
Abstract
Abstract
Abdominal pregnancy is a rare condition with significant risk of maternal and fetal morbidity and mortality. Because of the vascular involvement, the placenta is often left in situ. Prior reports have neglected to discuss the implications of leaving the placenta in situ on breastfeeding and lactation. We present a case of failure of lactogenesis II following the successful delivery of an advanced abdominal pregnancy in which the placenta was left in situ. This is the first report to discuss the effects on lactation of leaving the placenta in situ as a conservative management option in advanced abdominal pregnancy.
Introduction
Delayed lactogenesis and insufficient milk production have been noted in patients with retained placental fragments.1,2 Prior reports of leaving the placenta in situ have neglected to discuss the implications of a completely retained placenta on breastfeeding and lactation. We present a case of failure of lactogenesis II following the successful delivery of an advanced abdominal pregnancy in which the placenta was left in situ.
Case Report
A 39-year-old African American G1P0 presented at 8 weeks for routine prenatal care. Her pregnancy was complicated by chronic hypertension well controlled without medication. She also had a history of myomectomy with appendectomy due to a leiomyoma with ischemic necrosis and multiple subserousal fibroids. Pregnancy was confirmed by transvaginal ultrasound at her initial 8-week visit.
At 25 4/7 weeks of gestation the patient presented for follow-up. Ultrasound revealed a cervix that ended blindly in a fibroid of the lower uterine segment and an extrauterine gestational sac with no identifiable uterine wall. The placenta appeared to be implanted on the right portion of the uterine fundus extending laterally to the right pelvic sidewall overlying the internal iliac artery, extending over the bifurcation of the aorta and overlying the right renal vein and inferior vena cava. Power Doppler suggested major vascular supply to the placenta from the uterine fundus with additional placental vascular flow from the right uterine artery separate from the fundal implantation site and vascular supply from the right renal artery.
The findings and implications were discussed at length with the patient and her family, and she was admitted on hospitalized bed rest. Abdominal pregnancy was confirmed by magnetic resonance imaging, which revealed an extrauterine pregnancy located along the right flank. As shown in Figure 1, the fetus was surrounded by amniotic fluid and was located superior to the uterus. The uterus was enlarged and contained multiple uterine fibroids, the largest of which was 6.9 cm to the left of midline. Magnetic resonance angiography was then conducted in order to confirm placental vascular involvement. As shown in Figure 2, abdominal magnetic resonance angiography revealed an intraabdominal, extrauterine pregnancy with an arterial vascular supply via bilateral internal iliac arteries.
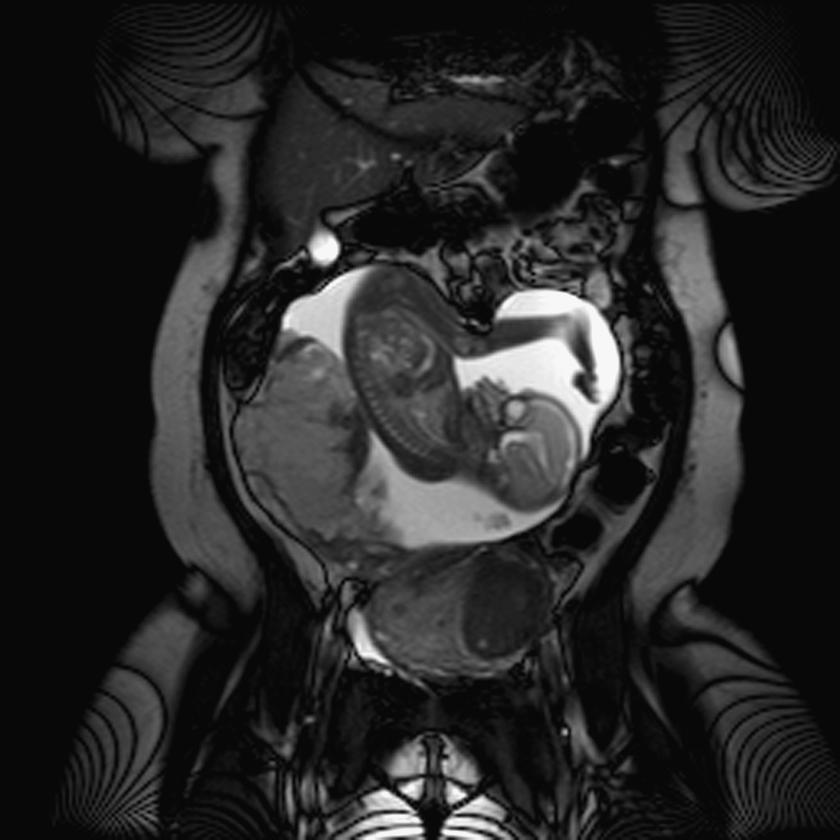
Magnetic resonance imaging of abdominal pregnancy at 25 4/7 weeks of gestation.
