
Abstract
Abstract
Objective:
Human milk has well-established health benefits for preterm infants. We conducted a multidisciplinary quality improvement effort aimed at providing at least 500 mL of human milk/kg in the first 14 days of life to very low birth weight (VLBW) (<1,500 g) infants in the neonatal intensive care unit.
Subjects and Methods:
Improvement activities included antenatal consults with at-risk mothers, staff and parent education, a breast pump loaner program for uninsured/underinsured mothers, pump logs, establishment of a donor milk program, and twice-daily physician evaluation of infants' ability to tolerate feedings.
Results:
The number of infants receiving at least 500 mL of human milk/kg in their first 14 days of life increased from 50% to 80% within 11 months of implementation, and this increase has been sustained for 4 years. Infants who met the feeding goal because they received donor milk increased each year. Since September 2007, infants have received, on average, 1,111 mL of human milk/kg. Approximately 4% of infants did not receive any human milk. Respiratory instability was the most frequent physiological reason given by clinicians for not initiating or advancing feedings in the first 14 days of life.
Conclusions:
Our quality improvement initiative resulted in a higher consumption of human milk in VLBW infants in the first 14 days of life. Other clinicians can use these described quality improvement methods and techniques to improve their VLBW babies' consumption of human milk.
Introduction
Although most of these efforts focus on the healthy full-term infant, feedings of human milk have also been associated with improvements in several health outcomes in preterm infants. These benefits include improved neurodevelopmental outcomes and a decrease in the rates of both late-onset sepsis and necrotizing enterocolitis.7–13 The 2005 American Academy of Pediatrics position statement on breastfeeding and the use of human milk stated that clinicians should recommend the use of human milk in preterm infants. 1
However, for various reasons, mothers of premature infants face multiple challenges in establishing and maintaining an adequate supply of milk. These include delayed lactogenesis stage II, insufficient milk volume, and difficulties in milk expression due to stress or inadequate support. 14 The American Academy of Pediatrics position statement recommended consumption of human milk for premature infants and noted that pasteurized donor milk may be a suitable alternative if a mother's own milk is not available. 1
In addition to the challenges of maintaining the availability of human milk to preterm infants, there are also limitations in delivering the milk due to these infants' immature intestinal motility and digestive function, as well as other complications of prematurity that preclude feeding. 15
Researchers in the neonatal intensive care unit (NICU) at UC Health University Hospital, Cincinnati, OH, conducted a multidisciplinary quality improvement effort aimed at increasing human milk consumption by very low birth weight (VLBW) (<1,500 g) infants. We report here on the results of that initiative.
Subjects and Methods
Setting
UC Health University Hospital is a large, urban academic medical center serving southwestern Ohio, northern Kentucky, and southeastern Indiana. In 2010, the NICU at UC Health University Hospital treated 444 neonates, including 129 VLBW infants.
Improvement team
In the fall of 2005, a multidisciplinary improvement team consisting of physicians, nurses, lactation consultants, and nutritionists was formed. The team began by reviewing the existing literature and determining the primary and secondary factors, called key drivers, 16 believed to be necessary to ensure reliable 17 delivery of human milk to VLBW infants (Fig. 1). Based on a local study that suggested a dose-dependent relationship between human milk volume received in the first 14 days of life in preterm infants and a decreased risk of necrotizing enterocolitis 9 and on animal studies showing histologic and biochemical changes in the intestine with early formula feedings compared with breastmilk, 18 the improvement team established a SMART (specific, measurable, actionable, relevant, and time bound) 19 aim of providing at least 500 mL of human milk/kg in the first 14 days of life to VLBW infants. This goal was believed to be achievable in most VLBW infants based on local feeding practices. Birth weight was used to determine the goal volume. Day of birth was considered the first day of life. The team then developed a set of improvement activities designed to address the key drivers and meet the aim.
