
Abstract
Abstract
Background:
Nipple pain and insufficient milk supply are major causes of early weaning. We have found that persistent nipple pain was associated with strong infant sucking vacuums during breastfeeding. Several studies indicate that nipple pain and abnormal infant sucking have the potential to reduce milk transfer. We aimed to determine whether women with persistent nipple pain had low milk supply.
Subjects and Methods:
The 24-hour milk production and feeding characteristics of mothers with persistent nipple pain (n=21) were compared with those mothers without nipple pain (n=21). Milk productions were measured by test-weighing the infant before and after every feed from each breast over a 24–26-hour period. Comparisons were made using Student's t tests and linear mixed models as appropriate.
Results:
Lower milk productions were associated with longer meal durations for mothers with pain. There were no significant differences in the average 24-hour milk production or any feeding characteristics between the groups. However, four women with persistent nipple pain had milk production levels below 500 mL/day.
Conclusions:
The majority of breastfeeding women experiencing persistent nipple pain were able to achieve normal milk production levels. Feeding duration and frequency were similar to those of women not experiencing pain. However, longer meal durations in the pain group were associated with lower levels of milk production. Further investigation is necessary to identify mothers most affected by maternal nipple pain.
Introduction
Breastfeeding is a complex physiological process, and full milk production is reliant upon adequate milk synthesis, secretion, ejection, and removal from the breast. 3 During established breastfeeding, milk synthesis rates are largely under autocrine control, in that synthesis slows as breast fullness increases. 4 Thus, ineffective milk removal will result in incomplete breast drainage and down-regulation of milk synthesis, which if prolonged may result in inadequate milk production. Newton and Newton 5 demonstrated the potential for pain to interfere with breastfeeding; they found that breastfeed volumes were significantly reduced by painful distractions. This reduction was attributed to inhibition of the milk ejection reflex, as the injection of oxytocin during the distractions increased milk transfer to normal volumes. 5 It is possible that the inhibition of milk ejection and strong sucking vacuums may have contributed to the lower feed volumes previously observed. 2
Because milk transfer may be lower in mothers with pain, it is important to determine whether or not milk production is consequently compromised. There is a large variation in milk transfer between breastfeeds both within and between mother–infant pairs, and the average volume of milk transferred during one breastfeed is inversely related to the number of breastfeeds over a 24-hour period. 6 Therefore, to accurately estimate milk production it is imperative to measure milk transfer over a 24-hour period to take into account the variations in feed volume and frequency.
This study aimed to investigate whether or not mothers with persistent nipple pain had reduced 24-hour milk production levels or altered feeding characteristics compared with mothers without pain.
Subjects and Methods
Participants
All mothers were recruited from an ongoing study investigating infant sucking dynamics during breastfeeding. Upon recruitment, mothers were invited to measure their milk production levels at home. Nine of the 30 mothers in the control group and 12 of the 30 mothers with persistent pain agreed to measure milk production. 2 An additional 12 control and nine pain mothers were recruited for this study.
The pain group consisted of mothers of healthy term infants who were experiencing persistent nipple pain during breastfeeding that had not resolved after assessment and counseling by a lactation consultant (n=21). Mothers were excluded from the study if a known clinical diagnosis for the cause of their pain had been made, including either bacterial or fungal nipple infection, nipple vasospasm, dermatitis, ankyloglossia, or torticollis. Women prescribed and taking either steroids and/or antibiotics were excluded from the study. The control group consisted of mothers breastfeeding healthy term infants, who were content with their breastfeeding relationship and not experiencing any pain during feeding (n=21).
Ethics approval for the study was granted by the Human Research Ethics Committee of The University of Western Australia, and all participants supplied written, informed consent to participate in the study.
Participant characteristics
Participant demographic and pain characteristics were collected via a questionnaire. Variables recorded included infant birth weight and gestational age, maternal age, pregnancy and postpartum complications, nipple pain, nipple shield use, and frequency of feeding expressed breastmilk and artificial formula. Maternal pain intensity was assessed immediately after the monitored breastfeed of the breast with the worst pain using the Visual Analogue Scale. 7 The duration of pain was calculated by subtracting the reported day that pain was initially experienced from the infant's age.
