
Abstract
Abstract
Background:
The effect of epidural analgesia on labor and effective breastfeeding is still being debated. The aim of this study is to define its impact on the trend of labor, the newborns' well-being, and early breastfeeding.
Methods:
We considered first-term physiologic pregnant women who delivered by the vaginal route. We divided them into two groups: Group A received epidural analgesia during labor, whereas Group B received no analgesia. We recorded maternal age, gestational age, modality of delivery, length of labor, and length of active labor. All newborns received skin-to-skin contact; early breastfeeding was encouraged. We recorded data on birth weight and length, Apgar score at minutes 1 and 5, type of crying, neonatal reactivity, and time between birth and exposure to the breast. Statistical significance was considered for p<0.05.
Results:
Of 934 pregnant women who delivered by the vaginal route, 317 patients required labor analgesia, and 245 patients agreed to participate in our study. Only 128 patients met inclusion criteria. We randomized them in 64 women in Group A and 64 women in Group B. Data on maternal age, gestational age, type of delivery, neonatal birth weight and length, and Apgar score showed no significant differences. Total length of labor was 363.58±62.20 minutes in Group A versus 292.30±64.75 minutes in Group B (p<0.001). The length of active labor showed no significant difference. Among neonatal parameters we found a statistically significant difference only for length of first breastfeeding, with a mean duration of <30 minutes in 62.2% in Group A versus 29.3% in Group B (p<0.001).
Conclusions:
Epidural analgesia has little effect on trend of labor and duration of first breastfeed and none on neonatal outcome. A new protocol of epidural analgesia may solve these side effects.
Introduction
Nevertheless, the impact of labor analgesia on the progress of labor, on the mode of delivery, and on the initiation of an effective and early breastfeeding is still being debated. Observational studies conclude that parturients who received labor analgesia for labor have higher cesarean section and instrumental vaginal delivery rates and longer durations of labor, without a clear cause–effect relationship. 2 In spite this, Halpern et al. 5 and a Cochrane review 3 on analgesia in labor asserted that epidural analgesia has no statistically significant impact on the risk of cesarean section, maternal satisfaction with pain relief, and long-term backache and does not appear to have an immediate effect on neonatal status as determined by Apgar scores. Another key point in the use of labor analgesia regards its effect on breastfeeding. Today mothers have an increased wish to have skin-to-skin contact with the baby and to breastfeed earlier as possible, so there is increasing attention on promoting this need. Breastfeeding has significant benefits for the newborns (i.e., protection from infectious diseases, improved cognitive development, and benefits related to maternal–infant bonding). 6 Human milk may also protect against sudden infant death syndrome, diabetes, lymphoma, allergies, and chronic digestive diseases. Lactation decreases the risk of postpartum bleeding, speeds the return to prepregnancy weight, improves bone remineralization, and reduces risks of ovarian and breast cancer.6,7 Nevertheless, there seems to be a link between breastfeeding and a greater response to infant cues in brain regions implicated in maternal–infant bonding and empathy during the early postpartum. Such brain activations may facilitate greater maternal sensitivity as infants enter their social world. 8 One of the first study on impact of labor analgesia and the delay in the initiation of breastfeeding in healthy neonates in the early neonatal period was published in 1989 by Matthews, 9 whose findings suggested that even small doses of the narcotic analgesic alphaprodine, when administered 1–3 hours prior to delivery, could delay effective feeding by several hours and, in some cases, days. Nowadays many new techniques of pain relief in labor are available, but controversial studies were conducted to detect the effect of labor analgesia on breastfeeding duration and in particular on the delay of first breastfeeding. Wilson et al. 10 compared many different types of epidural analgesia techniques in a randomized controlled trial, refuting the hypothesis that epidural analgesia per se has an effect on breastfeeding initiation. Even in other studies, no difference in breastfeeding was seen when mothers with or without epidural analgesia were compared.11–14 In particular, Jordan et al. 12 asserted that where women had intended to bottle-feed, intrapartum analgesia made no difference; where women had undergone a cesarean section, this was a more powerful determinant of infant feeding than the type of analgesia. However, all the data are from small samples, and the conclusions are not able to assert with certainty the absolute absence of effect of epidural analgesia on breastfeeding. Moreover, other studies showed an association but not a cause–effect link between epidural analgesia and reduced breastfeeding success.5,15,16
The aim of our study was to define the impact of epidural analgesia during labor on the trend of the labor, on neonatal well-being at birth, and, in particular, on the early establishment of an effective breastfeeding.
