
Abstract
Abstract
Objective:
We hypothesized that pooling a mother's expressed breastmilk for 24 hours compared with individual pump session collection of milk would provide a more consistent caloric product without increasing bacterial contamination.
Study Design:
We investigated 24-hour pooled breastmilk collection by enrolling 19 mothers who were expressing milk for their infants. Mothers followed a standardized milk collection protocol for 4 study days: daily milk was pooled in a sterile 1-L bottle on Day 1, and on Day 2 milk was aliquoted for each pump session into a sterile 120-mL container. The next week the order of collection was reversed. Milk samples were plated, incubated, and evaluated for bacteria colonization. Milk samples were analyzed for protein, fat, and carbohydrate content.
Results:
There was inherently less variability in the caloric and nutrient content of pooled milk compared with individual samples, in which caloric density varied by as much as 29%. Mother's milk had highly variable bacterial counts ranging from 0 to greater than 100,000 colonies/mL. High bacteria counts (>100,000 colonies/mL) occurred in 14.7% (31 of 211) of individual samples compared with 8.6% (three of 35) of pooled samples (p=0.39).
Conclusions:
Twenty-four-hour pooling of human milk reduces nutrient and caloric variability without increasing bacterial counts.
Introduction
There is an inherent variability in nutritional content of expressed milk between individual pump sessions. 4 As a result, current collection practices could lead to a marked variation in nutrient content of individual feeds for VLBW infants. Both pathogenic and probiotic bacteria are found in human milk, and proper milk handling is recommended to minimize pathogenic bacterial growth.5,6 However, in current NICU practice, milk is subject to multiple transfers between containers, exposures to open air, and numerous changes in temperature from the point of pumping to feeding of the preterm infant.
In this study, we hypothesized that pooling mother's own milk for 24 hours would provide a more consistent nutrient content feeding and ease mother's work load without leading to an increase in bacterial content in milk.
Subjects and Methods
Study subjects
Between February 2009 and February 2010, we enrolled a convenience sample of 19 mothers who had infants born at the University of California San Diego Medical Center in a pilot study to investigate 24-hour pooling of expressed breastmilk. All study mothers had ill or premature infants who were dependent on gavage feedings. Mothers were pumping with electric breast pumps at home and hospital-grade electric breast pumps in the hospital. The University of California, San Diego, Human Research Protection Program approved the study protocol.
Milk collection
Study mothers were given instructions in pump kit cleaning and milk collection methods. (Table 1). They received microwave steam bags, cooler bags, and gel cooling packs to standardize pump kit cleaning and milk transport. Mothers were provided with sterile, bisphenol-A-free, 1-L polypropylene plastic bottles (Medela, Inc., McHenry, IL) and 120-mL sterile bisphenol-free polypropylene collection cups (Premium Plastics, Inc., Chicago, IL) for milk storage. Mothers were instructed to pump into their own clean pump kit bottles and then decant milk into a collection container. They were instructed on the first study day to pool all milk for 24 hours in the 1-L bottle (POOL collection). Mothers were told to pour each pumped milk collection directly into the 1-L bottle, place it in the refrigerator, and continue to add freshly pumped milk to the bottle over the 24-hour time period. On the second study day, the milk was individually collected for each pumping session (IND collection) and refrigerated in 120-mL collection cups as is the standard practice in our NICU. The following week the collection was repeated in a reversed order of collection (i.e., IND, then POOL). Thus, each mother collected 4 days worth of refrigerated milk for analysis. Mothers brought refrigerated milk directly from their home refrigerator to the NICU in a standardized cooler bag with a gel ice pack. Milk collections were weighed and then agitated by hand. Milk samples (1 mL for bacterial culture, 3 mL for macronutrient analysis) were obtained from all collection containers. The remainder of the milk was divided after gentle agitation into aliquots for feeding or freezing. Milk was processed within 24 hours of completion of daily collection.
Bacterial culture methods
One-milliter samples from the IND and POOL collections were refrigerated until plating the same day. Samples were processed by plating 1 μL on each of three plates: sheep blood agar, colistin-naladixic acid agar, and MacConkey's agar. These plates were incubated for 48 hours at 35°C in CO2. The value for colony-forming units per milliliter (cfu/mL) was determined by counting the number of colonies and multiplying by 1,000. Resolving differences between samples based on number of counts at below 100,000 cfu/mL was likely to be inaccurate, and therefore such samples were not analyzed. We were not addressing the question of pathogenic versus nonpathogenic bacteria and thus elected not to speciate bacterial isolates.