Measurement of milk production
Each mother measured the volume of each feed from each breast over a 24–26-hour period using the infant-test weight method.
8
Mothers recorded the start and finish time
Feeds were defined as a breastfeed from one breast. Feed durations were calculated by subtracting the reported start time from the reported end time. If a second feed started within 30 minutes of the previous feed ending, then the two feeds were classed as paired. If a third feed started within 30 minutes of the second feed ending, the three feeds were classed as clustered. A meal was defined either as an unpaired breastfeed, two paired breastfeeds, or three clustered feeds. 6 Meal durations were calculated by summing the duration of all contributing feeds, excluding between-feed intervals.
Measurement of sucking vacuum
Intra-oral vacuum was measured for an entire breastfeed via a small Silastic™ (Dow Corning) tube attached to a pressure transducer (Cobe Laboratories, Frenchs Forest, Australia) taped alongside the nipple as previously described.2,9 The pressure transducer was then connected via an interconnect cable (Cobe Laboratories) to the bridge amp (ADInstruments, Castle Hill, Australia) that was connected to a Power Lab (ADInstruments), and data were analyzed using the software package Chart version 5.0.2 (ADInstruments). Average baseline and peak vacuums for the entire feed were calculated for each infant.
Statistical analysis
Based on milk production data from Kent et al., 6 it was determined that this study had a power of 0.8 to detect a true difference in milk productions of 130 g.
All analyses were performed using R version 2.9.0 for Mac OS X. 10 The additional packages nlme 11 and lattice 12 were used for linear mixed modeling and lattice plots, respectively. Data are presented as mean±SD values except where the data were not normally distributed, in which case the median (first quartile, third quartile) is presented. Values of p<0.05 were considered significant.
Total milk production was defined as the sum of the amount of milk removed from both breasts, through breastfeeding and breast expression, over the entire period, normalized to 24 hours. 6 Breastfeeding variables defined for each breast and normalized to a 24-hour period included milk production, total feed duration, number of feeds, mean feed duration, and mean feed volume.
Groups were compared on continuous variables using Student's t test, with the Welch modification for unequal variances used when Bartlett's test of equality of variance indicated heteroscedasticity. Distributions of milk production levels in the two groups were compared with the two-sample Kolmogorov–Smirnov test. Categorical variables were assessed for group differences using Fisher's exact test. Univariate associations between measured variables and 24-hour milk production have been assessed using either t tests or linear regression as appropriate.
Relationships among 24-hour milk production, group, and feeding characteristics were tested using regression models with milk production as the response and measured variables and group as predictors. All variables with a significant or near significant (p<0.1) univariate relationship to milk production were included as predictors in the full regression model, with the exception of confounding variables. Stepwise selection was used, removing the least significant variable until all included variables had a p value of<0.1.
Results
Demographics
No systematic differences were detected between the two groups for any of the participant characteristics tested (Table 1).
Data are presented as median (lower quartile, upper quartile) or proportions.
Significantly different, p<0.05.
Pain characteristics
Women with persistent pain reported experiencing bilateral pain for a median length of 66 (43, 89) days. The pain intensities were lower for women who measured their 24-hour milk production compared with those who did not: measured, 22/100 (14, 44); not measured, 50/100 (36.5, 62.5) (p=0.011).
Breastfeeding alternatives
Women in the pain group were significantly more likely to feed expressed breastmilk (p=0.043) (Table 1), although reported daily pumping frequencies were not significantly different (p=0.296). A low number of women expressed during the monitored period (control, n=2; pain, n=4), and thus the effect of expressing on milk production was not assessed.
Nipple shields
Nipple shield use was only reported in the pain group, with five women regularly using a nipple shield (p=0.048). When low supply was defined as<500 g, there was a higher rate of low supply in those using nipple shields (p=0.028) within the pain group.
Feeding characteristics
Feeding volume, frequency, and duration were similar for the persistent pain and control groups, when either feeds or meals were considered (Table 2) (p>0.4 for all). In a 24-hour period, the infants had an average of six meals of approximately 110 g, and feeding patterns for both groups are shown in Figure 1.
