
Abstract
Abstract
Background:
The negative outcomes associated with painful and damaged nipples have been widely documented in the breastfeeding literature. Numerous studies have been conducted evaluating topical preparations to treat nipple pain and damage with equivocal findings. No studies have evaluated the effectiveness of the increasingly popular all-purpose nipple ointment (APNO). The purpose of this trial is to evaluate the effect of the APNO versus lanolin on nipple pain among breastfeeding women with damaged nipples.
Subjects and Methods:
A double-blind, randomized controlled trial was conducted in a large single-site, tertiary-care hospital in Toronto, ON, Canada. Breastfeeding women (n=151) identified as having damage to one or both nipples were randomized to apply either APNO (intervention group) or lanolin (control group) to their nipples according to the trial protocol. The primary outcome was nipple pain at 1 week after randomization measured using the Short Form McGill Pain Questionnaire. Additional outcomes at 1 week after randomization and 12 weeks postpartum included nipple yeast symptoms and/or mastitis, rates of breastfeeding duration and exclusivity, and maternal satisfaction with infant feeding method and treatment ointment.
Results:
There were no significant group differences in mean pain scores at 1 week after randomization. Women in the lanolin group reported significantly greater satisfaction with their infant feeding method and had nonsignificantly higher breastfeeding duration and exclusivity rates at 12 weeks postpartum.
Conclusion:
Results suggest that APNO is not superior to lanolin in treating painful, damaged nipples.
Introduction
Various interventions have been evaluated in the treatment of painful, damaged nipples, including collegenase, 17 dexpanthenol, 17 soap and water, 17 tea bags,18,19 warm water compresses, 18 lanolin, 19 lanolin and breast shells,5,20 glycerin gel, 20 breast shells, 21 breastmilk and hydrogel dressings, 5 and topical antibiotic ointments. 10 Results from two systematic reviews suggest there is no evidence that any one intervention is superior to the others in the treatment of nipple pain or trauma.22,23
An all-purpose nipple ointment (APNO) has been used for women with painful or damaged nipples since approximately 2001. This ointment contains an antibacterial substance (15 g of mupirocin 2% ointment), an antifungal substance (miconazole powder to give a 2% concentration), and a hydrocortisone (15 g of betamethasone 0.1% ointment). Prescription information about the APNO is presently available on the Internet to women worldwide as a treatment for their sore and/or damaged nipples. However, there has been no research specifically evaluating this nipple ointment. The purpose of this trial is to evaluate the effect of the APNO versus Lanolin on nipple pain among breastfeeding women with damaged nipples.
Subjects and Methods
Participants
Participants were recruited from a large teaching hospital in Toronto, ON, Canada from November 2005 to August 2006. Eligible participants were all breastfeeding women who expressed they were experiencing nipple pain, had a visually apparent open area of skin on one or both nipples/areolas within the first 2 weeks postpartum, and who understood English. The exclusion criteria included (a) the continued use of finger feeding or a lactation device to give formula, (b) the use of a nipple shield, (c) breast reduction surgery or breast abnormalities that would preclude exclusive breastfeeding, and (d) maternal self-report of sensitivities or allergies to betamethasone, mupirocin, and/or miconazole.
Design and procedures
A single-site, double-blinded, randomized controlled trial was conducted (Fig. 1) following approval by Health Canada's Therapeutic Product Directorate (June 2005) and the participating hospital ethics review board. To recruit participants, the trial was briefly introduced to women who were identified by a staff nurse or lactation consultant as having nipple damage from breastfeeding. Verbal consent was then obtained to have the trial research assistant provide a detailed study explanation. Following informed consent procedures with eligible women, baseline data were collected, instructions for ointment application were explained and provided on a printed sheet, and the stopping policy was discussed. Participants were then randomized, and the ointment was provided. Randomization was centrally controlled by the hospital pharmacy using standard procedures for drug trials. Randomization numbers were generated in blocks of 20. One hundred sixty identical containers were filled with either lanolin or APNO by the hospital pharmacy in accordance with the standards of a double-blinded trial and sequentially numbered. Because of a slight difference in the appearance of the two ointments, inert food coloring was added to the APNO to make it look like lanolin. The ointments were placed in identical unmarked, opaque containers by the hospital pharmacy, which kept the randomization schedule until data collection was complete. A research assistant blinded to group allocation telephoned all participants at 1 week after randomization (Days 4–10 postpartum) and at 12 weeks postpartum to assess trial outcomes.