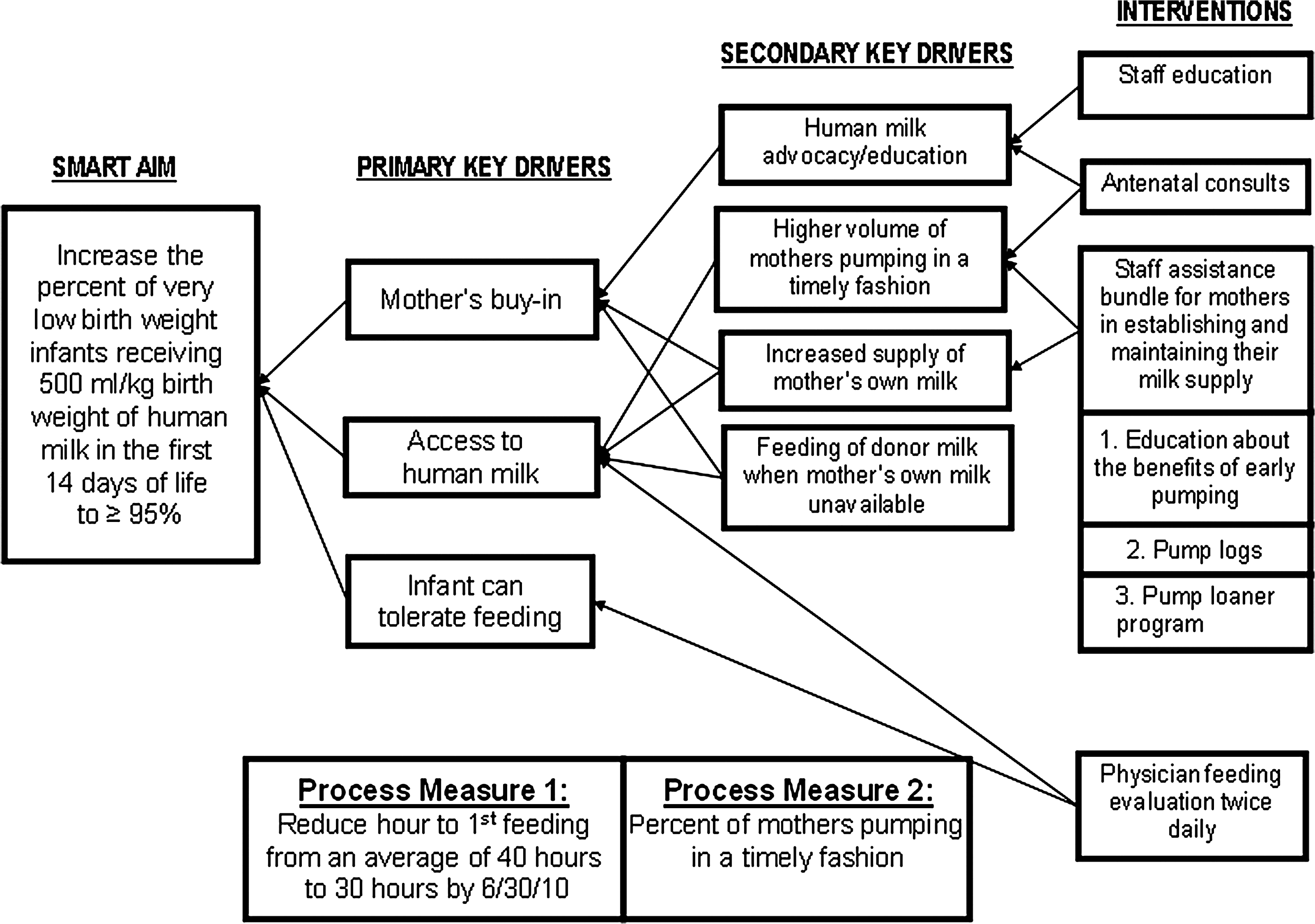
Key driver diagram. SMART, specific, measurable, actionable, relevant, and time bound. Copyright © 2008 Cincinnati Children's Hospital Medical Center.
Improvement activities
• In late 2005, posters were displayed in the NICU describing five improvements in breastfeeding standards: increasing the pumping initiation rate, standardizing the use of colostrum, increasing the volume of human milk delivered, increasing use of pre-breastfeeding activities that support milk volume (such as skin-to-skin contact with the infant, breast massage, and maternal pump logs),14,20 and simplified discharge feeding instructions. Education updates were provided in periodic multidisciplinary newsletters.