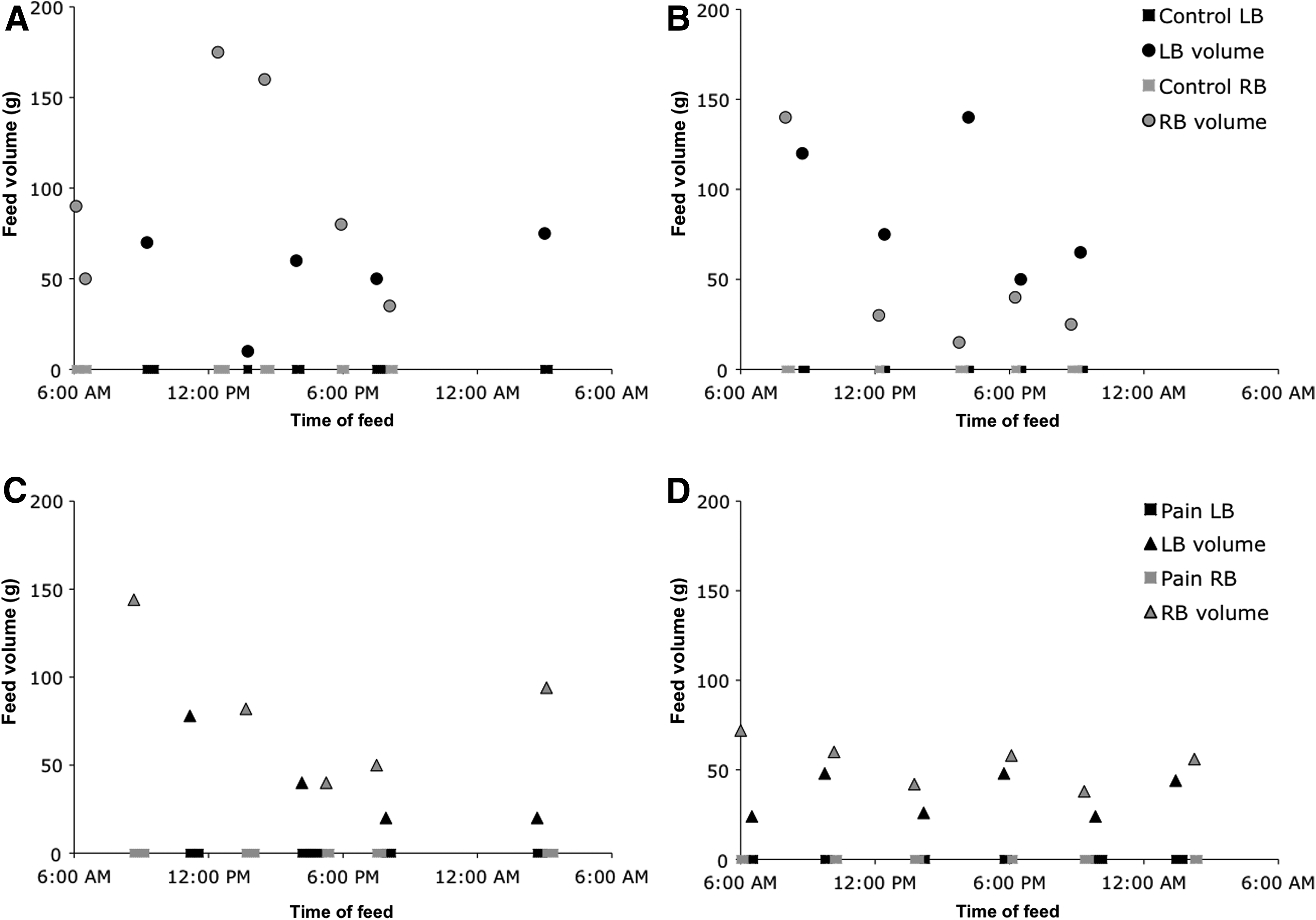
The 24-hour milk intake patterns by breast for two control group
Data are presented as median (lower quartile, upper quartile).