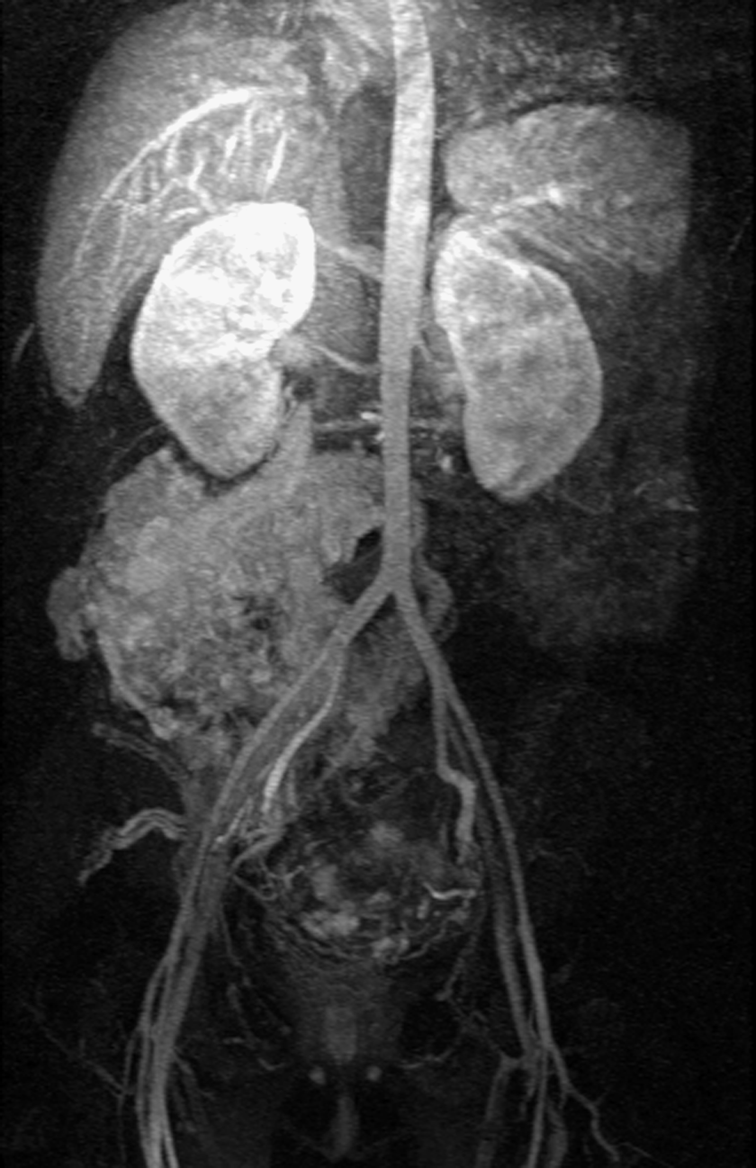
Magnetic resonance angiography of abdominal pregnancy at 25 4/7 weeks of gestation.
A multidisciplinary team including vascular surgery, general obstetrics, maternal fetal medicine, neonatology, blood banking, and anesthesia was included in the plan of care. Inpatient management included type- and cross-match for 4 units of packed red blood cells at all times, a protocol for massive blood, two large-bore intravenous lines, twice weekly complete blood counts, twice weekly limited ultrasounds looking for evidence of intraabdominal bleeding, daily electronic fetal monitoring, and repeat betamethasone series. The patient remained stable, and weekly ultrasounds confirmed maternal and fetal well-being with no evidence of compromise or hemodynamic instability. The patient declined intervention until 28 weeks.
At 28 1/7 weeks the patient was scheduled for a laparotomy and delivery. She was placed under general anesthesia with invasive monitoring. Surgical management began by a fluoroscopic-guided Fogarty balloon catheterization of bilateral hypogastric arteries in preparation for balloon occlusion if needed in an emergency. A midline vertical incision was then created. The placenta was noted to be attached to the right fundal region of the uterus extending laterally to the pelvic wide wall and cepahalad toward the right renal fossa, embedding into the anterior peritoneum. The fetus was noted to be in a transverse position with tense membranes filled with amniotic fluid. A small 1.5-cm incision was created, and a suction catheter was placed at the opening of the amniotic sac to prevent rapid decompression. After drainage of the fluid, the amniotic membrane incision was extended, and the fetus was delivered through the abdominal incision. A viable male infant with Apgar scores of 7 and 9 at 1 and 5 minutes, respectively, and weighing 1,205 g was delivered and handed to the Neonatal Intensive Care Unit team.