• Presentations about the improvement project, the benefits of early initiation of pumping to optimize milk supply, and the new pumps available were made by a lactation consultant (C.A.) to a variety of audiences. These included the nursing department, residents and fellows rotating through the NICU, and the multidisciplinary unit-based NICU design team, consisting of nurses, pharmacists, and respiratory, occupational, and physical therapists. These presentations addressed the importance of staff assistance to mothers in both maintaining and increasing their milk supply and provided sample language that promoted consistent communication about the benefits of mothers' milk to encourage mothers to provide milk for their VLBW infant. Examples included using the term breast pumping, rather than breastfeeding, when encouraging the mother to provide milk. Emphasis was also placed on pumping for a short period, rather than the entire hospital stay, when breastfeeding was not the mother's original goal. Staff were encouraged to remind mothers that their milk served as a “medicine” for their baby that only they could provide.
• A brochure titled Discover the Life-Saving Gift of Your Milk, created by the same lactation consultant and published by the marketing department at UC Health University Hospital, was given to all mothers when their infant was admitted to the NICU. A lactation consultant followed up with a discussion of initiating pumping prior to 24 hours after birth. Mothers were also given another brochure created by the lactation consultant, entitled Tips to Increase Milk Supply, that described interventions to increase milk production should their milk supply be insufficient. (Both brochures are available upon request from the corresponding author.)
• Pump logs were developed for mothers to record when they pumped, for how long, and how much milk was expressed per side. Lactation consultants and nurses used this information to guide additional support.
• The NICU lactation consult form was revised to include an area for the mother to document her milk volume twice a week.
• Meetings with nurse case managers and the medical directors of two Ohio Medicaid health maintenance organizations led to the establishment of protocols for coverage of hospital-grade electric breast pumps.
• Money provided by grants from the Jack J. Smith Jr. Charitable Trust, the Thendara Foundation, and anonymous sources was used to purchase 10 breast pumps and establish a loaner program for uninsured/underinsured mothers.
• A small magnetic alarm clock, set to ring every 3 hours, was attached to the breast pump stand to remind mothers to pump. This intervention was discontinued after 3 months when no increase in pumping frequency was observed.
• Starting in November 2006, pasteurized donor milk was made available for use in the absence of a mother's own milk. This program was initially funded through a grant from Tri-State Breastfeeding Advocates, a member of the Ohio Breastfeeding Alliance, 21 and subsequently by UC Health University Hospital.
• Mothers were given information about the use of donor milk. The superiority of their own milk was emphasized. A small convenience survey of 13 mothers was performed prior to the introduction of pasteurized donor milk to the unit. It revealed that 100% of the mothers would pump even if donor milk was available and that 77% would have consented to use donor milk if the baby was ready to begin feeding but the mother's milk was not yet available. Prior to using donor milk, the physician, lactation consultant, or nutritionist obtained informed consent. Mothers were counseled that donor milk is the preferred alternative to formula if their own supply is insufficient or unavailable. The pasteurization process and the screening process for mothers who donate their milk were described. Our consent form stated that there are no reported cases of disease transmission from a donor milk bank mother to a recipient baby.
• Beginning in March 2010, neonatology fellows and attending physicians who participated in antenatal consults with mothers at risk for delivering prematurely were asked by the improvement team to specifically discuss the benefits of human milk, with recommendations to initiate pumping as soon after delivery as possible.
• Based on preliminary data that suggested that infants who were fed earlier were more likely to meet the feeding goal, physicians began evaluating on rounds each VLBW infant's ability to tolerate feedings. Starting in March 2010, the ability to initiate or advance feeding was recorded on a feeding audit form. Our hypothesis was that, if clinicians specifically evaluated an infant's ability to feed, there would be more opportunities to deliver human milk.
• Also starting in March 2010, a second daily feeding assessment of each VLBW infant occurred on the evening shift. If the infant could not be fed, the reason was documented.
• The criteria for pump initiation were revised in May 2010 to encourage the first session within 6 hours of birth for all medically stable mothers.
Study population
The study population consisted of all infants admitted to the NICU at UC Health University Hospital from January 2006 through June 2010 with a birth weight of <1,500 g. Infants with major congenital anomalies or who were ≥34 weeks of gestation were excluded. Patients who died, developed necrotizing enterocolitis, or who were transferred within in the first 14 days of life were also excluded.
Outcome measures
The primary outcome measure was the percentage of VLBW infants meeting the feeding goal of at least 500 mL/kg in the first 14 days of life. Secondary outcomes included the time to first feeding (measured in hours after birth), the amount of human milk consumed, the reasons infants were not able to be fed, and the effect of personal contact on the mother's interest in pumping.