Sucking vacuum
There was a trend for mothers in the control group to measure milk production if their infant transferred less milk during intra-oral vacuum measurement (measured, 55.1±25.6 g, n=9; not measured, 78±30.7 g, n=21 [p=0.085]). Conversely, mothers in the pain group with higher milk transfer during intra-oral vacuum measurement were more likely to measure milk production (measured, 52.8±37.5 g, n=12; not measured, 34.0±24.6 g, n=18 [p=0.021]). Infants in the pain subgroup (n=21) of this study applied higher baseline (pain, –91.5±57.2 mm Hg; control, –38.4±25.4 mm Hg [p=0.003]) and peak (pain, –204.9±61.8 mm Hg; control, –151.7±45.7 mm Hg [p=0.004]) vacuums during the monitored feed compared with the control group (n=21). In the women who measured 24-hour milk production, no difference in milk intake was seen for the monitored feed: pain, 70 (38, 88) g; control, 68 (38, 80) g (p=0.916).
Milk production
Although the range of 24-hour milk production measured in the pain group (276–1,136 mL) was lower than that observed for the control group (510–1,324 mL), there were no significant differences in either the distribution (p=0.603) or the mean milk production (p=0.957) between the pain and control groups. Characteristics for the four women in the pain group with 24-hour milk production levels below the range seen in the control group (<500 mL) are shown in Table 3.
Significant univariate predictors of higher 24-hour milk productions were higher average feed (p<0.001) and meal volumes (p<0.001) and shorter average meal duration (p=0.008). Trends to higher milk production were demonstrated with increased infant age (p=0.066), vaginal delivery (p=0.078), and shorter average feed durations (p=0.054). There was no association between 24-hour milk production and baseline (p=0.589), peak vacuum (p=0.443), or infant sex (p=0.449). No significant univariate associations were detected between any of the remaining variables and 24-hour milk production.
There were different relationships seen between meal duration and 24-hour milk production for the two groups (Fig. 2). Although there was no relationship between meal duration and milk production for the control group (p=0.801), in the pain group an increase of 1 minute in meal duration was associated with a decrease of around 9 mL in milk production (p=0.017). Thus, in the pain group, short meal durations had higher milk productions than those with similar meal durations in the control group, those with meal durations of approximately 33 minutes had similar productions, and those with long meal durations had lower milk productions than the control group.
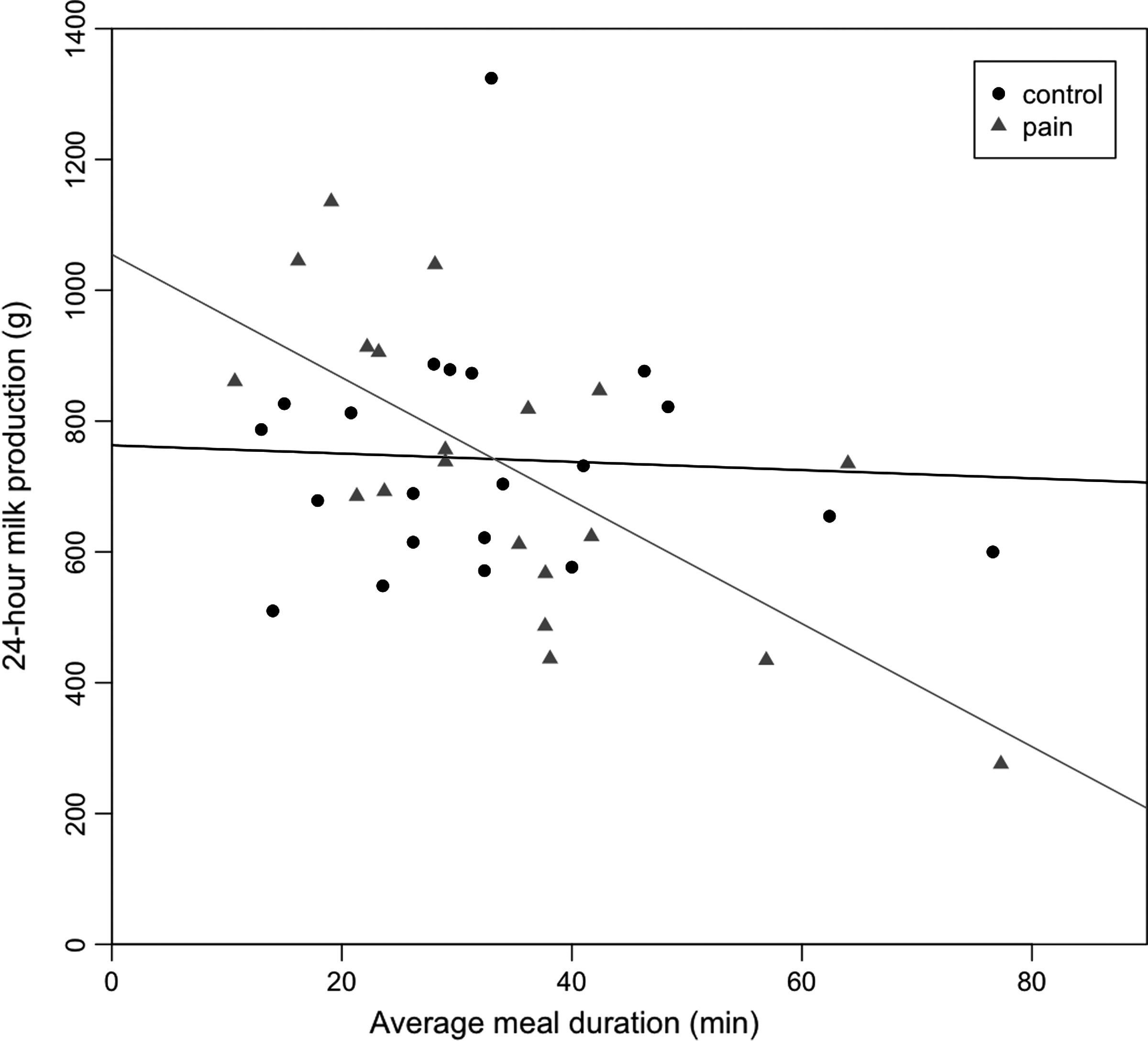