Subjects and Methods
Mothers and all term newborns admitted to the regular nursery of the Department of Gynaecological and Obstetric Clinic in the School of Medicine, University of Padua, Padua, Italy, a Level III hospital with full resources for obstetric and complete neonatal intensive care, from January 2008 and June 2008 who delivered by the vaginal route were eligible for inclusion in this study. The study was approved by the Institutional Review Board of the hospital.
Patients entered into the study sequentially and casually (i.e., gradually included in the sample and subsequently checked for exclusion criteria and only if they agreed to the study after adequate information and after giving their informed consent, in accordance with the Italian privacy law [Italian Law 675/96]). Outcome variables, methods of analysis, and inclusion and exclusion criteria were determined prospectively. As inclusion criteria we considered women with first physiologic pregnancies between 38 and 42 gestational weeks who underwent a spontaneous or induced labor and who had infants with neonatal birth weight between 2,500 and 4,300 g and an Apgar score of more than 7 at the first minute and 8 at the fifth minute.
We divided our sample into two groups. We called Group A our Study Group, constituted by patients who received analgesia during labor (3–4 cm of cervical dilatation and regular contractions on frequency, intensity, and duration) through a catheter placed at the lumbar spine (L2–L3, L3–L4) after maternal request and after an informed consent for anesthetic–analgesic procedures. As indicated by the Guidelines of the Italian Committee for Obstetric Anaesthesia, epidural analgesia was performed by administering an initial bolus of 100 μg of fentanyl diluted to 10 mL of saline solution and subsequently by booster boluses of 15–20 mL of ropivacaine (0.1%). Booster boluses were given on the basis of subjective evaluation of pain (expressed by a Verbal Numerical Scale) as a result of a subjective score of ≤4. The booster boluses were administered by the top-up technique. Upon reaching fully dilatation, the mother did not receive any additional dose. The Group B was our Control Group, consisting of patients who did not receive any form of analgesia during labor, whether spontaneous or induced, according to their own choice.
For all patients we recorded maternal age, gestational age (in weeks), modality of delivery (spontaneous, induced by intracervical application of prostaglandin, or piloted by oxytocin administration), length of the labor (in minutes), and length of active labor (i.e., second stage of labor [in minutes]).
At birth, newborns of both groups were put on the mother's abdomen for skin-to-skin contact, and as soon as the baby expressed the first sign of rooting for the maternal breast, he or she was encouraged to suck. Within the first 2 hours of birth, the midwives completed a grid-structured follow-up for each infant (Table 1), collecting data on birth weight and birth length, Apgar score at first and fifth minutes, type of crying (defined as weak or strong based on respiration, as an Apgar score parameter), neonatal reactivity (defined as weak reactivity [pathological] or energetic [physiological] according to the evaluation of the parameters of tone and reflexes as an Apgar score), elapsed time between birth and the possible breast exposure (i.e., the newborn searches and reaches for the breast, considering as physiological a waiting time of 30 minutes as recommended by World Health Organization/UNICEF guidelines 17 ), and evaluation of the first breastfeeding in terms of correct or incorrect sucking, according to the World Health Organization/UNICEF criteria 17 (wide open mouth, lower lip down, vigorous sucking, tongue under the areola, swollen cheeks). We measured the length of the first breastfeeding (in minutes), until the baby spontaneously peeled off.
NS, not significant (p>0.05).
Statistical analysis was performed by SPSS (Chicago, IL) software for Windows version 18, using parametric and non-parametric tests where appropriate. We performed the Kolmogorov–Smirnov to test normality of distribution. Continuous data have been tested with the t test, and categorical variables have been tested with the χ2 test or Fisher's exact test where appropriate. Statistical significance was defined as p<0.05.