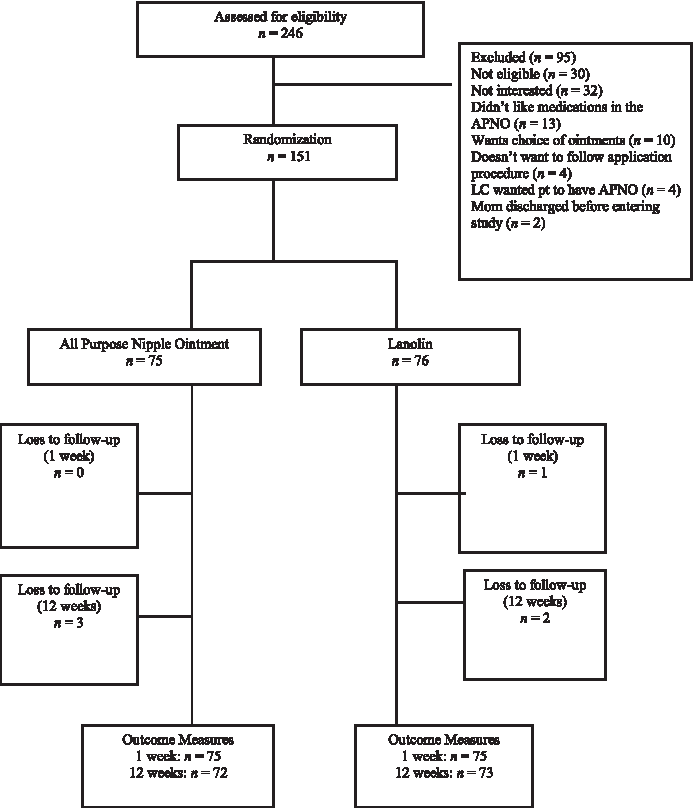
Schematic of trial recruitment. APNO, all-purpose nipple ointment; LC, lactation consultant; pt, patient.
Intervention
All participants were instructed to apply their ointment to their nipples and areolas sparingly after each feeding and to not wipe or wash off the cream prior to feeding their baby. Participants were asked to apply their ointment after each feeding for 10 days, then beginning with Day 11 apply ointment every other feeding for 4 days, and then on Day 15 apply no ointment. Participants were asked not to apply anything other than the treatment ointment or expressed colostrum/breastmilk to their nipples/areolas for the trial period. The length of intervention was chosen following discussions with two internationally known expert clinicians in breastfeeding medicine. All participants received routine postpartum care that included a referral to a lactation consultant for women experiencing damaged nipples.
Outcome measures
Nipple pain
The primary outcome was maternal nipple pain experienced at last breastfeed. Nipple pain was assessed at baseline, 1 week after randomization, and 12 weeks postpartum and measured using the Short-Form McGill Pain Questionnaire (SF-MPQ). 24 The SF-MPQ comprises a Pain Rating Index (PRI) and a Present Pain Intensity scale. The PRI is a 15-item questionnaire that uses descriptors to evaluate sensory and affective aspects of pain. Individuals select adjectives that best describe their pain and rank the severity of pain on a 4-point scale with 0=no pain to 3=severe pain. Scores are summed to produce a total score ranging from 0 to 45. The Present Pain Intensity is a 6-point pain scale to rate intensity ranging from 0=mild pain to 5=excruciating pain. The SF-MPQ also includes a visual analog scale, which was not used in this trial as follow-up data were collected via telephone. Instead, the widely used Pain Scale was administered where participants rated their pain on a scale ranging from 0=no pain and 10=worst possible pain. All pain assessments were based on perceived level of pain experienced at last breastfeed. The SF-MPQ has been widely used to assess the pain experience in numerous types of patients and has been used to evaluate the efficacy of various treatment regimens. 25 It has well-demonstrated psychometric properties. 26
Breastfeeding duration and exclusivity
Breastfeeding duration and exclusivity were assessed at 1 week after randomization and at 12 weeks postpartum. Breastfeeding was defined as the receipt of any breastmilk either by breastfeeding or by bottle in the past 24 hours and was measured with a “yes” or “no” response. Breastfeeding exclusivity was measured using levels of breastfeeding as defined by Labbok and Krasovec. 27 Responses included (a) exclusive breastfeeding (breastmilk only), (b) almost exclusive breastfeeding (less than 1 bottle/week of nonhuman milk), (c) high breastfeeding (<1 bottle/day of nonhuman milk), (d) partial breastfeeding (at least 1 bottle/day of nonhuman milk), or (e) token breastfeeding (breast given to comfort baby, but not nutrition).