Relationship between 24-hour milk production and average meal duration for the pain and control groups. Regression lines for the relationship between meal duration and 24-hour milk production are shown for each group (pain=triangles, control=circles). The trend for infants in the pain group represents higher volumes at low meal durations and lower volumes at higher meal durations. The regression lines of the two groups intersect at approximately 33 minutes, indicating average meal durations longer than 33 minutes were associated with lower 24-hour milk production levels in the pain group.
When all measured variables were considered, the best linear regression model took into account meal duration and volume and mode of delivery, with shorter meal durations (p=0.011), greater meal volumes (p<0.001), and vaginal delivery (p=0.048) being significant predictors of higher 24-hour milk production.
Discussion
This study has shown that despite experiencing pain during breastfeeding, mothers with persistent nipple pain are able to achieve a full milk production. Furthermore, these women fed with similar duration and frequency as women not experiencing pain. The feed characteristics and milk productions of these mothers are similar to those of other cohorts of breastfeeding women not experiencing pain.6,13 The similar feeding characteristics suggest that pain does not result in lower 24-hour milk production as a consequence of fewer or shorter feeds and does not require more frequent or longer feeds. It is possible that the professional assistance received by mothers with pain may have contributed to this outcome. Also, the mothers recruited for this study had a high sociodemographic status, which is associated with longer length of breastfeeding.14–17 Thus, these women were likely to be highly motivated to breastfeed despite experiencing pain.
As the volume of milk transferred during a 24-hour period was similar for both groups, it is unlikely that the milk ejection reflex was adversely affected by the pain experienced during breastfeeding. Presumably, if the milk ejection reflex were impaired, milk transfer rates during feeding would have been lower for these women. In the study of Newton and Newton, 5 painful distractions resulted in decreased milk transfer for one feed, and the volume of milk received by the infant could be increased by the injection of oxytocin, the hormone that stimulates milk ejection. It is interesting that distractions that reduce milk transfer have been found to have less impact over time, as the mother becomes conditioned to the stimuli. 5 Therefore, it is conceivable that the women in this study may have become conditioned to experiencing pain over time.