Results
Between January 2008 and June 2008 934 pregnant women who delivered by the vaginal route arrived to our operative unit. Neuroaxial analgesia during labor was required and received by 317 patients (36%), and among them 245 patients (77%) agreed our study. On the basis of our inclusion criteria, only 64 patients were eligible for the study (Group A). We randomly selected a sample of 64 women among the pregnant women who agreed the study, met the inclusion criteria, and had not received analgesia during labor to constitute our control group (Group B).
The statistical analysis of data about maternal age, gestational age, birth weight, neonatal length at birth, and Apgar score at the first and fifth minutes did not show significant differences between the study and control groups (p>0.05) (Table 1 and Fig. 1).
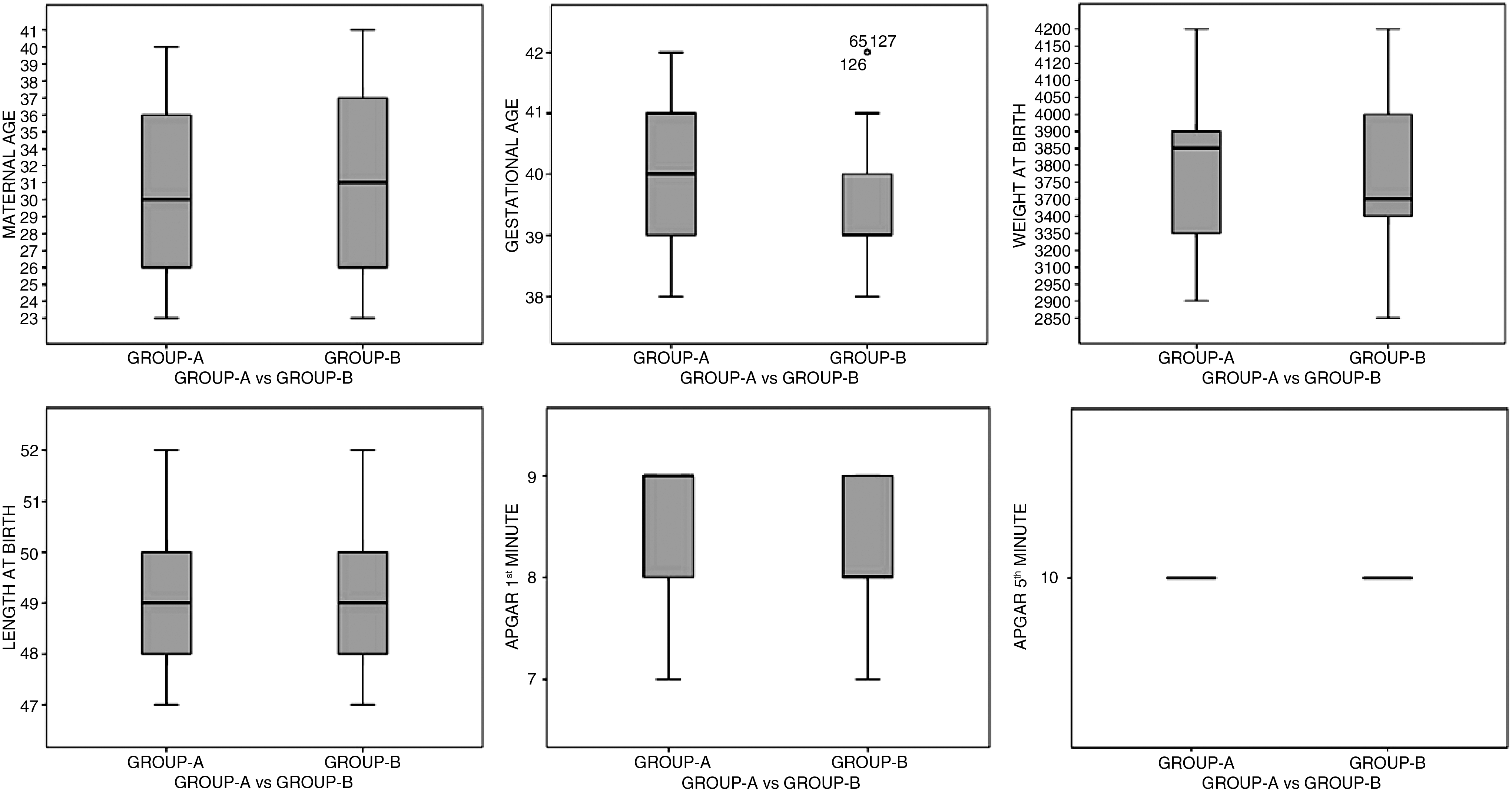
Comparison of general maternal–fetal features between Group A and Group B.
