
Abstract
Abstract
Objectives:
Despite popular and historical use, there has been little modern research conducted to determine the safety and efficacy of herb use during breastfeeding. The purpose of this study was to systematically review the clinical literature on herbal medicine and lactation.
Methods:
The databases PubMed, CAB Abstracts, Cochrane Central Register of Controlled Trials, HealthSTAR, Cumulative Index to Nursing and Allied Health Literature, and Reprotox were systematically searched for human trials from 1970 until 2010. Reference lists from relevant articles were hand-searched.
Results:
Thirty-two studies met the inclusion criteria. Clinical studies were divided into three categories: survey studies (n=11), safety studies (n=8), and efficacy studies (n=13). Six studies were randomized controlled trials. The most common herbs studied were St. John's wort (Hypericum perforatum L.) (n=3), garlic (Allium sativum L.) extract (n=2), and senna (Cassia senna L.) (n=2). Studies were very heterogeneous with regard to study design, herbal intervention, and outcome measures. Overall, poor methodological quality predominated among the studies.
Conclusions:
Our review concludes that further research is needed to assess the prevalence, efficacy, and safety of commonly used herbs during breastfeeding.
Introduction
The World Health Organization recommends exclusive breastfeeding for the first 6 months of life as the best nutrition for the infant. 4 In many cultures, the knowledge of herbal galactagogues (herbs that increase milk production) is passed down from generation to generation. Examples of herbal galactagogues include fenugreek, blessed thistle, milk thistle, fennel, anise, nettle, and others; however, there are very few modern data on their safety and efficacy.5,6
Under the 1994 Dietary Supplement Health and Education Act, herbal medicines are held to different regulatory standards than prescription medications. At present, there are concerns about the quality and safety of herbal products during pregnancy and lactation. 7 The primary purpose of this study was to systematically review the existing clinical studies on herbal dietary supplement use among breastfeeding women. The secondary purpose was to assess the methodological quality of existing clinical trials.
Methods
Type of studies, participants, and outcome
Only human trials were included. The studies were divided into three categories: survey studies, safety studies, and efficacy studies.
Search methods for identification of studies
The databases PubMed, CAB Abstracts, Cochrane Central Register of Controlled Trials, HealthSTAR, the Cumulative Index to Nursing and Allied Health Literature, and Reprotox were systematically searched from 1970 to November 2010. Additionally, we hand-searched the bibliographies of obtained articles for additional publications that would meet our criteria. The articles were identified from databases using MeSH terms such as “lactation” or “breastfeeding” or “galactogogue” and were combined with MeSH terms such as “plant extract” or “herb” or “medicinal herb” or “dietary supplement” or “phytotherapy.” Only articles written in English, human trials, published studies (no dissertations), and studies with abstracts were included in the review. We included articles that were published between 1970 and 2010.
Data collections
The initial database searches identified 1,575 articles (Fig. 1). After duplicate articles were removed, 942 abstracts were reviewed by two independent reviewers (K.B. and P.G.) for eligibility criteria. Exclusion criteria were as follows: (1) studies without abstracts, (2) dissertations, (3) vitamins/minerals/non–plant-based products, (4) review articles, (5) animal studies, and (6) in vitro studies. Only 62 clinical studies met the eligibility criteria. After the full text was reviewed, 32 studies were included in the final analysis. The abstraction tool assessed the studies in three parts: (1) aim of the study, study design, study population, and study characteristics; (2) modified Herbal Consort checklist; and (3) modified Jadad criteria.8,9

Search flow to obtain studies examined in this article.
The Herbal Consort score looks for inclusion of certain information about the herb in question, as well as the quality of adverse event reporting. The Jadad scale looks at various characteristics of randomized controlled trial (RCT) and non-RCT study design. We modified the “Consort Items for Randomized Controlled Trials of Herbal Medicine Interventions” to create a quality score to access the methodological value of each study. 8 Our modified scale contains seven items (best score=7; worst score=14). If an item had multiple criteria listed, we assigned the lower (better) score if one of them was met (see Appendix 1). To assess the quality of the RCTs, a Jadad criterion was used; to assess the quality of non-RCTs, a modified Jadad criterion was created (see Appendix 2). 9
Results
In total, 32 studies were included in this review (see Fig. 1). Thirty full text articles did not meet our eligibility criteria: 14 discussed non-herbal dietary supplements, two were in vitro studies, two were reviews, eight were studies where the lactating mother did not use herbs, and four studies did not meet inclusion criteria (see Fig. 1).