Macronutrient analysis
Three-milliliter samples from the IND and POOL milk collections were warmed to 40°C on a dry digital heating block. A 1-mL aliquot was placed onto a transflectance cup in a near-infrared spectrophotometer (SpectraStar™ 2400; Unity Scientific, Inc., Columbia, MD) for analyses of fat, protein, and carbohydrate. The near-infrared spectrophotometer method was validated in a previous article 7 where paired human milk samples were measured by near-infrared spectrophotometer and reference chemistry to calibrate the machine to r2 values greater than 0.9 for total protein, fat, and carbohydrates. Calories were calculated according to the following equation: total calories (in kcal)=(protein [in mg/dL]×4)+(fat [in mg/dL]×9)+(carbohydrate [in mg/dL]×4). 8
Maternal satisfaction
Subject mothers were asked to complete a satisfaction questionnaire regarding 24-hour pooling of milk. They were asked to compare the two collection containers and choose whether they liked the 1-L bottle, 120-mL cup, or both.
Statistical analysis
Sample size calculations were based on a clinically relevant 20% reduction in total calories with a power of 0.8 and α of 0.05 based on our previous study. 7
Descriptive statistics (frequency and arithmetic medians) were used to summarize demographic data. The arithmetic mean and the SD were calculated for nutrient content (protein, fat, and carbohydrates) data of all milk samples. Nutrient content for IND and POOL collections were compared using an independent t test. The χ2 test was used to compare differences in the number of high bacterial counts (defined as >100,000 cfu/mL) in IND and POOL collections. Survey results were reported as the frequencies of each response. Statistical significance was considered for a p value of <0.05.
Results
We collected a total of 35 POOL and 219 IND paired milk collections from 19 mothers. Two mothers provided only one paired (IND and POOL) milk collection because their infant was discharged prior to the second collection period. There was one incomplete data pair with IND but no POOL information. Mothers delivered infants at a median gestation age of 28.7 weeks (range, 24.9–38 weeks) with a median birth weight of 1,020 g (range, 630–2,825 g). Infants were a median 40 days of life (range, 15–118 days) when mothers provided the first study sample. Median maternal age was 29 years (range, 21–44 years). The median 24-hour milk production was 788 g (range, 221–1,718 g).
Bacterial colonization
Mother's milk samples had highly variable bacterial counts that ranged from 0 to >100,000 cfu/mL. Although bacteria counts over 100,000 cfu/mL occurred more frequently in the IND samples, this difference was not statistically significant (8.6% of POOL samples [three of 35) vs. 14.7% of IND samples [31 of 211], p=0.39).
Content analysis
One set of milk samples (POOL and IND) was lost during processing. The mean macronutrient content for all samples (ALL), IND, and POOL was similar (Table 2). However, over the course of the day, there was considerable variability in IND samples (Fig. 1). The range of variability of individual macronutrients for all mothers, taken as 2 SD, was±32% for protein,±46% for fat,±30% for carbohydrate, and±29% for total calories from the means.
