
Abstract

Since 2006, NYCDOHMH has worked to increase breastfeeding exclusivity and duration in 19 public and private hospitals by helping them implement system-wide policies and practices, educate and train staff, and collect standardized data on infant feeding practices. Using evidence-based practices based on the World Health Organization/UNICEF Ten Steps 1 and the Baby-Friendly USA model, Harlem Hospital Center was designated as the first Baby-Friendly Hospital in New York City in 2008, and New York University/Tisch Hospital became the second maternity hospital to achieve designation in 2011. Six hospitals are officially on the pathway toward Baby-Friendly designation, and others have expressed a heightened interest in pursuing designation.
In March 2010, NYCDOHMH received the CPPW obesity grant, funded by the Centers for Disease Control and Prevention. This funding has allowed NYCDOHMH to continue to work with hospitals to improve policies and procedures on the inpatient units. Additionally, because hospital services are often fragmented, the grant has allowed us to increase breastfeeding support to pregnant and parenting women by linking prenatal education providers in clinics, Women, Infants, and Children peer support counselors, and home visiting.
In October 2010, we received a CPPW supplemental grant (mentoring grant) to contribute to the development of a nationwide learning community by expanding on the collaborative partnership model for community health improvement to provide peer-to-peer mentoring, staff training, and technical assistance to 10 CPPW-funded LHDs around the country.2,3 The LHDs were selected to receive mentoring assistance based on their commitment to improve hospital breastfeeding rates in their communities 4 (Table 1). A needs assessment survey was conducted with each LHD to understand the scope of their current breastfeeding promotion activities and their population and demographics and to identify areas that could be improved by technical assistance support. Mentoring activities include the development of a community-specific work plan, which is updated during monthly teleconferences with each health department; two webinars, which are designed to build capacity; distribution of NYCDOHMH materials and/or the development of new web-based materials and tools; and information sharing via a confidential listserv. The mentoring grant also provided funding for Baby-Friendly USA to give on-site technical assistance to up to 50 hospitals within the jurisdictions of the LHDs and for Healthy Children's Center for Breastfeeding to provide five 40-hour lactation education courses to support hospital staff training needs (Fig. 1).