Table 1 provides summaries of the study characteristics, aims of studies, and the quality of the studies. In Table 1, the studies are divided into three main categories: survey studies (n=11), safety studies (n=8), and efficacy studies (n=13). Six studies were RCTs.
N, name of plant/dietary supplement; L, Latin name (genus species); D, dose; T, type of product.
Zuo yuezi is the month postpartum in China associated with a variety of traditional beliefs and practices. Zuo yuezi included: dietary changes, such as eating more food and avoiding “cold food,” behavioral changes, hygiene changes, and practices associated with infant feeding, including supplementary feeding and giving honeysuckle herb to the infant.
Trademark of Madaus Pharmaceuticals (Pty) Ltd.
Trademark of Purdue Products L.P.
APCD, acquired prothrombin complex deficiency; NA, not available; NRCT, non-randomized controlled trial; RCT, randomized controlled trial; S, study type; sIgA, secretory immunoglobulin A; TID, three times a day.
The 32 studies were very heterogeneous with regard to the specific herbs studied. The most common were St. John's wort (Hypericum perforatum) (n=3), garlic (Allium sativum) extract (n=2), and senna (Cassia senna) (n=2). Fourteen studies did not include genus species (Latin) names. Five studies did not mention common herbal names. Fifteen studies did not include dose. The dosage form (i.e., tea, capsule, powdered herb) was not described in 13 articles. Among the other 16 articles, the most common types of product were modified extract (n=6), tea (n=3), capsule (n=3), concentrated extract (n=3), and tincture (n=2). Many studies used multi-ingredient herbal preparations ranging from one to 35 single herbs.
The sample size of the studies ranged from one to 471 subjects. Four published studies did not document sample size. In terms of subject characteristics, 72% did not document subject's education, 75% did not document income, 84% did not report subject's ethnicity, and 28% did not document patient's age.
The quality of study methodology, using the modified Herbal Consort criteria, ranged from 8 (n=1) to 14 (n=5) on a scale of 7–14, with 7 indicating the highest quality study (Fig. 2). Figure 2 shows the distribution of the modified Herbal Consort scores. In terms of quality scores, the modified Jadad scores ranged from −1 to 4 for RCTs (scale of −2 to 5) and 1 to −2 for non-RCTs (scale of −2 to 3). The lowest quality score is represented by −2.
