nursing Mothers in the Workplace Act, which guarantees mothers the right to unpaid time and private space (not a restroom) to express breastmilk up to 3 years after the birth of their child.
Regulations and legislation pertaining to hospital maternity practices have been a recent focus in New York. NY Codes, Rules and Regulations, NYCRR, Title 10, 405.21 9 requires hospitals to have written policies and procedures that assist and encourage women to breastfeed, consistent with the World Health Organization/UNICEF's Ten Steps to Successful Breastfeeding 10 (Table 1). In addition, effective January 1, 2011, NYS amended Hospital Regulations (NYCRR, Title 10, Subpart 712 9 ) covering standards for construction of hospitals. According to the new 2010 Guidelines for Design and Construction of Health Care Facilities, 11 “when there is rooming-in [of a newborn infant with his/her mother], the number of bassinets in the nursery can be reduced, but the nursery cannot be eliminated.” Reducing nursery size encourages rooming-in and enhances opportunities for feeding on demand, an important component of breastfeeding success. 12
The source for these guidelines is the 1989 World Health Organization/UNICEF statement. 10
NYS passed NY Public Health Law, Article 25, Title 1, §2505-a, 13 the Breastfeeding Mothers' Bill of Rights, in 2008. This law guarantees the rights to specific breastfeeding care prenatally, during hospitalization, and post-hospital discharge. The portion of the law that addresses maternal healthcare facilities dictates certain maternity care practices during the birth hospitalization and codified and strengthened existing hospital regulations (NYCRR 405.21 9 ). This law became effective May 1, 2009. A copy of a women's rights endowed by this bill must be posted on the NYS Department of Health website (in eight languages) and in every maternity hospital. They must also be given to all pregnant women who attend prenatal classes, pre-book at a hospital, or are admitted to a hospital for childbirth.
In August 2009, the NYS Health Commissioner, under New York Public Health Law, Article 28, Title 1, §2803-j, 14 expanded the list of hospital measures that are required to be part of the mandated Maternity Information Brochure. Hospital-specific rates of breastfeeding during the newborn hospital stay were added to the Brochure, which is updated annually and posted on the NYS Department of Health public website. The law also requires hospitals to distribute the brochure to all pregnant women and new mothers as specified above.
Monitoring and Transparency of Infant Feeding in Hospitals
The evaluation of maternity hospital policies and practices has been an effective tool to achieve policy, systems, and environmental change to improve breastfeeding in NYS. Each hospital is required to have written breastfeeding policies as outlined in NYS hospital regulations (NYCRR 405.21 9 ). In 2009, all NYS hospitals providing maternity services (n=139) were required to submit their written breastfeeding policies to the NYS Department of Health for review. None of the hospital policies included all of the required components (Fig. 2). On average, the hospital policies included only 59% (19 of the 32 required components). Further analysis evaluated the nine key evidence-based components of the hospital breastfeeding policies that are most supportive of exclusive breastfeeding. The percentages of hospitals whose breastfeeding policy included each of the key components are illustrated in Figure 3. Each hospital was provided with an individual evaluation of their hospital's policies with suggested revisions. Revised hospital policies will be collected again and evaluated in 2011.

Review of breastfeeding policies from NYS hospitals in 2009 (n=139).
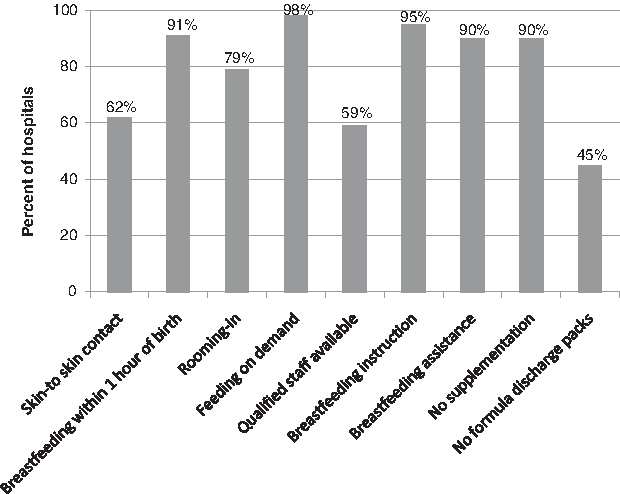
Review of inclusion of key components in NYS hospital policies (n=139).