Data collection
Eligible infants were identified by reviewing the UC Health University Hospital NICU admission log. Data were collected retrospectively. Data on each infant's daily milk intake were obtained via medical record review from January 2006 through June 2010. Time to an infant's first feeding was obtained from the feeding audit form from January 2009 through June 2010. The percentage of infants who could not be fed was obtained from the tracking form from March through June 2010. Data on the influence of breast pumping encouragement and counseling by healthcare workers was obtained from the feeding goal section of the NICU Lactation Consult Form.
Data analysis
Statistical process control charts and run charts were used to examine the impact of the interventions over time.22,23 These charts are commonly used to analyze data from industrial process improvement efforts. They can differentiate common cause variation (causes that are inherent in the process over time) from special cause variation (causes not part of the process, but which arise due to specific circumstances) and evaluate the effectiveness of a change. 24 The upper and lower control limits on the charts establish the margins within which the measurement will be found approximately 99% of the time. An observed change is considered a special cause (statistically significant) when any of the following are true: there is a shift (eight or more consecutive points either above or below the mean or median center line), there is a trend (six consecutive increasing or decreasing points), or there are alternating points (at least 14 consecutive points alternating above and below the mean/median center line). A c (constant area of opportunity) statistical process control chart 22 was used to examine the impact of the improvement activities on the percentage of VLBW infants who met the feeding goal. Data for infants who met the feeding goal were grouped by 10 consecutive births. An X-bar chart was used to examine the change in the amount of human milk consumed. A run chart was used to examine the change in time until first feeding. A Pareto analysis 25 was used to quantify barriers to feeding VLBW infants. Birth weight and gestational age were analyzed using one-way analysis of variance.
Human subject protection
This study was approved by the institutional review boards at Cincinnati Children's Hospital Medical Center and UC Health University Hospital.
Results