From the comparison of data about the type of delivery in the two groups, we recorded spontaneous labor in 39 patients (61%) in Group A versus 36 patients (56%) in Group B, piloted labor in nine patients (14%) versus nine patients (14%), and induced labor in 16 patients (25%) versus 19 patients (30%) (p>0.05) (Fig. 2).

Comparison of labor type between Group A and Group B.
The total length of the labor was 363.58±62.20 (mean±SD) minutes in patients of Group A versus 292.30±64.75 minutes in patients of Group B (p<0.001) (Table 2 and Fig. 3).
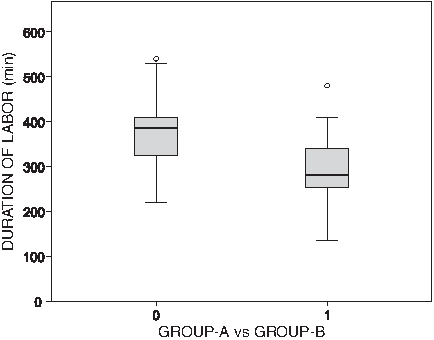
Difference in length of labor between Group A and Group B.
Statistical significance was detected only for length of labor and length for first breastfeeding.
The length of active labor was 56.23±19.11 (mean±SD) minutes in patients of Group A versus 48.34±14.17 minutes in patients of Group B (p not significant) (Table 2 and Fig. 4).
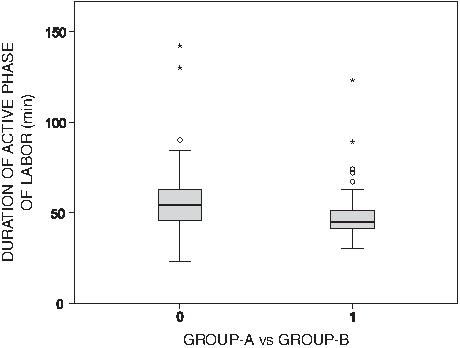
Difference in length of active labor between Group A and Group B.
The analysis of data from the observation of newborns after skin-to-skin contact with their mothers as soon as possible after birth showed that there is no statistically significant difference between Group A and Group B in terms of intensity of crying, newborn's responsiveness, elapsed time between birth and the possible exposure to the breast, and quality of the first breastfeeding (p not significant) (Table 2).
Statistical significance was shown in the comparison of the length of the first breastfeeding among newborns of Group A versus those in Group B, with a mean duration of first breastfeeding of <30 minutes in 33 of 53 (62.2%) newborns in Group A versus 17 of 58 (29.3%) newborns in Group B (p<0.001) (Table 2).
Discussion
Epidural analgesia is the most effective way of providing pain relief in labor. This technique has been progressively and widely introduced in clinical practice over the past three decades. In the United States, the percentage of parturients receiving neuraxial analgesia for labor rose to 77% in 2001 from 21% in 1981; in the United Kingdom, a little over 33% of parturients chose neuraxial analgesia for childbirth in 2008–2009. 2 Data collected during the period for our center are aligned with the percentages of analgesic epidural in labor given in industrialized European countries like the United Kingdom. In an epidemiologic study by Calderini et al. 18 in 2009, the use of neuroaxial analgesia during labor in Italian delivery rooms still appears poor in many hospitals, although in some advanced obstetric centers it reaches acceptable rates. According to our experience, the principal reasons for rejection or rather lack of maternal request may be attributed to religious, cultural, or social causes, and not least the fear of adverse effects on the fetus. Proper maternal counseling by both the mother's medical staff (obstetricians and anesthesiologists) and the midwifery staff or during childbirth preparation courses can be the most challenging step to overcome this obstacle. The fundamental step is an adequate training of the medical and midwifery staff.