Previously, we found that feed volumes were reduced in infants with strong sucking and mothers with persistent pain. 2 In this study, neither the mean baseline nor peak vacuum levels were related to milk production. Similarly, no relationships were detected between feed/meal durations and baseline/peak vacuums. This suggests that although strong sucking vacuums are applied neither milk synthesis nor removal rates are affected.
In the final regression model to predict 24-hour milk production volume, higher mean meal volume, shorter mean meal duration, and vaginal delivery were significantly associated with higher milk production. Thus it may be worthy to investigate the affect of mode of birth on established milk production levels in a larger cohort. Mode of birth has been recently shown to be associated with delayed onset of lactation 18 and reduced breastmilk transfer from Days 2 to 5 postpartum, 19 compared with vaginal deliveries. Thus cesarean section may be a barrier to breastfeeding success and worthy of further consideration.
Clinically, the only predictor of lower milk production was meal durations lasting longer than 33 minutes in the women with persistent nipple pain, and longer meal durations were not associated with lower milk productions in the control group. Reasons for long meal durations could be due to either maternal opinion of minimum feeding durations or that the infant may not appear to be settled and satiated at the end of the feed. Thus, it may be useful to monitor milk transfer in women who report long meal durations. It is interesting that in this study we did not find a relationship between infant sex and milk production, which differs from the previous findings of significantly higher milk productions (p=0.036) between mothers of boys (831±187 g) and those of girls (755±151 g). 6
Caution is required when applying these results to all mothers with persistent pain, as recruited mothers who measured their milk production differed from those who did not in two respects. First, those women who measured their milk production reported lower pain intensities than those who did not. The task may have been too onerous for those experiencing higher-intensity pain. Breastfeeding characteristics, such as feeding duration or expression frequency, may be different in women with high pain intensity as interference levels are likely to be higher. Also, it is unknown whether higher pain intensities affect oxytocin release, and subsequently milk transfer volume. Second, unlike our previous study of infant sucking vacuum, 2 milk transfers for the monitored feed were not different between the two groups (p=0.916). Women in the control group tended to measure their milk production if milk transfer during the monitored feed was lower, possibly for reassurance, whereas women in the pain group with higher milk transfer during the monitored feed were more likely to measure milk production. These tendencies may explain the more homogeneous spread of monitored milk intakes between groups in this study. Therefore, further investigation of a larger cohort of women with pain, especially those with high-intensity pain and low feed transfer, is necessary to determine which breastfeeding dyads may experience low milk production.
In this study, breastfeeding mothers with pain were more likely to use nipple shields and feed expressed breastmilk than breastfeeding mothers without pain as a means of reducing the level of their pain. Three of the five women experiencing pain and using nipple shields had low milk production (<500 mL). Nipple shields are not generally recommended as an intervention for nipple pain unless monitored by a knowledgeable health professional. Studies of the effect of nipple shields on milk transfer are conflicting. Early studies have associated nipple shields with reduced milk transfer,20,21 whereas more recent research in preterm and term infants suggests that ultrathin nipple shields do not affect milk transfer.22–24 Because it is not known whether the low milk production measured in mothers who were using nipple shields in this study was due to the shield itself or other factors that might potentially influence supply such as pain or low prolactin levels, monitoring of mothers using shields is strongly supported. Because of the small numbers of mothers using shields in this study, further research is required into the effect of nipple shields on milk transfer in term infants whose mothers experience pain.
Conclusions
It is possible that with professional support, breastfeeding women experiencing low-intensity persistent nipple pain can achieve a full milk production despite their infants applying strong vacuums. Those women who had difficulty reaching full milk production were not breastfeeding less frequently and were more likely to have long breastfeeding meal durations. Further research is required to determine if mothers with high-intensity nipple pain have compromised milk production.
Footnotes
Acknowledgments
Financial support in the form of a Ph.D. scholarship and unrestricted research grant was received from Medela AG, Switzerland.
Disclosure Statement
No competing financial interests exist.