NYS Department of Health has also surveyed hospitals to assess maternity care and infant feeding practices. Initial surveys were completed in 1998 and 2002. An expanded survey was developed and sent into the field in 2009 and is scheduled to be repeated in 2011 and 2013. These surveys are intended to provide process measures on hospital practices and to raise hospital awareness about the public health importance of breastfeeding, especially exclusive breastfeeding during the hospital stay.
Measuring the impact of systems change at the hospital level necessitates a comprehensive system utilizing breastfeeding performance indicators, such as the infant feeding data from the electronic birth certificate. To improve the quality and reporting of these data, standardized definitions for these indicators were established in conjunction with the National Center for Health Statistics, the Joint Commission on Accreditation of Healthcare Organizations, New York City Vital Statistics, and Bureau of Biometrics and Health Statistics, NYS Department of Health. The electronic birth certificate in NYS and New York City specifies four infant feeding categories: Formula only; breastmilk only; both formula and breastmilk; or other. Public health law mandates NYS hospitals must submit birth certificate data at discharge or day 5 of life for infants not yet discharged. Under NYS Public Health Law, Article 28, §2803–j, 14 three breastfeeding performance indicators—(1) fed any breastmilk (initiation), (2) exclusive breastmilk feeding, and (3) formula supplementation of breastfed infants—are publicly reported for each hospital in the Maternity Information Brochure and on the NYS Department of Health public website (hospitals.nyhealth.gov/). These measures are calculated for all healthy infants (defined as liveborn infants, excluding infants admitted to a neonatal intensive care unit and/or transferred in/out of the hospital) and are updated annually.
Implementation of Evidence-Based Best Practices
In hospitals
Three key areas were the focus of state efforts to support improved hospital breastfeeding performance: Policy training for hospital administrators, on-line training for hospital nursing staff, and a hospital-based quality improvement learning collaborative. The gold standard for hospital-based maternity and infant feeding care is the World Health Organization/UNICEF's Ten Steps to Successful Breastfeeding 10 (Table 1). These steps are strongly linked to breastfeeding exclusivity and duration 12 and are the evidence-based best practices that should guide maternity care decisions to achieve optimal outcomes for mothers and newborns. Many of the hospital practices that mothers and newborns experience throughout their hospital stay affect how likely they are to establish breastfeeding. Mothers experiencing none of the Ten Steps are eight times more likely to stop breastfeeding before 6 weeks than those experiencing five steps. 15 Research has shown that changes in maternity care practices effectively increased breastfeeding initiation and duration rates.16,17
The evaluation of NYS hospital breastfeeding policies (discussed previously) identified a need for improvement. To address this deficiency, NYS developed a model hospital breastfeeding policy and an implementation guide. These documents were designed to support improvement of hospital breastfeeding policies and increase utilization of evidence-based best practices (the Ten Steps to Successful Breastfeeding 10 ). They provide hospitals with potential strategies for implementation and translation of policies into practice and for making the systemic and environmental changes necessary for improvement of overall breastfeeding support. The Academy of Breastfeeding Medicine published protocols 18 that were used to guide document development for the NYS Model Hospital Breastfeeding Policy. 19 Eighty-four percent (113 of 135) of hospitals that provide maternity care (n=135 in 2011) in NYS participated in one of the nine NYS Model Hospital Breastfeeding Policy Training 20 webinars that were provided in early 2011. The NYS Model Hospital Breastfeeding Policy 19 and the NYS Model Hospital Breastfeeding Policy: Implementation Guide 21 are posted on the NYS Department of Health public website.