Mastitis
This outcome was assessed at 12 weeks postpartum and was defined as any self-report of mastitis symptoms that met the designated criteria that occurred at or before 12 weeks postpartum. The mastitis symptoms assessment was based on the self-reported diagnostic criteria suggested by Fetherston. 12 The assessment for mastitis symptoms included questions specific to three different categories: (a) temperature, chills, or aches as a symptom of a breast infection; (b) one of either breast pain, lump, swelling, redness, or nipple crusts; and (c) symptoms lasting greater than 24 hours. To meet the criteria for mastitis symptoms, a “yes” response was required in each of the categories.
Nipple yeast symptoms
This outcome was assessed at 12 weeks postpartum and was defined as any self-report of nipple yeast symptoms that met the designated criteria described by Tanguay et al. 11 and Francis-Morrill et al. 28 The assessment for nipple yeast symptoms included questions specific to two different categories: (a) nipple and/or areola pain that is worse for 15 minutes after feeding, burning nipple pain, and/or needle-like pain in the nipple and/or areola; and (b) pink, red, or discoloration of the nipple and/or areola and/or swelling, shiny, cracks, itching, flaking, and/or pustules of the nipple and/or areola. To meet the criteria for nipple yeast symptoms, a “yes” response was required in each of the categories.
Maternal satisfaction with infant feeding method
This outcome was assessed at 12 weeks postpartum using a shortened version of the Maternal Satisfaction with Infant Feeding Questionnaire. 29 The 11 items are rated on a 5-point Likert-type scale where 1=strongly disagree to 5=strongly agree, to produce an overall score with higher scores indicating greater satisfaction with infant feeding method.
Maternal satisfaction with treatment
This outcome was measured at 12 weeks postpartum and included questions related to satisfaction with the effectiveness of the ointment. One item was rated on a 5-point Likert-type scale where 1=definitely satisfied to 5=definitely not satisfied. Five additional questions with diverse response formats were related to maternal report of ointment side effects (yes or no), a description of any side effects, and compliance with treatment protocol.
Sample size
The sample size was estimated with use of an equation appropriate for comparing two independent group means and was based on the ability to detect a moderate effect size of 0.50 in pain scores on the SF-MPQ subscale PRI. A moderate effect size was selected with the goal to detect a minimum 30% reduction in pain scores. Thus, with 80% power, a two-tailed α error of 0.05, and using a moderate effect size of 0.50 in the treatment of pain at 1 week after randomization, a sample size of 128 (64 per group) was required; we planned to enroll 150 to allow for losses to follow-up.
Data analysis
Data were analyzed using SPSS version 15 and an intent-to-treat approach. A significance level of 0.05 was used for all outcome data. Continuous variables were analyzed using the two-sample two-sided Wilcoxon test or t test. For binary variables, χ2 analyses were carried out, and one-way analysis of variance was used to assess differences between groups on categorical variables.
Results
In total, 151 women were recruited into the study. Characteristics of trial participants are presented in Table 1. There were no clinically important differences in baseline characteristics between the two groups. Of the women who were randomized, 75 (100%) of the APNO group and 75 (98.7%) of the lanolin group completed the assessment 1 week after randomization. At 12 weeks postpartum, 72 (96%) women in the APNO group and 73 (96.1%) in the lanolin group completed the outcome assessment. Participants were considered compliant if they described using their ointment for at least half of the recommended amount of time. Fifty-seven (79.2%) of women in the APNO group and 59 (80.8%) in the lanolin group described using the ointment exactly as recommended.