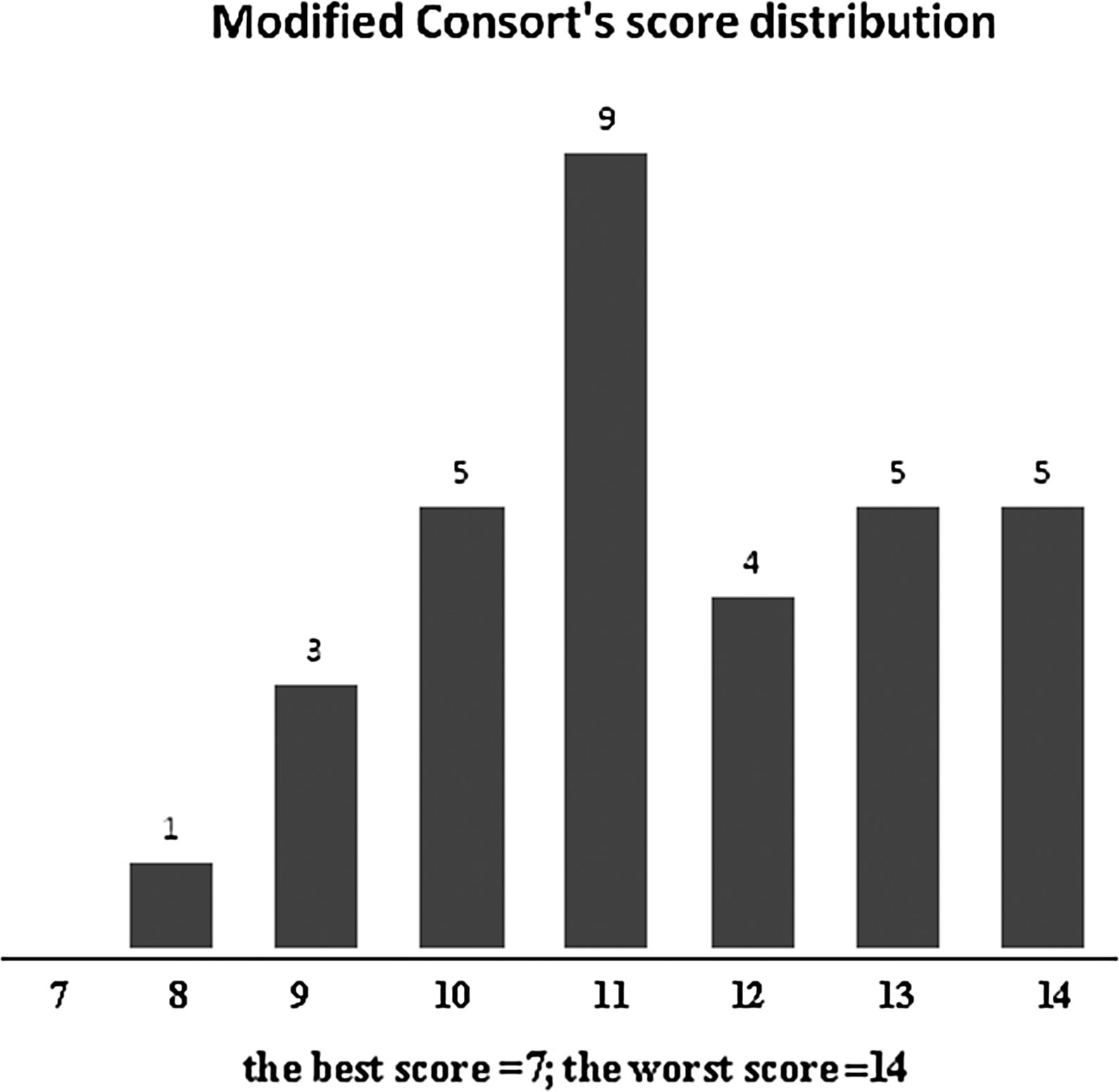
Distribution of quality scores.
Table 2 presents the survey studies. As shown in Table 2, the main outcomes are qualitative, describing the list of plants commonly used by postpartum women or herbal dietary modifications that were done to help increase milk production. Most of these studies did not discuss safety of the herbal intervention in the women or newborns.
There were a total of eight published safety studies, which included Senna spp. (Cassia spp.) (n=2), St. John's wort (H. perforatum) (n=3), herbal liqueur (n=1), and a traditional Chinese herb (n=1) (Table 3). One case-control study reported a potential serious side effect, acquired prothrombin complex deficiency syndrome, among Thai infants consuming an herbal liquor. 10 The herbal ingredients were not disclosed in the article.
There were 13 efficacy studies: seven had outcomes in the mother, two in the infant, and four in both mother and infant (Table 4). Outcomes were measured in numerous ways, including milk intake by infant, biomarkers such as prolactin and oxytocin levels in the mother, weight of infant, duration of the infant attached to the mother, decrease of duration of illness, or levels of antibodies in milk.
NS, not significant.
Discussion
This systematic review of herb use in breastfeeding women identified 32 studies in the last 40 years: survey studies (n=11), safety studies (n=8), and efficacy studies (n=13). These studies have heterogeneous interventions, study designs, and outcomes measured. Many studies on safety or efficacy were of poor methodological quality. In considering the scores from the modified Jadad and modified Herbal Consort assessment tools, it should be noted that the modifications to these tools were not validated but provide a basic assessment of the quality of the research.
Although other reviews, such as those of Anderson and Valdes, 11 Conover and Buehler, 12 Belew, 13 Low Dog, 14 and Dugoua et al., 15 have focused on the use of single herbs or pharmaceutical agents during breastfeeding or preconception, this review included multiple herbs and herbal formulas only during breastfeeding. One of the major highlights of this review is reporting the deficit in published data on herb use among breastfeeding women in the United States.