In total, 460 eligible infants were included in the study: 120 from 2006, 97 from 2007, 100 from 2008, 97 from 2009, and 50 from the first 6 months of 2010. Mean gestational age of the study infants was 28.6 weeks in 2006 and 2007, 28.5 weeks in 2008 and 2009, and 28.3 in 2010. There were no statistical differences in gestational age between years. Mean birth weights were slightly, but significantly, lower in 2008 and 2010 (p<0.05): 1,115.2 g in 2006, 1,116.7 g in 2007, 1,039.7 g in 2008, 1,142.1 g in 2009, and 1,048.5 g in 2010.
When the project was launched, only 50% of VLBW infants received at least 500 mL of human milk/kg in their first 14 days of life. Within 11 months of implementation, this rose to a median of 80% and was sustained for 4 years (Fig. 2). Following the introduction of the most recent interventions in March 2010 (antenatal consults and twice-daily feeding evaluations), the percentage of VLBW infants meeting the feeding goal remained at or above 80%.
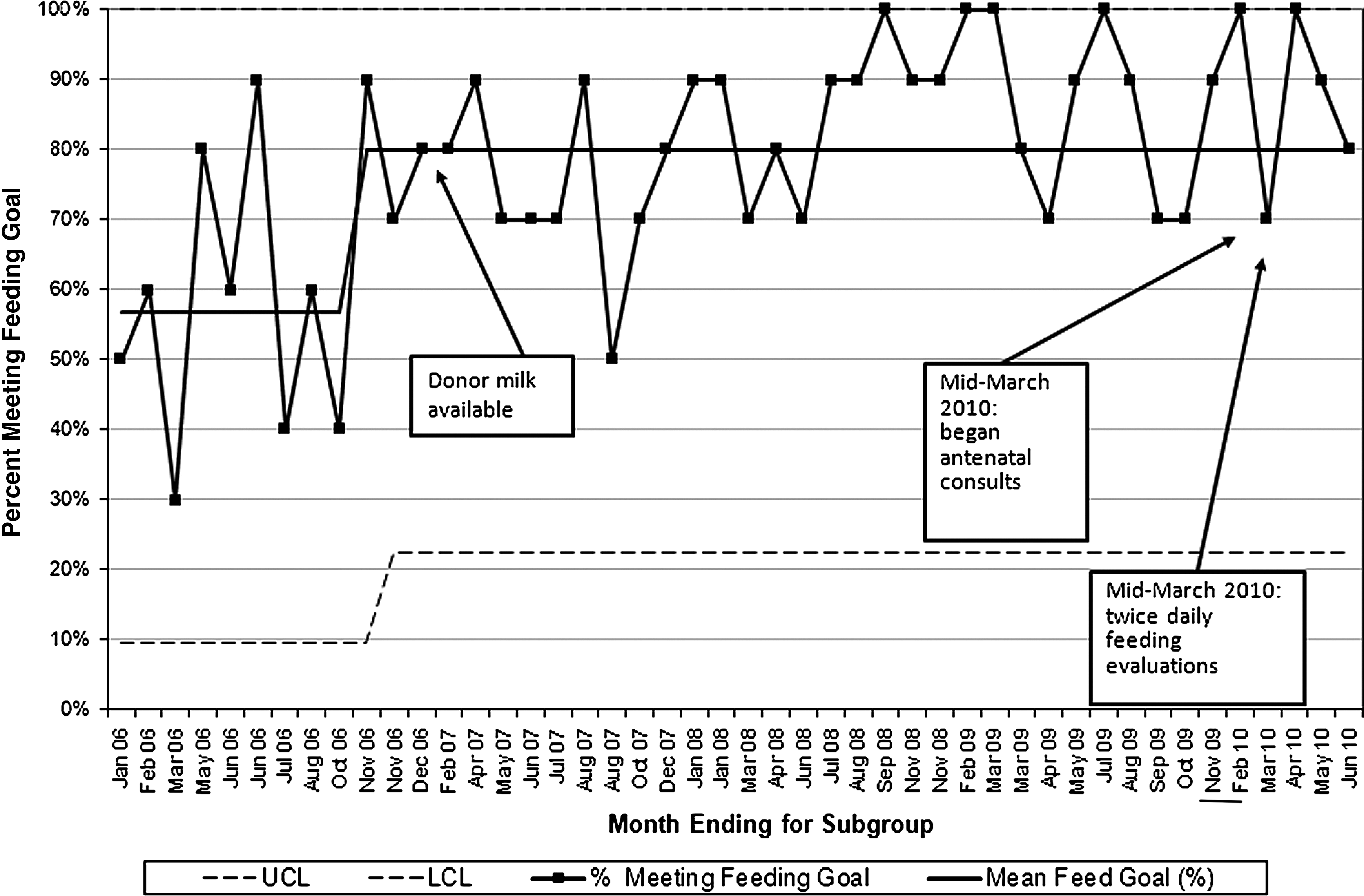
Percentage of patients who met feeding goal, subgrouped by 10 consecutive births. LCL, lower control limit; UCL, upper control limit.
Coaching and counseling by healthcare workers helped to promote milk expression by mothers of VLBW infants, even if breastfeeding was not their original goal. A survey of the first 20 mothers who received the Discover the Life-Saving Gift of Your Milk brochure showed that 71% read it. Of those, 38% said it made them more interested in pumping. Thirty percent of respondents reported an increased interest in pumping based on personal contact with healthcare providers. Furthermore, among the mothers who expressed milk, the percentage who reported pumping as a result of counseling by healthcare workers was 16% in 2006, 29% in 2007, 45% in 2008, 28% in 2009, and 30% in 2010.
The amount of human milk received by the VLBW infants was consistently over the goal, averaging 875 mL/kg from January 2006 through August 2007 and 1,111 mL/kg after September 2007 (Fig. 3).

Average human milk consumption.
The percentage of all infants who were able to meet the human milk feeding goal because they received donor milk was similar each year: 25% in 2007 and 2008, 30% in 2009, and 33% in the first half of 2010. The average donor milk consumption increased each year. It was 73 ounces per month in 2007, 94 ounces per month in 2008, 110 ounces per month in 2009, and 148 ounces per month in 2010.
The time of the first feeding after birth varied considerably during the course of the project, with a mean of 40 hours. However, during each of the first 6 months of 2010, coincident with the implementation of twice-daily feeding evaluations, the average hour of first feeding ranged from 29 to 39 hours.