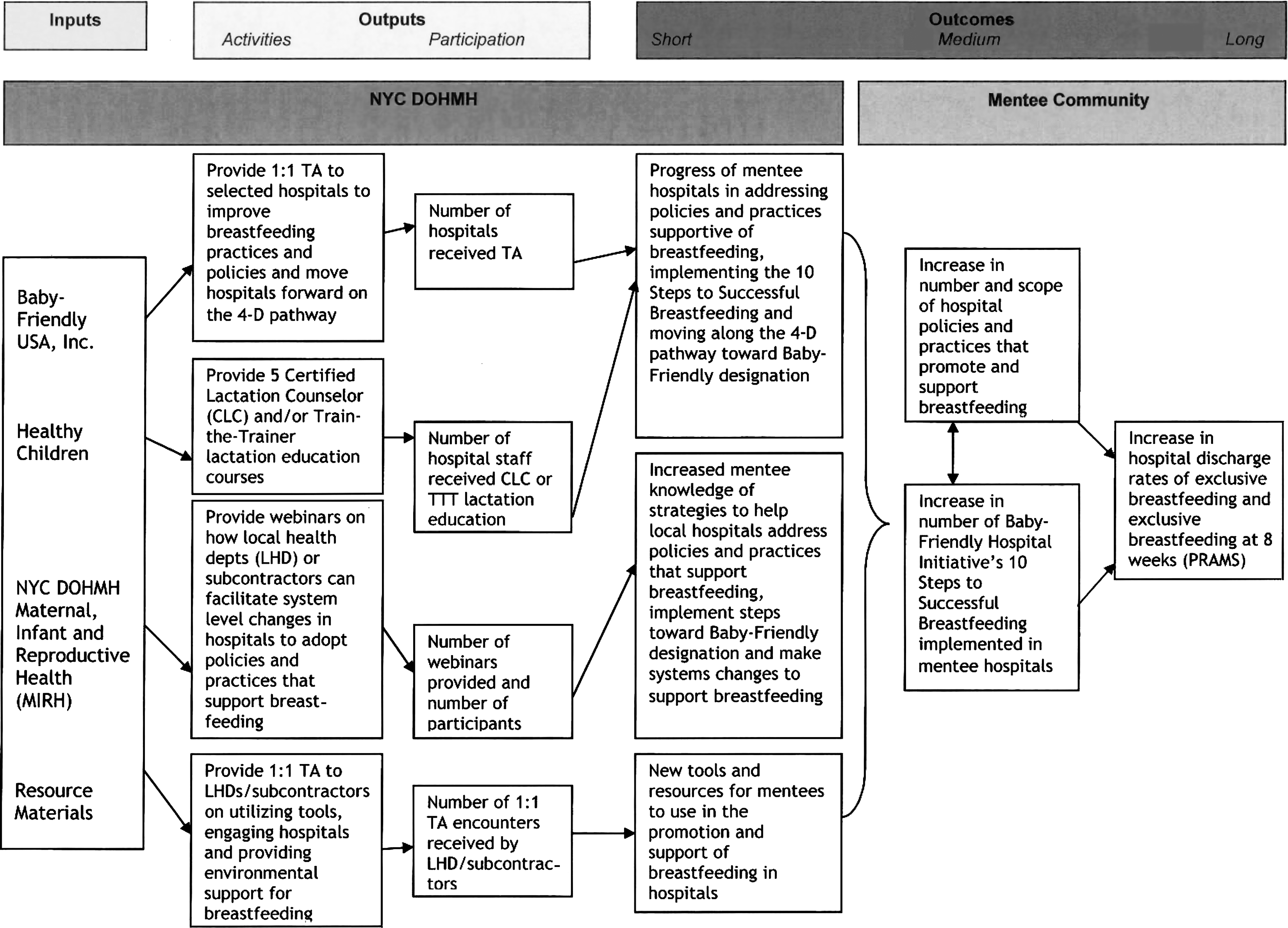
Logic model describing activities and outcomes of the Communities Putting Prevention to Work breastfeeding mentoring grant. LHD, local health department; NYC DOHMH, New York City Department of Health and Mental Hygiene; PRAMS, Pregnancy Risk Assessment Monitoring System; TA, technical assistance; TTT, Train-the-Trainer.
Data are from the Centers for Disease Control and Prevention. 4
Statistics available only for the state where noted.
Progress of mentoring activities will be evaluated by DOHMH using process measures such as mentee participation in conferences and webinars, website hits, and documentation of phone encounters as well as gains in knowledge on established learning objectives as a consequence of conferences and webinars. Particular attention will be paid to the progress made in implementing the 10 Baby-Friendly steps. NYCDOHMH will gather qualitative feedback from mentees to ascertain the impact of mentoring activities in improving policies and practices in the hospitals and increasing the breastfeeding rates and duration in their communities.
Common Issues Across Communities
Despite their diversity, we were struck by how many LHDs report similar successes and challenges. We identified five common areas of concern for which the majority of LHDs requested technical assistance.
Engaging hospitals
The LHDs have different historical interactions and relationships with the individual hospitals in their communities, and many had not worked on breastfeeding promotion in the past. Technical assistance requests focused on defining the LHD's role in changing hospital systems, how to approach and establish relationships with hospital staff, and how to support internal hospital champions once they are identified.
We suggested methods they could use to establish hospital contacts, including creating a spreadsheet of current hospital staff and contact information. We advised on how to assist hospitals with convening a multidisciplinary committee composed of essential hospital staff and external partners, provided information on how to engage internal champions in order to build momentum, and facilitated discussion of how to develop a buy-in strategy for hospitals to excite them about breastfeeding promotion.