Increasing individual hospital maternity care staff knowledge to improve hospital breastfeeding support practices has been a priority in NYS. The Ten Steps to Successful Breastfeeding on-line course 22 was provided to more than 1,000 staff at NYS maternity care hospitals. Access codes were distributed either directly from NYS Department of Health to hospitals or through the Regional Perinatal Centers, with progress and completion monitored by the NYS Department of Health. To date 80% of activated courses have been completed. This training satisfies Step 2 of the Ten Steps (“Train all healthcare staff in skills necessary to implement this policy”) and also meets training requirements of the Baby-Friendly Hospital Initiative. 23
To expand this work beyond basic training, a targeted quality improvement collaborative was initiated with Communities Putting Prevention to Work funds from the Centers for Disease Control and Prevention. A group of the lowest performing hospitals was invited to participate in the Breastfeeding Quality Improvement in Hospitals (BQIH) learning collaborative. The work incorporates evidence-based maternity care practices (the Ten Steps to Successful Breastfeeding 10 ) and the Institute for Healthcare Improvement's Breakthrough Series improvement methodology. 24 Identified high-leverage changes are based on the steps that have the most impact on breastfeeding success. The Model for Improvement 24 (Fig. 4) combines evidence-based practices and fundamentals of improvement to create change. Fundamentals include: Knowing why improvement is needed, a feedback mechanism to determine that improvement is occurring, development of changes that will result in improvement, testing changes before implementation, and implementation of change. Essentially, this identifies what is known, what is being done, and what is needed to bridge the gap to improve healthcare practices. Finally, the Learning Model 24 (Fig. 5) engages hospital teams in monitoring their successes, sharing ideas, and gaining knowledge and skills to advance the improvement process. It also provides opportunities for the leadership team to monitor progress and guide the teams to optimize their strategies for effective change. Overall, process and outcome measures are evaluated to better understand how to achieve consistent, sustainable change in hospital systems that result in improvements in breastfeeding.
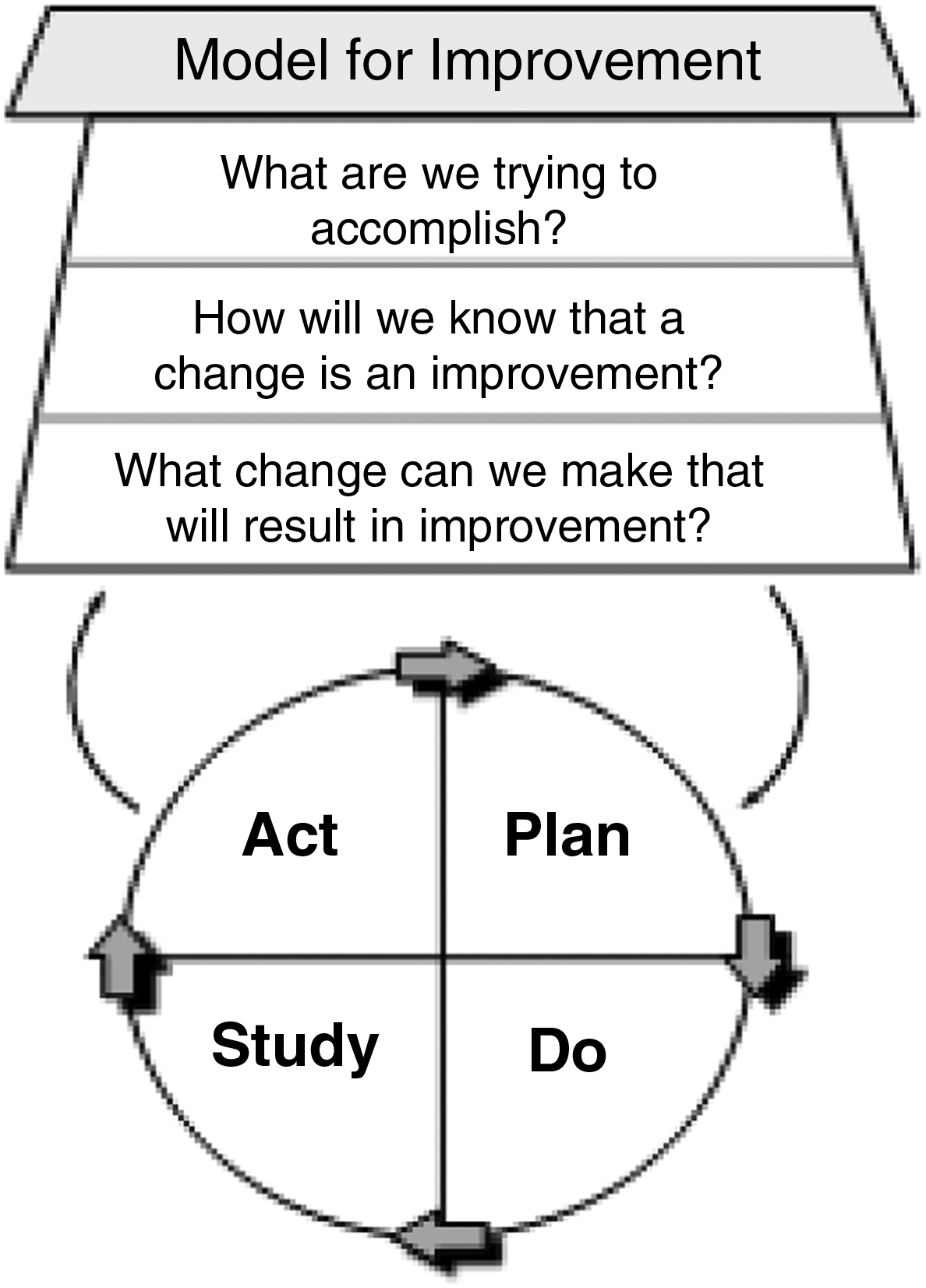
Breastfeeding Quality Improvement in Hospitals improvement model. Adapted from the Institute for Healthcare Improvement Breakthrough Series. 24