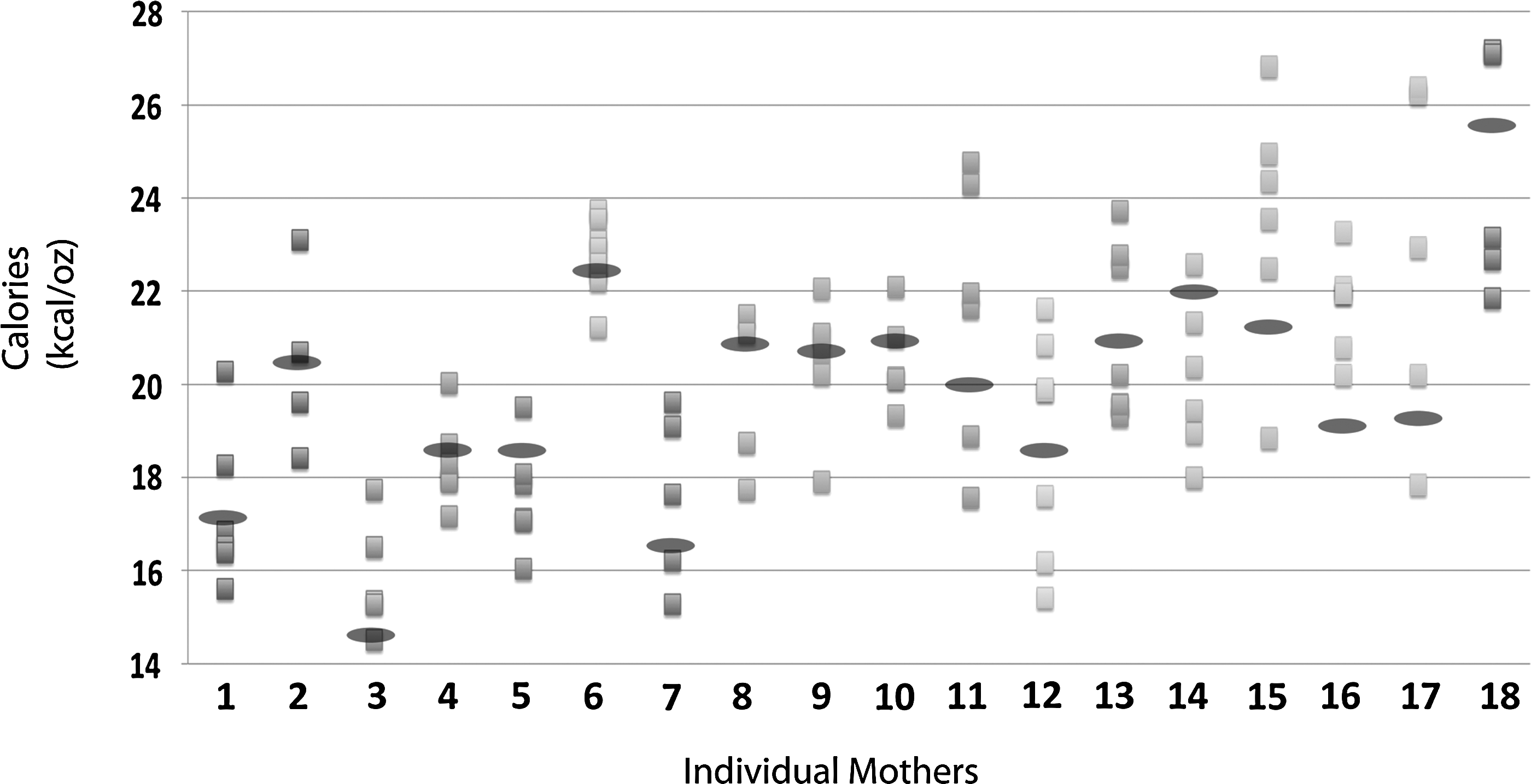
Caloric content of 18 mothers' individual and pooled milk collections. A single set for each mother is shown. The pooled and individual collections are represented by ellipses and squares, respectively.
Data are mean±SD values. One set of milk samples (pooled [POOL] and individual [IND]) was lost during processing. The mean macronutrient content for all samples (ALL), IND, and POOL was similar.
Maternal satisfaction
Fifteen mothers (79%) responded to our questionnaire; results are summarized in Table 3.
Mothers were asked to rank their preference for different milk storage containers (n=15; four mothers did not return questionnaire).
Discussion
Human milk use in the NICU is increasing as evidence grows for the benefit to the VLBW infant.9,10 Providing optimal milk quality and support of the pumping mother are important aspects in managing preterm infant nutrition. 11 Hospitals have traditionally recommended that milk from each pump session should be individually stored, but this approach has not been validated. 2 Furthermore, the merits of 24-hour pooling of mother's own milk have not been examined in the clinical environment. We found that a single daily pooling strategy provides several important benefits—consistent nutrient quality, equivalent bacterial content, and improved maternal satisfaction—over individualized collection.