The placenta was re-inspected, and the initial findings were confirmed. The decision was made to leave the placenta in situ as it was embedded, not freely mobile, and had significant vascular supply. The cord was ligated at the placental base, membranes were trimmed, and the placenta was left in situ. After 15 minutes of observation, the placenta remained intact, and hemostasis was maintained.
Arteriography was performed, revealing hypervascualrity with an enlarged uterus and markedly enlarged bilateral uterine arteries serving the placenta in the right lower quadrant. Embolization was performed via right and left uterine arteries to achieve hemostasis. Follow-up arteriograms confirmed embolization. An abdominal aortogram was then performed, which demonstrated residual vascularity in the region of the placenta. Systemic arterial branches arising from the right hypogastric artery leading up to the area of the placenta were also noted. Completion aortogram revealed some persistent vascularity in the region of the placenta. However, it was markedly reduced from the pre-embolization arteriograms.
Intraoperatively, the patient was presumptively given 2,700 mL of crystalloid, 4 units of packed red blood cells, 2 units of fresh frozen plasma, 1 unit of cryoprecipitate, and 10 packs of platelets. However, given the decision to leave the placenta in situ, documented intraoperative blood loss was only 1,000 mL. The patient remained hemodynamically stable. Preoperative hemoglobin and hematocrit (H/H) levels were 13.4 g/dL and 39.1%, respectively; respective intraoperative H/H levels were 13.6 g/dL and 40.7%, respective postoperative H/H levels were 13.2 g/dL and 39.4%, and respective H/H levels on postoperative Day 5 were noted to be 12.7 g/dL and 37.4%.
Postoperatively, the patient was taken to the Cardiovascular Recovery Unit for continued observation and continued respiratory support. The patient was extubated on postoperative Day 1 and transferred to O2 therapy of 3 L by nasal cannula. She remained hemodynamically stable; on postoperative Day 2 the vascular introducers were removed, and the patient was transferred to the floor for routine care postoperative and postpartum care.
Breast pumping was initiated on postpartum Day 1 while the patient was still in the Cardiovascular Recovery Unit. The patient initially pumped two times during a 24-hour period. On postpartum Day 2 the patient increased the number of pumping sessions and pumped every 4 hours. A double hospital-grade breast pump was used for all pumping sessions, and the patient received extensive lactation support during her hospital stay. On postpartum Day 2 the patient produced a few drops of colostrum. The patient continued this pattern of breast pumping every 4 hours with no breastmilk production. On Postpartum day 6 the patient produced one drop of white breastmilk, the volume of which was not obtainable or measurable to give her infant in the Neonatal Intensive Care Unit. Kangaroo care was initiated on Day 7 with no change in breastmilk production, and on Day 8 the patient discontinued breast pumping. The patient confirmed breast changes during pregnancy but had no noted breast changes or engorgement following delivery notable for lactogenesis II. The patient experienced no breast changes or engorgement upon cessation of breast pumping. She was discharged home on postoperative Day 8 in stable condition with close postpartum outpatient follow-up.
At 2 months postpartum, the patient remained in stable condition, was noted to have returned to her normal menses, and had a quantitative beta-human chorionic gonadotropin of 19 milli-international units per milliliter (mIU/mL). At a 6-month postoperative visit, a repeat abdominal computed tomography scan was performed. An enlarged uterus with multiple fibroids and a low-density lesion superior to the uterus was noted. The low-density lesion, presumed to be the retained placenta, was noted to be reduced in size from 12.5×9.0 cm to 8.4×7.8 cm. At 8 months postpartum a urine human chorionic gonadotropin test and quantitative beta-human chorionic gonadotropin test were both negative, and the patient had an essure hysteroscopic sterilization. No further hormonal studies were performed.
The infant had an uncomplicated neonatal course with the exception of a patent ductus arteriosis, inguinal hernia, and an undescended testicle and phymosis. At 37.4 weeks adjusted gestational age, he was noted to be growing and developing appropriately and was discharged home in stable condition.