Breastfeeding Quality Improvement in Hospitals learning model. Adapted from the Institute for Healthcare Improvement Breakthrough Series. 24
During the first 10 months of the BQIH project significant changes have been seen, including increases in exclusive breastfeeding from 33% to 47%, increases in the number of infants rooming-in (>18 hours in a 24-hour period) from 31% to 54%, and a decrease in the proportion of infants/mothers who receive free formula samples and/or coupons at discharge from 58% to 29%. Ten of the 12 hospitals no longer distribute formula discharge gift bags, which may positively influence exclusivity and duration of breastfeeding for infants born at those facilities.
The BQIH collaborative, when completed, will provide the additional examples of successful strategies to implement change and improve maternity care and breastfeeding, especially exclusive breastfeeding success. These will enhance development of a toolkit and provide case studies of how hospitals overcame barriers to implement policy, systems, and environmental change. Future plans in NYS include dissemination of this toolkit to all NYS hospitals providing maternity services and engagement of additional hospitals in quality improvement work.
Prenatal and postnatal settings
The NYS Special Supplemental Nutrition Program for Women, Infants and Children (WIC) has been a pivotal partner in promotion and support of breastfeeding. In 2010, NYS WIC was recognized by the U.S. Department of Agriculture for its high breastfeeding initiation rate: 74.4% in NYS WIC compared with 62% for all U.S. WIC participants. The U.S. Department of Agriculture awarded the program $1.6 million, which has been used to fund a media campaign and a healthcare provider detailing project. The media campaign included television, internet, and bus shelter advertisements. The balance of the grant was used to design and distribute a toolkit entitled “Partnering with WIC for Breastfeeding Success.” 25 The toolkit is used to educate healthcare providers on how best to support breastfeeding mothers. These are delivered to local obstetric, pediatric, and family practice provider offices in person by WIC staff. Included in the package for providers are an educational DVD, a clinician's pocket guide, website cards, and posters. A leaflet summarizing the NYS laws that support and protect a woman's decision to breastfeed are provided (and can be ordered) for distribution to pregnant women and new mothers. Also featured is specific guidance for achieving a breastfeeding friendly practice.