Approximately 4% of VLBW infants did not receive any human milk during their first 14 days of life, and 8% of mothers did not provide any of their own milk. Over time, as donor milk became more available and counseling became more successful, we found that lack of human milk was no longer a reason why infants did not meet the human milk feeding goal and that it was the infant's medical condition that precluded feeding (Fig. 4). At 24%, respiratory instability was the most frequent physiological reason given by clinicians for why these infants could not be fed. Other common reasons were gastric aspirates, patent ductus arteriosus treatment or prophylaxis with indomethacin, and the presence of umbilical catheters.
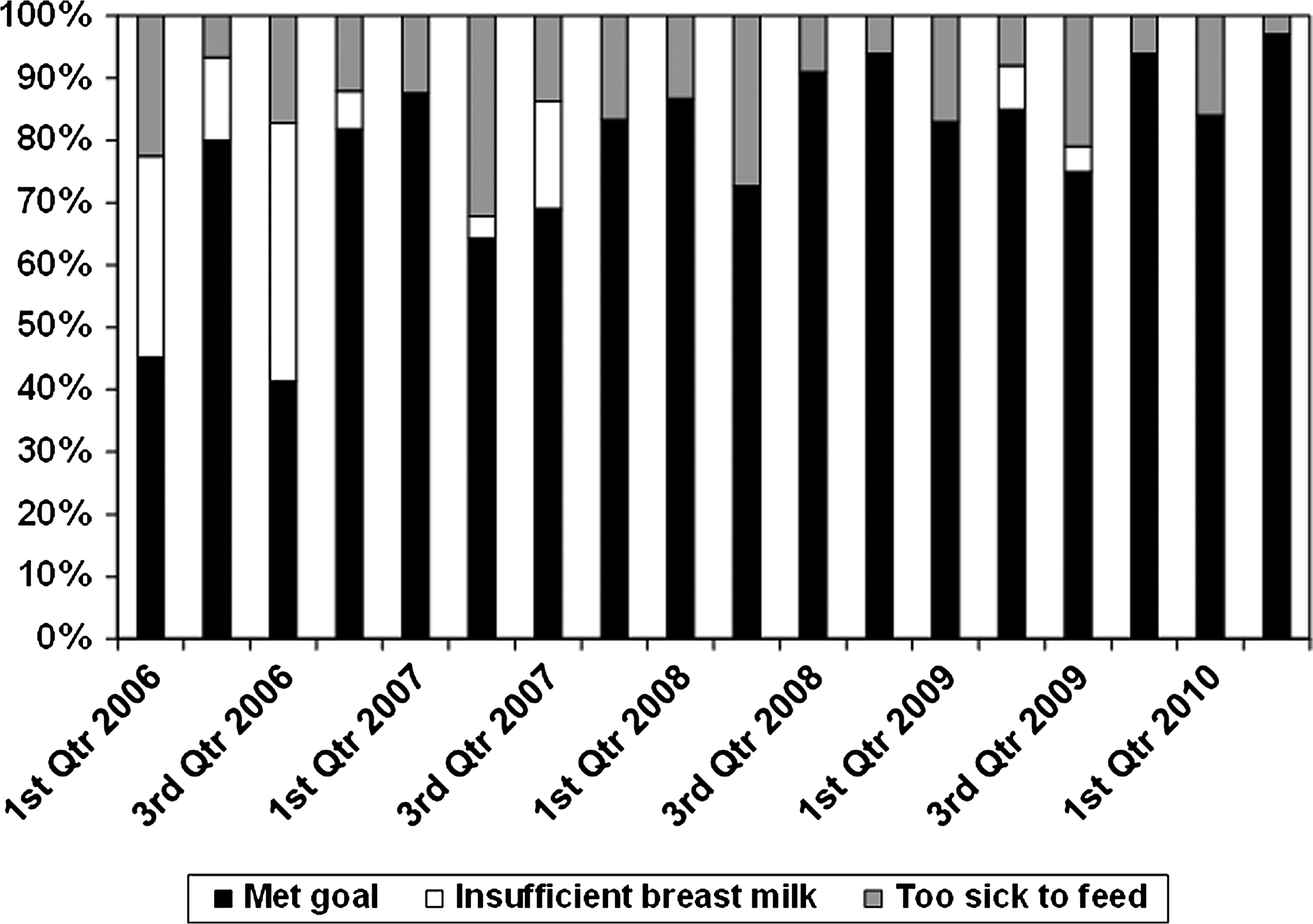
Reasons for infants not meeting breastmilk feeding goal of >500 mL/kg in the first 14 days of life. Qtr, quarter.