Convening hospitals
Because most of the LHDs had several hospitals in their jurisdiction that had never worked collaboratively in the past, they requested assistance on how to organize and convene hospitals to partner with them on breastfeeding promotion. This was an issue in New York City as well, where we thought it was important to build momentum to engage all 40 maternity hospitals across the five boroughs, not just those participating in the grant. We addressed this problem locally by holding a half-day conference, “Getting from Here to There: Helping NYC Hospitals Go Baby-Friendly,” at the NYCDOHMH. Representatives from 95% of the maternity hospitals attended. The conference featured opening remarks by the Commissioner of Health, Dr. Thomas Farley, a keynote presentation from Trish MacEnroe, the Executive Director of Baby-Friendly USA, and an interactive panel presentation from six local hospitals on best practices. We have started a hospital listserv, which further extends the hospitals' ability to share information and benefit from other New York City programs. For interested LHDs, we provided our conference materials and final report as well as assistance to those planning their own conferences.
Supporting staff training
Staff training is an evidence-based component 5 to improve breastfeeding exclusivity and duration in hospitals, and several LHDs wanted to help hospitals train their clinical staff on lactation management and education. Some suggestions included creating a resource list of local experts in breastfeeding (either within their own agencies or in the community); sponsoring Grand Rounds presentations for clinical staff; developing and printing educational materials for providers; hosting or sponsoring 20-hour lactation education courses for nursing staff, which can be done online or by in-person 40-hour Certified Lactation Counseling courses; and developing a resource guide of no/low-cost training courses available online for physicians.
Reaching out to community partners
Breastfeeding support for new mothers goes beyond the hospital stay. However, most hospitals were unaware of the scope of breastfeeding resources that are available in their communities. We emphasized to each LHD that their view of the community was unique and that they were well positioned to collect information on existing breastfeeding resources. As an interested, but objective entity, LHDs are also well situated to create nonpartisan materials that could be distributed to all hospitals and consumers. We presented the example of the New York City Breastfeeding Resource Guide listing all hospitals, Women, Infants, and Children sites, childbirth education classes, and other resources. The Guide was professionally developed, printed, and distributed to all hospitals and is available on the NYCDOHMH website. We also provided LHDs with the breastfeeding educational resources and tools that NYCDOHMH has developed over the years, including pocket guides for pediatricians, obstetrician/gynecologists, and family physicians, as well as posters and crib cards, all available in six languages.
Data collection and evaluation
Data are a fundamental part of changing hospital-based breastfeeding practices and policy because without accurate data it is impossible to track accomplishments and areas of continued need. Several LHDs were interested in supporting hospitals with data collection and evaluation. Specifically, there was interest in knowing how LHDs can track and evaluate the progress of their programs and how LHDs can use and share data as an advocacy tool.
We emphasized that LHDs need to determine their best role in helping hospitals collect and analyze their data. We shared our data collection tools, including a codebook of variables and summary reporting documents. We suggested ways in which the LHD can play a role by helping to strengthen and improve systems, by providing in-kind or paid staff to support the data collection, extraction, and evaluation process. LHDs may also be able to provide assistance to hospitals in their communities by creating templates for data collection, tracking, and reporting, as well as consulting on how to use data, set benchmarks, and increase compliance with documentation standards. The LHD can also draw local attention to national models and reports for how to utilize data as a tool for advocacy.
Conclusions
LHDs are uniquely positioned to support hospitals in improving their breastfeeding policies and practices using a collaborative model. LHDs are not in competition with hospitals and therefore have the ability to work across hospital systems to increase the number of facilities promoting breastfeeding. Hospitals in New York City were initially reluctant to partner with the NYCDOHMH; however, as a local agency without regulatory responsibility for hospitals, we have been able to provide an impartial perspective as well as maintain confidentiality.
The mentoring grant has allowed NYCDOHMH a unique opportunity to look at how LHDs in communities across the country are engaging hospitals to improve breastfeeding initiation, duration, and exclusivity. In developing the collaborative mentoring model, we have been able to promote dialogue, best practices, and technical assistance. This methodology can be readily adapted to the needs of cities/counties with the goal of building momentum in establishing and maintaining breastfeeding exclusivity and duration in the United States.
Footnotes
Acknowledgments
This article was supported by Cooperative Agreement Number 3U58DP002419-01S1 from the Centers for Disease Control and Prevention, Communities Putting Prevention to Work. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention. The authors thank Judith Sackoff, Ph.D., and Sarah B. Perl, M.P.H., for their valuable assistance.
Disclosure Statement
No competing financial interests exist.