The principal difficulty in performing studies on analgesia during labor is the random assignment of women to a placebo (no pain relief) group. In fact, when neuroaxial analgesia is available, it might be considered unethical as the use of an invasive technique with its correlated risks without ensuring pain relief.
Neuraxial labor analgesia has the potential to impact the course, duration, and outcome of labor. From the debate on the use of analgesia and on its effect on labor and on delivery outcome, older observational studies asserted that women who have epidural analgesia during labor are more likely to require a cesarean delivery. However, the Cochrane review 3 on analgesia in labor involving 20 trials assessed that the relative risk of cesarean delivery with epidural analgesia compared with no analgesia was 1.07 (95% confidence interval, 0.93–1.23). Initiation of neuraxial analgesia in the latent phase of labor does not increase the rate of cesarean delivery or prolong the duration of labor. Yet, effective neuraxial analgesia can prolong the second stage of labor by 15–30 minutes and, possibly, increase the necessity of instrument-assisted vaginal deliveries as well as oxytocin administration. 2 This can explain the result of a statistically significant difference of the length of the labor between the two groups in our study, perhaps in association with the small size of our sample. Our results are consistent with the literature,5,19,20 and in a recent study Frigo et al. 20 proposed a rebuilding of the labor curve during neuraxial analgesia.
In accordance with the literature,4,21,22 considering neonatal outcome, we did not record significant differences in neonatal outcome between the two groups. In recent work by Reynolds, 4 when investigating different methods of maternal pain relief in labor, regarding systemic analgesia, which could depress fetal muscular activity, aortic blood flow, short-term heart rate variability, and oxygen saturation, neuraxial analgesia seemed to be associated with better Apgar scores and variable neurobehavioral changes. Neonatal acid–base status was not only better with epidural than with systemic opioid analgesia, it was also better than with no analgesia. As also explained by Reynolds, 4 this may be due to the good effects of the neuraxial analgesia on the mother's body during labor, such as the reduction in maternal stress hormones and the better maternal ventilation frequency and uterine blood perfusion after sympathetic blockade with lower episodes of fetal desaturation because of shift in the maternal acid–base curve with better saturation of fetal hemoglobin.
Two areas of uncertainty related to epidural analgesia still remain: Its associations with maternal fever and reduced success in breastfeeding. Epidural-associated fever has been reported in randomized, controlled trials, but the mechanism is still unknown. 19 The association of epidural analgesia with reduced breastfeeding success is difficult to evaluate because of the many medical and social variables that can influence a woman's decision to start or continue breastfeeding. Nowadays there is no consensus about the unintended effects of labor epidural analgesia on breastfeeding success5,9–16,23,24 because the success of breastfeeding involves both maternal and neonatal factors.25–27
The use of labor epidural analgesia inclusive of opioids has been suspected in having a negative impact on breastfeeding success because opioids may potentially depress the neonate, preventing the establishment of a good feeding behavior in the initial hours of life. 24 Although adverse neonatal outcomes have not been reported, 3 the possibility of mild effects on the newborn is sufficient to avoid an early successful initiation of breastfeeding, leading to precocious, unplanned cessation of breastfeeding. So the mother can quit breastfeeding prematurely. Many factors, such as the mode of delivery, prior breastfeeding success, and parity, are considered potentially confounding variables in evaluating analgesia labor effect on breastfeeding.6,7,27 For this reason, in our study we excluded patients with potential confounding factors.
Our study shows a statistically significant difference only in the length of the first breastfeeding among newborns of mothers who received labor analgesia compared with those of mothers who did not. Our data agree with the results of Wieczorek et al., 23 who demonstrated that, among multiparous women who delivered vaginally after receiving epidural analgesia inclusive of fentanyl, the incidence of breastfeeding cessation at 6 weeks postpartum was much lower than previously quoted in the literature. This result maybe was linked to an environment that facilitates continued breastfeeding.