Discussion
Human milk has well-established health benefits for preterm infants.7,8,10,13 Providing feedings of human milk is an evidence-based strategy for prevention of morbidity and mortality in this population. Our quality improvement initiative resulted in a higher consumption of human milk in VLBW infants in the first 14 days of their life. Over time, we have found that the culture of our NICU has changed in that human milk has become the food of choice in this vulnerable population.
The literature shows that encouragement by healthcare professionals can have a major impact on a mother's decision to breastfeed.26–28 The results of our study are consistent with a recent systematic review and other studies that found that human milk feedings in the NICU are promoted by multidisciplinary staff training.26,27,29–32 We found that some mothers would agree to pump on our recommendation, even if breastfeeding was not their original goal. We also found that most mothers would consent to donor milk if they did not intend to pump or if their own milk supply was insufficient. The availability of donor milk had a big impact on our project, with approximately 25% of babies meeting the human milk feeding goal because of donor milk.
Early initiation of nutrition support, consisting of both parenteral nutrition and limited or minimal enteral feedings, in preterm infants has been associated with a rapid regain of the initial weight lost, improved weight gain, earlier achievement of full enteral feedings, reduced systemic sepsis, and a shorter hospital stay.33,34 Once the supplies of human milk were consistently adequate to meet the needs of our VLBW infants, we began to focus on the challenge of milk delivery to promote earlier feeding. Our more recent interventions focused on improving opportunities to feed infants who were otherwise being missed, as well as learning about the factors that prevent us from feeding them. Although we have fed babies earlier with these interventions, significant morbidities, such as respiratory difficulties and feeding intolerance, so common in this population, still preclude feeding. Therefore, consistently meeting our goal of feeding 90–95% of these infants will remain difficult.
We encourage mothers to initiate pumping and manual expression within hours of giving birth. However, many mothers of VLBW infants have delivered by cesarean section, and some have additional complications, such as requiring a 24-hour course of magnesium sulfate after delivery. In addition, at the time of delivery, many of these mothers may not have considered expressing their milk. All these issues contribute to the difficulty of initiating early pumping.
Although our measures covered just the first 14 days of life, significant challenges remain for mothers of VLBW to maintain their milk supply throughout the infant's hospital stay. A variety of factors influence a mother's ability to produce milk and breastfeed a premature infant, including infant health complications, 35 cultural background or race, 36 socioeconomic status, 36 maternal education, 37 and maternal age. 38 Provision of mother's own milk is also likely to be mediated by counseling that conveys the importance of human milk feeding to prevent devastating diseases, instrumental support (such as provision of a pump to provide the mother's own milk), maternal self-efficacy regarding her milk, comfort with human milk feeding, and lack of comfort with formula feeding. 26 Although the availability of donor milk played a significant role in our success and there are clear benefits of donor milk compared with formula feedings,39,40 unanswered questions regarding its use remain. A mother's own milk may be the best immunologic match to the infant's needs and increases the mother–infant bond, and it is not known whether the use of donor milk affects a mother's motivation to produce her own milk and sustain lactation. In addition, at approximately $4.30 per ounce, donor human milk is costly.
This was a retrospective review of quality improvement interventions at a single NICU. However, the improvements observed for this sample of VLBW infants are very encouraging. Our future steps will ultimately include providing education and counseling on the benefits of human milk to women earlier in their pregnancy, possibly even preconception. Although we have been targeting high-risk mothers who are threatening to delivery preterm, we plan to counsel this population prior to the stressful time of admission. In addition, given the unique properties of mother's own milk and benefits to both mother and baby, we plan to continue to pursue further measures that may improve earlier onset of a copious supply of mother's own milk.
Footnotes
Acknowledgments
Money provided by grants from the Jack J. Smith Jr. Charitable Trust, the Thendara Foundation, and anonymous sources was used to purchase 10 breast pumps and establish a loaner program for uninsured/underinsured mothers. The funding sources had no involvement in the study design; collection, analysis, or interpretation of the data; writing of the report; or decision to submit this article for publication.
Disclosure Statement
No competing financial interests exist.