
Abstract

Every human being is the author of his own health or disease … 1
As with any initiative, a cost is involved, and someone has to pay. In terms of health care, who are the payers? The list includes:
• Individuals • Hospitals and clinics • Other organizations • Insurance providers • Government organizations
Depending upon how you look at this list, top down or bottom up, the cost of services is generally a mix. Take, for example, providing breastmilk for a baby in the NICU. To breastfeed an infant in the NICU, a mother needs a hospital-grade (preferably) breast pump and milk collection and storage supplies to initiate and maintain her milk production during the hospitalization and possibly after discharge. Recently, a cost analysis was conducted to determine the value of 100 mL of expressed mother's own milk for an infant in the NICU. 5 A range of $2.60–$6.18 per 100 mL of milk was calculated based on the cost of breastfeeding equipment and loss of maternal wages. For very low birth weight (VLBW) infants, additional nutrients (fortifiers) are required to be added to mother's milk to promote growth. When a mother's own milk is not available, pasteurized donor human milk is recommended for feedings in order to avoid exposure of the infant's vulnerable intestine to commercial formula. A recent study found that after controlling for confounding factors, VLBW infants who were fed human milk exclusively (mother's own milk and/or donor milk plus human milk-based fortifier) had a 77% reduction in the odds of developing necrotizing enterocolitis (NEC) compared with infants who were exposed to any preterm formula. 6 There is a cost associated with donor milk and human milk-based fortifier; however, there is no universal standard on who pays. A cost analysis 7 based on discharge data from over 257 California hospitals found that VLBW infants with medical NEC had a length of stay extended by 11.7 days and additional costs of U.S. $74,004 compared with VLBW infants without NEC. The results for surgical NEC were even more compelling, with an added 43.1 days to length of stay and incurred additional costs of U.S. $198,040. These analyses may assist individual hospitals to justify the cost of providing donor milk and human milk-based fortifier to promote better outcomes for this patient population. Currently at our hospital, donor milk is covered by Texas Medicaid and other third-party payers. Additionally, most third-party payers are covering for the human milk-based fortifier. In Texas, as in some other states, breast pumps are provided free of charge to mothers who are eligible for the Women, Infants, and Children supplemental nutrition program if their infants are in the NICU. Some third-party payers cover the pump rental fees, although coverage is inconsistent. For the rest, the mother must bear the cost. Some hospitals absorb the cost of milk storage bottles, roll the cost into the bed charge, or pass on the cost to the individual patient in the form of a hospital charge.
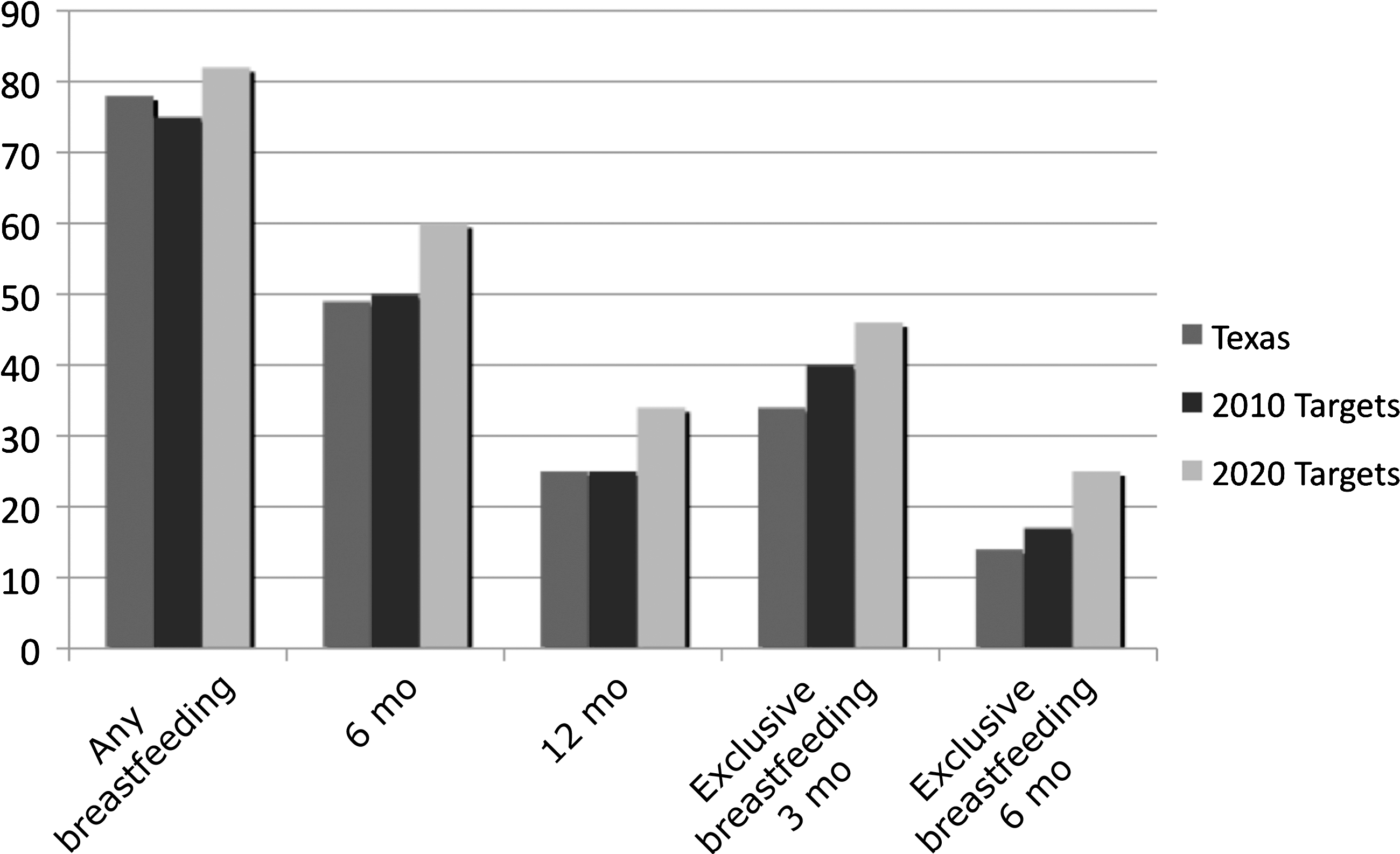
Beyond the NICU, breastfeeding initiatives have taken on various forms. Government reports, such as the 2020 Healthy Goals 8 and the Surgeon General's Call to Action, 1 provide a blueprint to increase breastfeeding in the United States. These reports allow individual states to track where they fall based on past and future goals (Fig. 1). Other actions like the recent reversal of the Internal Revenue Service to allow the deduction of breastfeeding supplies on 2010 taxes provides an incentive to breastfeed. The Patient Protection and Affordable Care Act section 4207 11 