In contrast, Torvaldsen et al. 16 asserted that women who have epidurals are less likely to fully breastfeed their infant in the few days after birth and more likely to stop breastfeeding in the first 24 weeks, so although this relationship may not be causal, the authors concluded that it is important that women at higher risk of breastfeeding cessation are provided with adequate breastfeeding assistance and support. Specifically, Riordan et al. 28 pointed out that labor pain relief medications diminish early suckling but are not associated with duration of breastfeeding through 6 weeks postpartum. This confirmed the results of Crowell et al., 29 who asserted that infants who received analgesia within an hour of birth, or no analgesia, and who initiated breastfeeding early established effective feeding significantly earlier than infants with longer duration of analgesia and later initiation of breastfeeding.
Anyway, unlike our study, where we used a new although internal anesthesiological protocol with doses as low as possible, most trials demonstrating such an association do not indicate the type or dose of epidural medications used, making impossible a standardized comparison. Only Beilin et al. 24 performed a randomized, controlled trial assessing a dose–response effect of epidural fentanyl on breastfeeding success. They indicated that a dose of epidural fentanyl >150 μg is associated with a higher rate of stopped breastfeeding by 6 weeks postpartum.
One of the strengths of our study is the way of choosing of the sample studied because we selected patients from the general population arriving in our delivery room using strict inclusion criteria. Another important element seems to be the use of a unique technique of epidural analgesia during labor, standardized at our unit, and moreover performed by skilled and selected anesthesiologists, always the same. In order to establish neonatal well-being, we evaluated different parameters, focusing not only on objective ones such as Apgar score at the first and fifth minutes and umbilical arterious pH at birth, but even subjective parameters such as neonatal reactivity, type and intensity of crying, and ways of sucking, as recommended by the World Health Organization. 17 In assessing breastfeeding trend, we recorded not only the correctness of execution of first breastfed, but in particular the temporal gap between the birth and the beginning of breastfeeding and the length of the first breastfeed. Finally, our study points out that important elements useful in the management of the first contact between mother and newborn can be detected in this short but fundamental time of the mother–child relationship. Weaknesses of our study are represented by the small size of our sample, by the lack of data on the temporal duration of the first stage of labor to define effects of epidural analgesia on all the stages, the lack of data regarding the long-term follow-up on the trend of breastfeeding, and the lack of a test to detect maternal satisfaction on the use of analgesia during labor and the personal feel of the childbirth experience after an early maternal–fetal skin-to-skin contact.
Many more social, economic, and other medical factors influence the relation between epidural analgesia and delivery. We have also to consider the maternal coping style rather than a physiological effect of epidural analgesia because the level of pain tolerance in labor is subjective and might predict women's ability to cope with breastfeeding difficulties and early skin-to-skin contact with the newborn after the delivery.
Conclusions
Epidural analgesia in labor can be considered a safe procedure to remove pain during labor, with no effect on the neonatal reactivity and very low and negligible effects on the trend of the labor. So nowadays epidural analgesia is the best form of analgesia available with the least effect on the newborn. On the open points regarding the usefulness and side effects of epidural analgesia, the early cessation of breastfeeding is still of concern. At present there is no prospective, randomized evidence that epidural analgesia causes reduced breastfeeding success. Retrospective studies showed an association but not a cause–effect link between epidural analgesia and reduced breastfeeding success. Although retrospective studies conflict in their conclusions,5,15 doses of the epidural fentanyl >150 μg during labor may interfere with early breastfeeding success; consequently, boluses and high infusion concentrations of fentanyl should be avoided. 24 As the benefits of breastfeeding are now universally recognized, it is essential that appropriate assistance with early breastfeeding is provided at least until effective breastfeeding is begun. Our data highlight that a protocol of epidural analgesia able to reach the greatest coverage possible with the least influence on the trend of labor, the neonatal outcome, and the establishment of an early and effective breastfeeding may solve this concern. Further studies on epidural analgesia during labor, particularly on its relation to an impaired early breastfeeding establishment, should be undertaken.
Footnotes
Acknowledgments
The authors thank all midwives who helped in collecting the data and all anesthesiologists for their significant contributions in performing the study.
Disclosure Statement
No competing financial interests exist.