Discussion
Milk secretion is inhibited by the presence of estrogen, placental lactogen, and progesterone produced by the placenta. Progesterone interferes with prolactin by binding to the receptors on alveolar cells within the breast and directly suppressing milk production. Circulating levels of progesterone drop rapidly after the delivery of the placenta, triggering the initiation of lactation and allowing prolactin to act unopposed to stimulate milk production. Several human and animal case reports have noted retained placental fragments as a cause for a delay or failure of lactogenesis II in which lactogensis was initiated following removal of the retained products.1–3
In order to determine the effects of leaving the placenta in situ in advanced abdominal pregnancies and the effect on lactation, a literature review was conducted. A MEDLINE search was performed using the MESH terms “pregnancy, abdominal,” “breastfeeding,” “lactation,” “lactogenesis,” “placenta,” and “placenta, retained.” All studies between January 1981 and October 2011 in English were included. Inclusion criteria included patients with an extrauterine pregnancy with a viable neonate in which a complete or partial placenta was left in situ. Prior reviews have identified a total of 163 cases of advanced abdominal pregnancy described in 22 reports, 4 with live births being reported in 109 cases of advanced abdominal pregnancy. 5 Only six studies and a total of nine women with viable neonates were treated conservatively for abnormal invasive placentation.5–10 Reference to breastfeeding or lactation was not mentioned in any of the cases.
A brief review was conducted of placenta accreta in which the placenta was left either whole or in part with viable neonates in which a reference was made to breastfeeding. Breastfeeding and a return to normal menses were noted in one patient with a placenta previa with percreta. 11 Continued breastfeeding at 8 months postpartum was noted in a patient with placenta accreta. 12 Initiation of breastfeeding with the return of normal menses following cessation of breastfeeding was noted in a patient with placenta increta. 13 No reports were identified that defined specifically the pattern of lactogenesis or breastfeeding behaviors.
Adjunctive therapy used in the management of retained or abnormal placentation may include methotrexate or uterine artery embolization, as was used in our patient. Methotrexate is secreted into breastmilk at low levels with a relative infant dose of 0.12%. 14 However, pediatric evidence suggests avoidance of methotrexate during breastfeeding as there is an absence of clear evidence whether any amount of methotrexate may be harmful to the breastfeeding infant. 15 In contrast, the American College of Radiology's Committee on Drugs and Contrast Media has recommended that it is safe for mother and infant to continue breastfeeding after receiving contrast media, 16 as in uterine artery embolization.
Although retained placenta appears to be a causative factor of failed lactogenesis II in our patient, alternate causes must also be considered for her failure of lactation. Postpartum hemorrhage is often cited as a potential cause of lactation failure. 17 The severe risk of maternal morbidity and mortality associated with advanced abdominal pregnancy is often to due significant hemorrhage secondary to the abnormal placentation that is present. Leaving the placenta in situ has been noted to decrease the need for blood transfusions 9 and is being promoted as a potential management option in appropriate patients. As noted above, by leaving the placenta in situ, our patient had minimal blood loss with stable postoperative blood counts, which is thus an unlikely cause of her lactation failure. Although our patient initiated breast pumping on postpartum Day 1 while still in the Cardiovascular Recovery Unit, the frequency of breast pumping sessions and delayed intiation of skin-to-skin contact must be considered as a possible contributing cause. Our patient had a normal return to her menstrual cycle; thus it is unlikely that endocrine or hormonal factors such as Sheehan's syndrome of thyroid conditions were a contributing factor. Additional causes to consider may also have included primiparity, prematurity and maternal–infant separation due to prematurity, maternal physiologic response to stress, and delayed infant suckling.
Conclusions
Advanced abdominal pregnancy is a rare condition associated with high fetal and maternal morbidity and mortality. Management of the placenta depends on the gestational age at the time of delivery, site of placental attachment and vascular involvement, and maternal desire for future fertility. Complications to consider when leaving the placenta in situ include vaginal bleeding, shock, dilatation and curettage, fever, delayed hysterectomy, and lactation failure. Although failure of lactogenesis II may be multifactorial, retained placenta is likely a causative factor. Further research is needed to identify the duration of placental tissue hormone function, the amount of functional placental tissue required to inhibit lactation, and documentation of breastfeeding patterns following management with placental retention.
This report of an advanced abdominal pregnancy in which the placenta was left in situ provides further evidence to the effects of the placenta on lactation. The final decision to leave the placenta in situ is often made intraoperatively. Therefore, it is important to discuss with patients in whom treatment options include leaving the placenta in situ the potential for delayed or failure of lactation prior to the time of delivery.
Footnotes
Disclosure Statement
No competing financial interests exist.