requires an employer to provide reasonable break time for an employee to express her milk for her nursing infant for 1 year after birth. At our hospital this has been done for several years. Employees can use the pumping facilities, including hospital-grade breast pumps, in the Lactation Support Services area adjacent to the NICU. There are several additional pumping rooms throughout the hospital and in other buildings on campus. In the soon to be completed Pavilion for Women, there is a pumping room for employees on every floor. Several large companies and institutions have created other such services, mostly driven by employees who saw a need and influenced change.
At the state level, legislation has made significant strides forward in the promotion of breastfeeding:
• 44 states have laws that allow women to breastfeed in any public or private location. • 28 states exempt breastfeeding from public indecency laws. • 24 states have laws related to breastfeeding in the workplace.
The verbiage in these laws illustrates the change in the culture. For example, Virginia allows women to breastfeed on any land or property owned by the state. Puerto Rico requires shopping malls, airports, public service government centers, and other select locations to have accessible areas designed for breastfeeding that are not bathrooms. Louisiana prohibits any child care facility from discriminating against breastfed babies. Mississippi requires specific guidelines for licensed child care facilities related to breastfeeding and proper handling of expressed breast milk. California requires the Department of Public Health to develop a training course of hospital policies and recommendations that promote exclusive breastfeeding and to specify staff for whom this model training is appropriate. Maryland exempts the sale of tangible personal property that is manufactured for the purpose of initiating, supporting, or sustaining breastfeeding from the sales and use tax. California, New York, and Texas have laws related to the procurement, processing, distribution, or use of human milk. New York created a Breastfeeding Mothers' Bill of Rights, 12 which is required to be posted in maternal healthcare facilities.
All of these changes were driven by individuals who recognized a need in their communities. Enlisting help from organizations with a vested interest in breastfeeding promotion (i.e., La Leche League, state and local breastfeeding coalitions), individuals and groups can impact the support mothers receive related to breastfeeding. In Texas, we are very fortunate to have a very active State Department of Health and Human Services in promoting breastfeeding education. Services provided include staff education, peer counseling programs, and local breastfeeding clinics, such as the Lactation Foundation in Houston. The Baby Café concept is another grassroots initiative that originated in the United Kingdom and has spread worldwide. With four locations in Texas, these centers offer free support for breastfeeding mothers on a drop-in basis.
In conclusion, there is much that can be accomplished to improve breastfeeding rates for healthy and hospitalized infants. In the climate of healthcare reform, important decisions will need to be made to determine the most cost-effective way to achieve the best possible outcomes for mothers and their infants. Individuals, hospitals, private businesses, organizations, and all levels of government will play a role in the promotion, support, and cost of breastfeeding if we are to reach the U.S. 2020 goals.
Footnotes
Disclosure Statement
No competing financial interests exist.