NYS WIC is continuing promotion and support of breastfeeding through development of a Return to Work Toolkit (currently unpublished) to support participants in making arrangements to continue breastfeeding after returning to work. The development of this toolkit is based on formative research, including listening sessions of breastfeeding mothers at WIC agencies. NYS WIC staff will be trained on using this toolkit, which will be available in the fall of 2011 (breastfeedingpartners.org/).
The Return to Work Toolkit builds on previous work utilizing the Business Case for Breastfeeding. This program provides guidelines to help employers provide worksite lactation support to their breastfeeding employees while highlighting the benefits to both business and mother. In 2009, the NYS Department of Health provided 1-day training seminars on the Business Case for Breastfeeding 26 at venues across NYS. More than 400 professionals were trained. An evaluation of the impact of these training sessions, through measurement of success and failure during implementation at worksites, is ongoing.
Discussion and Conclusions
Breastfeeding has been a priority in NYS for more than 25 years. Current efforts are aligned with the recognition that optimal health benefits for infants and mothers are provided by exclusive breastfeeding for the first 6 months of life. This recommendation is consistent with the HP2020 3 goals and the Joint Commission on Accreditation of Healthcare Organizations' hospital perinatal standards. The overall goal in NYS is to make exclusive breastfeeding the norm by ensuring optimal support is available for breastfeeding mothers from their spouse/partner, family, healthcare providers, hospitals, worksites, daycare facilities, and communities.
The NYS Department of Health has developed a 5-year plan to expand the successful BQIH Initiative to include all hospitals providing maternity services in NYS. To achieve this overall goal, we have the following aims: Increasing compliance with NYS legislation and hospital regulations, improving the quality and validity of reported breastfeeding data, and improving implementation of evidence-based best practices in maternity care and infant nutrition. The results of these efforts are expected to increase breastfeeding initiation and exclusivity, reduce variation in breastfeeding outcomes across hospitals, and reduce disparities by race/ethnicity, maternal educational attainment, and income in population breastfeeding rates. An increase in the number of Baby-Friendly hospitals in NYS will also support the institutionalization of these efforts.
Next steps are to reduce identified barriers to exclusive breastfeeding for 6 months. Potential strategies include: Increasing the availability and insurance coverage (Medicaid, health exchanges, private) of breastfeeding education and lactation counseling by recognized practitioners (International Board Certified Lactation Consultants and Certified Lactation Consultants) prenatally, perinatally, and postnatally; increasing the percentage of newborns delivered in Baby-Friendly hospitals; and making it easier for working women who must return to work to nurse/pump in the worksite (supported by state legislation, Nursing Mothers in the Workplace Act, 8 and federal legislation). Additional strategies at the federal level include modifying The Family and Medical Leave Act 27 to allow eligible employees to take 6 months, rather than just 12 weeks, of unpaid, job-protected leave. These changes will reduce disparities in breastfeeding outcomes and move NYS towards the HP2020 3 exclusive breastfeeding goals.
NYS has started to build a statewide system that supports and monitors breastfeeding across multiple sectors of health care and business to ensure ongoing promotion, support, and protection of breastfeeding. NYS's successes to date are the result of many, including breastfeeding advocates, medical and other professional groups, individual healthcare providers, lactation consultants, mothers and their families, and state and local health departments and governments. To be fully successful in changing the social norm, however, continued efforts by the partners and stakeholders are needed to make NYS the most breastfeeding friendly state.
Footnotes
Acknowledgments
This work was supported in part by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, American Recovery and Reinvestment Act of 2009, Communities Putting Prevention to Work State Supplemental Funding for Healthy Communities, Tobacco Control, Diabetes Prevention and Control, and Behavioral Risk Factor Surveillance System DP09-901/3U58DP001963-01S2, Cooperative Agreement 5U58/DP001414-03 from the Centers for Disease Control and Prevention, and the New York State Department of Health.
Disclosure Statement
No competing financial interests exist.