Macronutrient content
Nutritional content of human milk is thought to vary depending on differences in pumping fraction (hindmilk vs. foremilk), time of day, day of lactation, and degree of breast emptying.4,12,13 Indeed, low calorie foremilk may contain as little as 12 kcal/ounce, with high calorie hindmilk having as much as 30 kcal/ounce. 7 Moreover, individual samples can vary substantially in fat, protein, and carbohydrate content. In the current study, for example, one mother produced milk that varied in caloric density between 14 and 28 kcal/ounce. Although perhaps inconsequential for the nursing child, the variability in calorie content may pose significant problems for the premature infant, who often receives a full day's feeding from only one pumping session. Single daily pooling not only eliminates the variability in nutrient composition and content, but also may improve feeding tolerance of the immature intestine.
Pooled samples also provide more reliable estimation of nutrient content. Optimizing nutrient delivery to the premature infant is important for somatic and brain growth because in utero growth accretion rates are difficult to achieve. 14 We found that a single pump session differs substantially from a mother's average 24-hour nutrient content, leading to inaccurate nutrient and calorie supplementation for the high-risk infant. Mother's milk analysis in real time has been proposed to improve nutritional delivery by allowing tailored fortification.15–17 Daily pooled collection would allow accurate measurement and more consistent nutrient composition in day-to-day feedings.
Transfers of milk (from pump bottle, to storage container, to fortification container, to feeding syringe) can result in loss of fat and calories. Sixteen percent of calories can be lost by fat adherence to tubing in the feeding apparatus alone. 18 By minimizing these manipulations, 24-hour milk pooling may help maintain caloric density.
Bacterial content
Human milk contains the mother's bacteria, which are passed to the infant with feeding. But, human milk also has properties that mitigate bacterial growth over time when the milk is refrigerated, and a recent study regarding milk cultures and infant illness concluded that routine milk cultures are not predictive of infant infection.19,20 Although pooling milk eliminates nutrient variability, it might also increase bacterial growth. However, we found that most pooled milk had no more bacteria than individually collected samples, even after multiple entries into the larger container.
Maternal perceptions
Mothers of NICU infants struggle with the work load of pumping, labeling, storing, and transporting multiple small containers of milk. Many mothers have problems with low production, which can be compounded if they are not able to track their daily milk volumes.21,22 A single bottle with volume markers (unlike our prototype, which did not have markers) would provide a reliable method for estimates of milk volume. Our mothers preferred the pooled method for overall ease of use and transporting milk to the hospital. Mothers also commented that it was easier to label only one container, took up less space in their refrigerator, and was easier for the nurse to log in the milk. They preferred the smaller containers for tracking their pumped milk volume and for storing milk in the hospital. Because most milk used in the hospital is frozen and must be used within 24 hours of thawing, mothers feared that freezing large amounts of milk could lead to milk being discarded.
Suggestions for future study
Further studies should address whether collection method, cold storage, and travel time contribute to differences in bacterial growth rates and to milk colonization by Gram-positive or Gram-negative bacteria. The limitations of this study were the small sample size and the inaccuracies inherent in a study involving home collection of mother's milk and unsupervised cleaning of each mother's pump kits. Although we found bacterial counts to be low in most milk samples, further study analyzing pathogenic bacterial growth in mother's milk may be helpful.
Hospital guidelines for using a pooled milk container would need to be developed. Evaluation of the practicality of pooling all milk, encouraging use of fresh milk, and minimizing milk transfers would be very useful for the NICU setting. Based on our study, we suggest that mothers would pool a 24-hour milk collection every day. After freezing milk that exceeds the infant's daily milk requirement, mothers would transport the 24-hour feeding volume of fresh milk to the hospital for fortification, aliquoting, refrigeration, and use within 48 hours. For most mothers, a large container would not be practical for long-term storage of frozen milk. Hospitals often struggle with safe milk handling, dealing with numerous containers, storage issues, and prevention of wrong milk/wrong baby errors. 23 A large container that would allow fresh milk to be labeled, measured, fortified, and allow feedings to be drawn or poured from the same vessel may be a safer alternative to current practice.
Conclusions
Twenty-four-hour pooling of expressed mother's milk minimizes variation in nutritional content and simplifies milk handling for the mother without increasing bacterial growth.
Footnotes
Acknowledgments
The authors would like to thank the study mothers for their participation. One-liter milk bottles were produced and provided by Medela, Inc. for this project.
Disclosure Statement
J.H.K. and L.M.S. have received a past unrestricted research grant, breast pumps, and honoraria for educational lectures sponsored by Medela, Inc. Y.E.V., C.S.C., and T.D.M. have no competing interests to report.