In our review, we documented eight clinical safety studies, only one of which was an RCT 16 (Table 3). In Thailand, one case-control study of 20 infants with acquired prothrombin complex deficiency syndrome reported higher rates of postpartum mothers using an herbal liquor extract compared with controls (n=60). 10 The authors did not report the ingredients used in the herbal liquor. The two studies of senna and two studies of St. John's wort reported no adverse events.17,18 One study of St. John's wort did note change in infant behavior that did not require intervention by the primary care provider. 19
The four efficacy studies were RCTs and reported diverse outcomes such as using biomarkers, weight gain or loss, or time attached to the mother's breast. Only one study showed that breastmilk intake was higher than in the placebo group.
Many women consume herbal teas during breastfeeding, and there are many breastfeeding teas in the marketplace. (Note that tea technically refers to water extracts made from the tea plant [Camellia sinensis], but herbal tea is part of the common vernacular and is used in this article.) It is surprising that there are few data on the safety or effectiveness of fenugreek, one of most common herbal dietary supplements used by breastfeeding women. A 2011 study published by Turkyilmaz et al. 20 found an herbal tea with fenugreek significantly increased milk production in breastfeeding women. However, it was not included in this review because the inclusion criteria specified articles published between 1970 and 2010.
According to Herbal Consort guidelines, good quality studies should include randomization, blinding, and placebo control.8,11 Most of the herbal studies did not meet Herbal Consort guidelines; for example, the studies were not RCT but open-label, case-control, or before–after studies. Additionally, none of these studies met full criteria for the Herbal Consort criteria that provide guidelines for the reporting of herbal interventions, particularly for RCTs. 8 For example, most studies did not report the Latin (botanical) name of the herb being studied, and some did not include the common name of the herb
This systematic review has limitations, including not reviewing non-English studies, animal studies, and in vitro studies. We chose to focus on human data because of the prevalence of the use of herbs by nursing women and the relevance of human studies to nursing women. Although animal studies can provide useful information on the safety and efficacy of herbs, the results may not be directly applicable to human clinical use. The exclusion of non-English articles was due to a lack of resources to translate articles written in other languages.
Currently, in the United States, herbal products are regulated as dietary supplements, and supplement manufacturers are responsible for generating or compiling evidence of safety and efficacy for their products. 21 As pre-market approval for supplements is not required by the Food and Drug Administration, there are no existing regulatory guidelines in the United States that propose a risk assessment or protocol to determine the safety and efficacy of herb use during breastfeeding. In the European Union, where herbal products are regulated as medicines and require pre-market approval from the government, a risk assessment protocol for medicinal plant safety during breastfeeding has been developed. 22 The risk assessment integrates evaluation of nonclinical and clinical data and includes consideration of nonclinical pharmacological and pharmacokinetic properties of the medicinal product, as well as results from nonclinical toxicity studies and clinical experience. 22 Similarly, in Canada, herbal products are regulated as Natural Health Products and require pre-market approval from the government. 23 Evidence of safety and efficacy must be provided for a product to be granted a Natural Health Products license, and higher levels of safety evidence must be provided for products intended for use by vulnerable populations (i.e., pregnant or nursing women).
Therefore, there are international models that can be used to assess the safety or efficacy of herbal products during pregnancy and lactation, and further research agendas should take into account high-quality basic science and clinical research on newborns and their mothers.
Conclusions
In conclusion, based on the limitations of the available literature, it is difficult to develop accurate information on the safety and efficacy of specific herbs during breastfeeding. It is critical that more research is conducted in this area, including national prevalence, safety, and efficacy studies. Furthermore, careful thought must be put into appropriate outcome measures and methods needed to address the ethics of doing such studies in such a vulnerable population. It may be that novel research methods will be needed to address such a large research agenda.
Footnotes
Acknowledgments
P.G. is the recipient of grant K07AT005463 from the National Center for Complementary and Alternative Medicine. K.B. is the recipient of Physician Training Award in Preventive Medicine 97-185-12 from the American Cancer Society.
Disclosure Statement
Z.E.G. is employed by Traditional Medicinals, Sebastopol, CA. K.B., J.-J.D., T.L.D., and P.G. have no competing financial interests.