Data are mean (SD) values.
Data are n (%) values.
Clinical outcomes
Nipple pain
Both groups reported considerably less nipple pain on all pain outcome measures from baseline to 1 week after randomization. No significant group differences were found in pain scores for the SF-MPQ subscales or the Pain Scale (Table 2).
By Wilcoxon two-sided test.
One week after randomization.
Breastfeeding duration and exclusivity
At 1 week after randomization, only two women in each group had discontinued breastfeeding. Breastfeeding exclusivity at 1 week after randomization had increased from baseline levels by approximately 20% for the women using APNO and 15% for the mothers using lanolin (Table 3). There were no significant group differences in level of breastfeeding at 1 week after randomization (F1,147=0.515, p=0.47). At 12 weeks postpartum, 20 (27.8%) women in the APNO group had discontinued breastfeeding compared with 11 (15.1%) in the lanolin group. Breastfeeding exclusivity rates were also higher among mothers in the lanolin group (n=44, 60.3%) compared with mothers in the APNO group (n=33, 45.8%). However, this difference did not reach statistical significance between groups (F1,143=3.48, p=0.06).
Data are n (%) values.
One week after randomization.
Twelve weeks postpartum.
Mastitis and nipple yeast symptomatology
At 12 weeks postpartum, three (4.1%) women in the APNO group and two (2.7%) in the lanolin group described symptoms of mastitis that met the designated criteria. In relation to nipple yeast, six women (8.1%) in the APNO group and eight (11 %) in the lanolin group described symptoms of nipple yeast that met the diagnostic criteria.
Nipple healing times, maternal satisfaction, and side effects
To further understand any treatment effect and change in infant feeding status across time, we examined nipple healing times. Approximately one-third of women in both groups (APNO, 33.3%; lanolin, 31.5%) indicated nipple healing (yes or no response) had occurred during the first week of treatment. No significant difference in healing time was found between the groups (χ2=0.502, p=0.97). Approximately one-fifth of all women reported that healing did not occur until 8–14 days following treatment initiation (APNO, 26.4%; lanolin, 23.3%), and about 30% of women indicated that healing did not take place until 15–21 days (APNO, 16.7%; lanolin, 19.2%) or longer (APNO, 11.1%; lanolin, 13.7%).
Women in the lanolin group reported significantly higher levels of satisfaction with their breastfeeding experience (mean=48.05, SD=5.96) than those in the APNO group (mean=44.93, SD=7.73) (t143=–2.73, p<0.01). However, there were no significant group differences related to maternal satisfaction with ointment (F1=.027, p=0.87). Sixty-five (90.3%) women in the APNO group and 68 (93.1%) in the lanolin group were satisfied with the effects of the ointment in treating their nipples. Only two women in the APNO group and one in the lanolin group reported side effects. In the APNO group, one woman experienced an uncomfortable stinging sensation from the ointment and discontinued use after 24 hours of applications, and another experienced a burning sensation and discontinued use after 2 days. Similarly, one woman in the lanolin group reported severe itching and burning and discontinued use after 1 day.
Discussion
The purpose of this randomized controlled trial was to evaluate the effectiveness of APNO versus lanolin for the treatment of painful, damaged nipples among breastfeeding women. Overall, APNO was not a more effective treatment than lanolin. In particular, there were no significant group differences related to nipple pain, breastfeeding duration and exclusivity rates, mastitis and nipple yeast symptoms, nipple healing time, ointment side effects, and satisfaction with treatment. This is the first trial to evaluate the effectiveness of APNO on breastfeeding outcomes, and the findings are consistent with two previous systematic reviews.22,23 Currently, there is limited evidence available to clearly indicate what is the most effective treatment for painful, damaged nipples, and additional research in this area is warranted. However, an important study finding is that within the first week after treatment initiation pain scores decreased significantly, and about one-third of all women experienced nipple healing. This suggests that either ointment may have a potential beneficial effect for women experiencing nipple pain or damage.
Although all study participants were experiencing nipple pain and damage, the rate of breastfeeding continuation was high with approximately 97% of women breastfeeding at 1 week after randomization. At 12 weeks postpartum, approximately 78% of all study participants were breastfeeding, of whom 53% were doing so exclusively. However, it is interesting to note that at 12 weeks postpartum 85% of women in the lanolin group were breastfeeding, in comparison with 72% in the APNO group who were breastfeeding. Although these results are not statistically significant, it may be clinically important that more women in the APNO group had discontinued breastfeeding in comparison with women in the lanolin group. However, the breastfeeding rates in both groups were higher than other rates (67.6%) reported in national Canadian studies. 30
This trend was also evident regarding rates of breastfeeding exclusivity. As noted, more mothers in the lanolin group were exclusively breastfeeding at 12 weeks postpartum compared with APNO mothers, although the difference was not statistically significant. In relation to other breastfeeding studies, mothers in the lanolin group had higher rates of breastfeeding exclusivity (60%), whereas mothers in the APNO group (46%) were more on par with other rates (52%) reported in Canadian and U.S. studies.30,31 The almost 15% difference in breastfeeding exclusivity among mothers using lanolin may be clinically important.
These findings regarding breastfeeding duration and exclusivity are interesting in that nipple pain/trauma has been a frequently reported variable related to low breastfeeding duration and exclusivity.6,7,32 This suggests that the mothers in this study may have had a high degree of commitment/motivation to breastfeed and continued despite the difficulties encountered. There is some evidence to support the higher rates of breastfeeding in this study. First, at the baseline assessment the majority of mothers felt that breastfeeding was progressing “very well” or “good” despite having nipple pain, suggesting they had positive attitudes toward breastfeeding. Second, the majority of mothers in this study were married, had an average age of 32 years, and were university educated. These demographic variables (marital status, age, education) have been associated with increased rates of breastfeeding 32 and increased breastfeeding self-efficacy. 33 Self-efficacy has been identified as a salient variable affecting breastfeeding outcomes among diverse populations.34–37 Mothers who are efficacious in their breastfeeding abilities will be more likely to initiate breastfeeding, put forth greater effort and persist with breastfeeding when difficulties are experienced, and have positive thought patterns and emotional reactions to breastfeeding. 38
The incidence of both mastitis and/or any yeast symptoms was very low in both groups; thus this study was inadequately powered to detect any significant differences between groups. Based on the power analysis, a sample size of 416 would have been needed to detect significant differences between groups regarding mastitis symptoms if the mastitis rate was 25%.
Women in the lanolin group were significantly more satisfied with their breastfeeding experience than those in the APNO group, and this may be related to the fact that more mothers in the APNO group discontinued breastfeeding by 12 weeks than those in the lanolin group. Studies have found that women who discontinue breastfeeding prematurely often have more negative perceptions of their infant feeding experience.39,40 Despite these differences in satisfaction with infant feeding experience, almost all women independent of treatment group allocation were satisfied with the effects of the nipple ointment. This may be related to the facts that very few women experienced any negative side effects and that almost all women had a decrease in nipple pain 1 week after treatment was initiated. This may have also contributed to the high degree of protocol adherence.
There are many strengths of this trial. It incorporated a centrally controlled randomization process, and participants, health providers, and outcome assessors were all blinded to group allocation. There was a high study acceptance rate among eligible women, and losses to follow-up were less than 10%. The application of ointment was standardized, and compliance rates were high. A power analysis was completed to determine the sample size, and data were analyzed using an intent-to-treat approach. Despite these strengths, the sample was homogeneous, limiting the generalizability of the results. Additional research is warranted with a sample at higher risk for poor breastfeeding outcomes.
Conclusions
APNO does not appear to be more effective than lanolin in the treatment of painful, damaged nipples. Further evaluation of treatments should be considered and include a larger sample so that the outcomes of mastitis and nipple yeast symptoms may be evaluated.
Footnotes
Acknowledgments
We gratefully acknowledge The Canadian Foundation for Women's Health and the Maternal/Infant Program at Mount Sinai Hospital for funding the study. We thank Dr. Jackie Thomas, the late Dianne Younker, and Dr. Jack Newman for their support and assistance. We thank the 10th and 7th Floor Nursing staff, the Lactation Consultants, and Shafagh Fallah, Statistician, from Mount Sinai Hospital. Additionally, we want to thank the women who participated in the study.
Disclosure Statement
No competing financial interests exist.